
Article

In simpler times, a dental patient who suffered some kind of harm resulting from clinical negligence would identify the person who provided the treatment in question, and make a claim against that person to seek any appropriate compensation. That makes perfect sense to most people, and apparently to the GDC, which requires individual registrants to hold adequate and appropriate indemnity for their own negligent acts and omissions, designed to make it more likely that patients can receive any financial compensation due to them if they are harmed by negligent dental treatment.
Yet an increasing number of law firms, especially lawyers whose business model is based upon ‘conditional fee agreements’ (CFAs), more commonly referred to as ‘no win-no fee’ arrangements, are disregarding the treating dentist, and instead bringing claims against the owners of the dental practices where these dentists provided the treatment. The purpose of this article is to explain why this is happening, what it means for individual dentists and how practice owners and those trading as or through limited companies can best protect themselves against this growing threat.
Background
The long-established legal principle of vicarious liability means that an employer can be held responsible for the negligent actions and omissions of an employee. Historically based upon a ‘master and servant’ scenario, there is a continuing assumption that there is an element of control, direction, oversight and supervision of an employee that comes with the relative power, seniority and authority of the employer. In essence, the employer makes the rules and the employee is expected to follow them. The employee is an integral part of the employer's business and has very little freedom, autonomy and independence.
From the perspective of a person making a claim, the natural assumption is that the employer, or owner of the business where the injury occurred, will have deeper pockets than any individual member of staff, and the prospect of successfully recovering compensation will be greatly improved if the claim is directed at the employer, either instead of, or in addition to, the individual concerned. Quite apart from anything else, the employer/owner of the business will want to protect its reputation, and will probably have access to insurance anyway.
The situation in general dental practice is unusual in that, whether or not the patients realize the distinction, many dentists are in fact self employed, independent contractors (associates) rather than true employees. Indeed, the proportion of dentists who own or co-own the practice(s) where they work has been steadily reducing. Two other factors have also contributed to changing the landscape in the past 20 years or so: the first of them relates to the legal environment (and in particular, successive reforms of the civil justice system); and the second is the growing number of non-UK-trained dentists joining the UK register, especially from Europe, and who work as associates.
The Wolff reforms to the civil justice system in 19991 paved the way for the ‘no win-no fee’ law firms to enter the personal injury and clinical negligence market in England and Wales. By its very nature, this created a lucrative windfall for the claimant lawyers if they chose their cases carefully and avoided taking on cases, or investing time on investigating cases, that were not likely to deliver a successful outcome, which in turn unlocked the cashpoint. It wasn't long before these law firms were regularly earning fees many times greater than the damages received by their patient clients. But among the frustrations they encountered were dentists who did not have indemnity at all, or whose indemnity at the time of treatment was no longer in force (typically a claims-made insurance policy with no run-off), or who were no longer registered and/or untraceable. Many of the latter were dentists from Europe and elsewhere who had left the UK and returned to their home country. Some of them had discretionary indemnity at the relevant time, but their indemnity provider would not assist them unless and until they requested this in writing. Yet nobody knew their whereabouts, so this hadn't happened. In many instances, they were completely unaware of the claim. The no win-no fee law firms lobbied the government and the GDC to make indemnity compulsory, and ran various campaigns designed to close the other loopholes that were denying them many of the lucrative paydays that they had been set up to achieve.
In 2005,2 the GDC was given additional statutory powers that effectively made it compulsory to hold adequate and appropriate indemnity if a dentist had any direct contact with patients. But across in the civil justice legal system, the gross excesses of the no win-no fee firms were being laid bare, and in response, further and far-reaching legal reforms were foreshadowed from about 2009, fleshed out in 20103 and finally implemented in April 2013.4
Having had their wings clipped, the no win-no fee firms soon turned their attention away from lower value and increasingly unprofitable claims and instead identified certain higher-value types of case to target, often involving multiple dentists. In this altered litigation environment, one newly favoured tactic was to allege that the owner of a dental practice is vicariously liable for the negligent acts and omissions of any member of staff working in or for the practice – even if the person who carried out the treatment was a self-employed associate dentist, contractually responsible for their own actions, even if they are known to hold their own professional indemnity, and even when that dentist's indemnity provider had confirmed their readiness to accept responsibility for the claim. We will explore the reