United Nations, Department of Economic and Social Affairs, Population Division. 2013.
Living and Dying Well: A National Action Plan for Palliative and End of Life Care in Scotland. 2008;
The Scottish Government.
Scottish Health Survey 2012.
Gluzman R, Katz RV, Frey BJ, McGowan R Prevention of root caries: a literature review of primary and secondary preventive agents. Spec Care Dentist. 2013; 33:133-140
Cancer Research UK.
Marrie TJ Pneumonia in the long-term-care facility. Infect Control Hosp Epidemiol. 2002; 23:159-164
van der Maarel-Wierink CD, Vanobbergen JN, Bronkhorst EM, Schols JM, de Baat C Risk factors for aspiration pneumonia in frail older people: a systematic literature review. Am Med Dir Assoc. 2011; 12:344-354
van der Maarel-Wierink CD, Vanobbergen JN, Bronkhorst EM, Schols JM, de Baat C Meta-analysis of dysphagia and aspiration pneumonia in frail elders. J Dent Res. 2011; 90:1398-1404
McGrath C, Bedi R The importance of oral health to older people's quality of life. Gerodontology. 1999; 16:59-63
Walls AW, Steele JG The relationship between oral health and nutrition in older people. Mech Ageing Dev. 2004; 125:853-857
The francis report – implications for oral care of the elderly Nicholas Beacher M Petrina Sweeney Dental Update 2024 42:4, 707-709.
Authors
NicholasBeacher
BDS, MFDS RCPSG
Clinical Lecturer in Special Care Dentistry, Glasgow Dental School, School of Medicine, College of Medical, Veterinary and Life Sciences, University of Glasgow, UK
Senior Lecturer/Honorary Consultant in Special Care Dentistry. Glasgow Dental School, School of Medicine, College of Medical, Veterinary and Life Sciences, University of Glasgow, UK
Oral health is an essential, yet often neglected, aspect of care in the elderly population. A mouth free of pain and disease which is functional, comfortable and aesthetic improves quality of life. Following the shocking reports of patient neglect and abuse published in the Francis Report, the dental profession must acknowledge that there are longstanding deficiencies in the provision of oral healthcare for the elderly, whether residing in care homes, hospitals or at home with support. It must be a universal goal to improve the care provision for this population through developing a greater understanding and overcoming the multi-factorial barriers to care. This article will highlight the key features of the Francis Report and its significance in the context of oral healthcare provision for the elderly.
Clinical Relevance: To provide insight into the oral healthcare needs of the growing elderly population and the necessity of dealing with the current limitations in service provision.
Article
The Francis Report is arguably the single greatest invitation for change in the provision of care in the history of the NHS. The pages of the Report reveal case after case of abuse and neglect from those who were educated to, and entrusted with, care for fellow human beings when they were at their most vulnerable.1 The incomprehensible conduct of healthcare professionals and their managers occurred repeatedly to the point where it became accepted as normal. In its effort to be a business, the crown jewel of the nation, the NHS, failed its patients and their loved ones at every level.
The dental profession cannot hide from the stark and uncomfortable truths laid out in the Francis Report. We, too, have grown to accept the deficiencies in the oral and dental care provided for our elderly population. We have neither addressed the existing significant disease burden nor how we manage it. As we stand on the threshold of a new post-Francis era of healthcare, the profession must strive to meet the oral healthcare needs of our ageing population with patients at the very centre of care.
Clinical considerations
An ageing population and its challenges
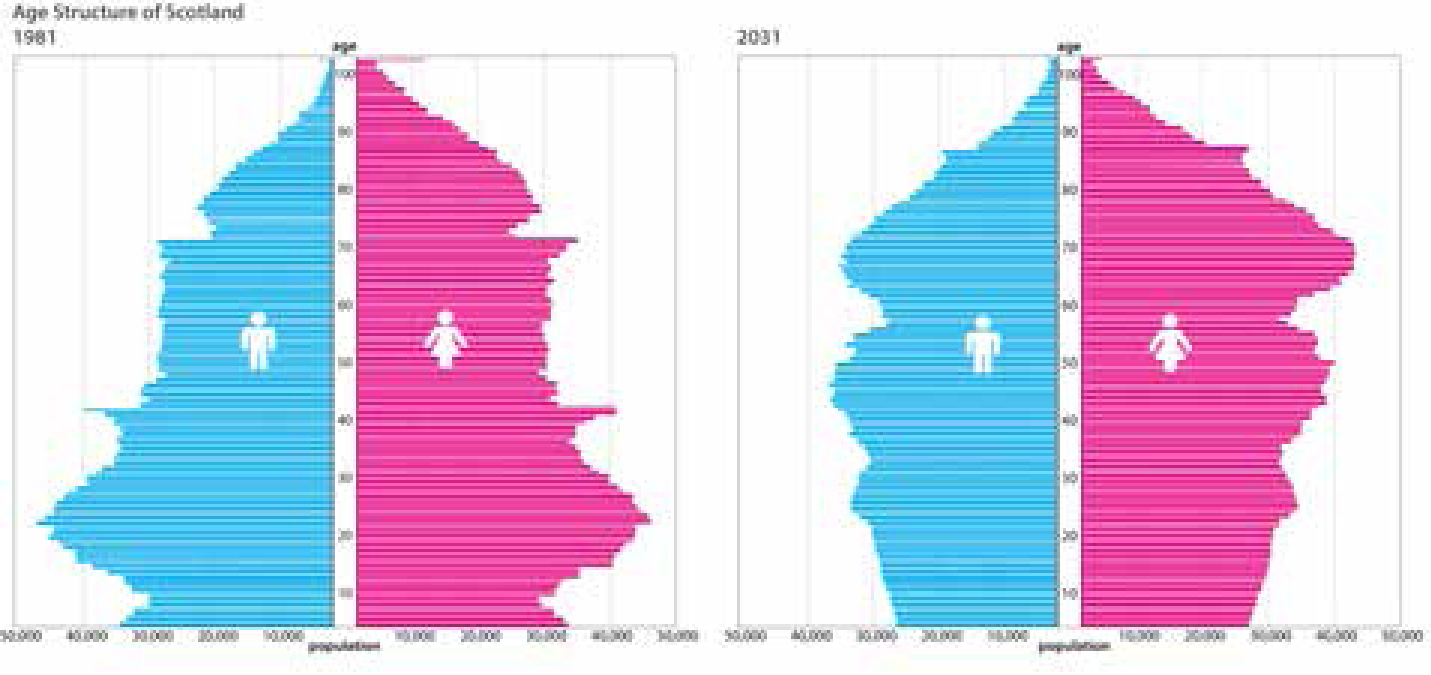
The United Kingdom has an ageing population,2 a demographic shared with other developed nations.3 Data from Scotland illustrates clearly the predicted population change from 1981 to 2031, with a notable increase in longevity and increased median age of the population4 (Figure 1).
Figure 1. Population pyramids for 1981 and (projected) for 2031, demonstrating the significant demographic shift towards an increasingly elderly population.
Advancing medical care and medications
In addition to improved social conditions, the increase in life expectancy is partly due to the enhanced capabilities of modern medicine. Improved medical care has prolonged life, but often at the cost of living with chronic illness. It is predicted that 66% of the Scottish population will be living with a chronic condition by 2035.5 This has implications for both individuals and healthcare systems as demand upon resources increases.
As people live longer, they are more likely to require prescribed medications, and polypharmacy is very common in the elderly. This has oral health implications, for example oral side-effects of medication (Table 1), and makes the delivery of dental care increasingly more complex and demanding.
Xerostomia
Gingival enlargement
Lichenoid reactions
Angioedema
Taste alteration
Pigmentation
Dementia
Dementia is a syndrome which may be chronic or progressive, resulting in decreased cognitive function beyond that which might be expected of the normal ageing process. Alzheimer's disease is the most familiar type though other forms, including cerebrovascular and Lewy Body, are also common in the elderly. Estimates suggest that less than half of those living with dementia in the UK have a formal diagnosis. Such significant under-reporting may present itself at a later stage as we struggle to meet the expectant healthcare needs of our nation.
Dementia raises many issues for oral health, including daily provision of preventive oral healthcare, communication issues, capacity to consent and co-operation to permit treatment.
Retention of teeth
People are retaining their natural dentition for longer. The most recent Scottish data revealed that 54% of those aged 75 and over had some teeth remaining.6 Complex restorative dentistry is increasingly prevalent. Restorations such as multi-unit bridges and implants, often placed earlier in life before disability developed, pose huge challenges for those no longer able to self-care and maintain the excellent oral hygiene that is a fundamental necessity for such fixed prostheses.
The Francis Report
The vast report is but words on a page until a personal connection can be made to the events it describes. The transcripts describe real people who suffered terribly at the hands of the NHS. The elderly are not people ‘past their expiry date’ and cannot simply be left to ‘go off’. They have journeyed the path of life as we do now and experience the very same feelings and emotions as every other individual. Let's look at some of Robert Francis’ conclusions in the context of oral healthcare for the elderly:
‘Too great a degree of tolerance of poor standards’
The Francis Report continually exposes the reader to harrowing cases of neglect, in which poor standards of care were normalized and became accepted. The uncared for and heavily diseased mouth is regrettably a familiar sight to the dental practitioner who provides care for those older people who are dependent upon others. A case managed by one of the authors highlights such neglect:
“An elderly gentleman resident in a long-stay specialist unit for care of the elderly, who was fully dependent upon others for personal care, was prescribed ferrous sulphate tablets. He had a profoundly dry mouth and a mild dysphagia secondary to stroke disease. The attending dentist was asked to assess the patient because he had developed a painful, ulcerated mouth with a facial swelling over the right mandible (Figure 2a, b). This patient had been unable to swallow the iron tablets and as a result of his stroke they were accumulating in his lower right buccal sulcus. Iron tablets cause tissue necrosis and had produced gross ulceration in the buccal sulcus, which resulted subsequently in a septicaemia. There is no doubt that if daily oral healthcare measures had been in place, this event would have been avoided. Simply performing an oral sweep of the mouth and changing his prescription to a liquid form of iron would have averted such a traumatic and life-threatening event.”
Figure 2.
(a) Extra-oral and (b) intra-oral views of an elderly hospital patient with an extensive iron burn.
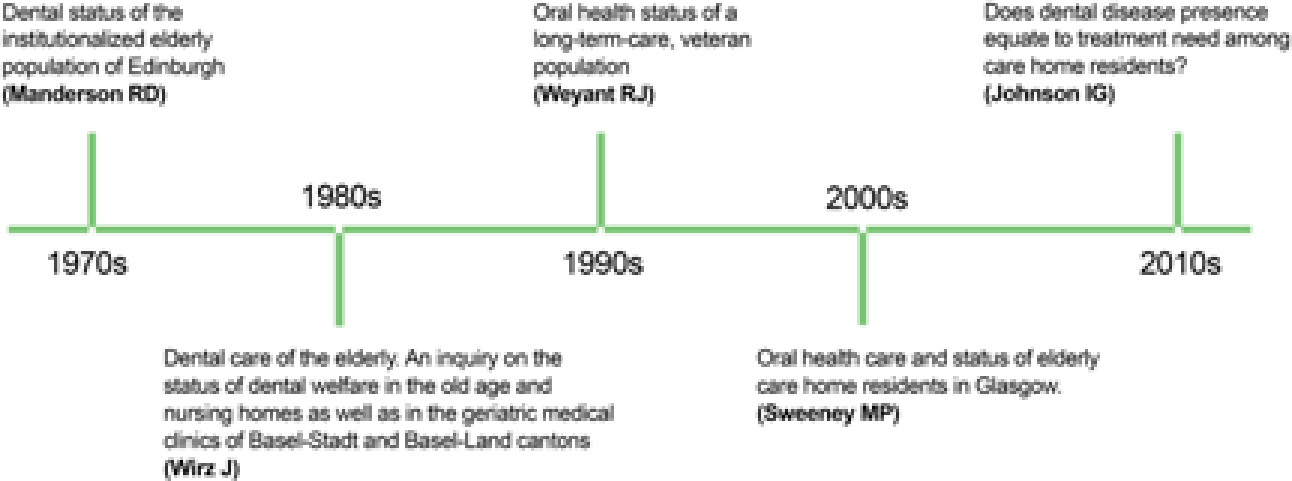
So why do we tolerate such neglect? The scientific literature provides little reassurance that the dental profession has advanced in its care of the elderly in recent years. A snapshot of the few existing research studies undertaken in this group of patients repeatedly highlights the lack of oral healthcare for the elderly (Figure 3). The scientific evidence of poor standards of care is all too clear – we need to develop evidence-based models of care that will correct the inadequacies of current practice.
Figure 3. A timeline of oral health research showing consistent deficiencies in oral care for the elderly.
The oral pathologies affecting the older person's mouth are very familiar to dentists. Caries, particularly root caries which affects 30–60% of older people,7 periodontal disease and oral mucosal disorders are common. As awareness of oral cancer improves, it is appropriate to draw attention to the fact that 20% of oral cancers diagnosed in the United Kingdom are in those aged 75 and over.8 Unfortunately, these patients often present late, highlighting the need for regular dental examination in addition to the daily routine assistance which may be required by those unable to self-care. Supported assistance with oral hygiene presents an opportunity for carers to observe the oral mucosa and arrange for dental assessment as appropriate.
‘And they must be protected from avoidable harm’
Francis was very clear in his Report that the inherent principles of patient-centred care must emerge into the foreground as the NHS moves forward. The NHS is the people's healthcare establishment, charged with providing the highest standards of care, clinical excellence and professionalism. If such high standards are set, then it is imperative that measures are taken to avoid harm across the service, including the dental profession. Oral disease has an impact on systemic health, for example in relation to aspiration pneumonia, a significant cause of death for those residing in long-term care homes.9 The mouth is the primary source of bacteria responsible for aspiration pneumonia. In the neglected mouth the bacterial load is increased and thus the reservoir of pathogenic micro-organisms is greater, increasing the risk of aspiration pneumonia.10,11 Simple measures, such as ensuring a clean and healthy mouth for an older person, helps to protect them from harm and the dental profession needs to be leading the way.
Berwick,12 in his response to the Francis Report, gave further credence to not only the role of healthcare professionals, but also to the associated members of the NHS team from top to bottom as guardians of patient safety:
‘Patient safety should be the ever-present concern of every person working in or affecting NHS-funded care.’
Dental healthcare professionals represent a significant component of the NHS and have an important part to play in delivering the patient-safety agenda:
‘And they must be protected from avoidable harm and any deprivation of their basic rights’
Human rights embody equality. Parity is not a natural phenomenon and thus the fundamental rights which we take for granted are not omnipresent in our society. To date, care of the elderly, including oral healthcare, has not been delivered in an equitable manner and it is timely to remind ourselves of some key articles of The United Nations Convention of Human Rights. Each has relevance to care of the elderly:
Article 5: ‘No one shall be subjected to degrading treatment’
The frequency with which degrading treatment was observed in the Francis Report is both unnerving and inexcusable. Those who put their trust in the care of the NHS were let down. One of the transcripts produced as evidence in the Report highlights the importance of caring for the mouth and how the most basic of caring principles, when lost, can be devastating to those who are vulnerable and dependent upon others for care:
‘A lady of 95 years who was registered as blind and diabetic and suffering from pneumonia was left to sit in a corridor in A & E at Stafford Hospital for three hours. The care, when it was eventually provided, was good. The next day the patient was transferred to Ward 10 where she was left in soiled bed clothes and no one answered when she rang her call bell for help. When the patient's false teeth were lost she was assured that the dental department would provide a new set, yet weeks later she was told such a service was not available. The food provided to the patient was not suitable for a lady with no teeth and despite being blind, staff offered her no assistance with feeding. For the patient's entire stay, which was several weeks, she was not washed or cleaned.’
It is prudent to reflect that Mid-Staffordshire Hospital does not stand alone in its neglect of care. In February 2007, an 87-year-old lady called Mrs McGaw died in a Scottish hospital following her admission from a care home after becoming acutely unwell. Her general medical practitioner acknowledged that the lady's condition was deteriorating and suspected an oral cause. An inquiry was established to investigate the death of Mrs McGaw. Her primary cause of death was reported as ischaemic heart disease but her oral condition raised serious concerns. It is believed that her denture might have been left in her mouth for a period in excess of two weeks and a body of opinion from the medical witnesses believed it quite likely that the denture contributed to Mrs McGaw's death.
Article 21.2: ‘Everyone has the right of equal access to public service in his country’
The NHS is arguably the United Kingdom's greatest achievement as a public service and is a source of much pride to the nation's people. However, of late it has been subjected to sequential negative stories. The NHS is quoted as ‘belonging to the people’, which includes the elderly. We need to take responsibility for removing the barriers currently inhibiting their access to the care they require, which for dentistry includes mobility and access to dental premises, communication issues, dental anxiety and cost.
Article 25: ‘Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care’
Undoubtedly, oral health has an impact on both general health and well-being. Older people report oral health as important to their own quality of life for the purposes of eating, being comfortable, their appearance, ability to smile and laugh and as part of their personality.13 Although people can cope without teeth and/or prostheses, their quality of life is ultimately impaired. It has a negative impact on nutrition resulting from impaired masticatory function and avoidance of foods that are hard to chew, leading to the intake of processed, high cholesterol and lipid-based foodstuffs.14
Article 27: ‘Everyone has the right freely to participate in the cultural life of the community’
Perhaps some of the most treasured moments for those older people resident in care are when they are visited by family members. Time spent interacting with friends at social events and eating together reinforces the importance of a healthy mouth to allow the social interaction enjoyed in life.
‘A culture focused on doing the system's business – not that of the patients’
As politicians attempt to plan for the future and stretch the Treasury's money further, we still have to deliver the frontline care for those in need of our expertise. However, the provision of dental care for the elderly is not, and can never be, business-friendly. The requirements for domiciliary dentistry, transportation to dental clinics, and increased numbers of long and failed appointments all increase costs. Other questions also seek answers. Is our current workforce big enough to meet the need? Are we training our dental students adequately to cope with the demands of providing this type of treatment? Is this a role for generalists or specialists in Special Care Dentistry? Should the importance of oral health be firmly embedded in all healthcare curricula, for example medical and nursing programmes?
What next?
National initiatives such as the Caring for Smiles (http://www.nes.scot.nhs.uk/education-and-training/by-discipline/dentistry/areas-of-education/oral-health-improvement-caring-for-smiles.aspx) Government initiative in Scotland, working closely with the Care Inspectorate, dementia consultants and social services, perhaps point the way towards models of improvement for the future. They need to be supported, however, with research programmes that will help us to understand and overcome the existing psychological barriers to change, if we are to witness significant improvements to oral healthcare of vulnerable older people throughout the United Kingdom. Above all, we need to remember the importance of putting the elderly patient at the very centre of the care we deliver – if we get that right, the rest will follow.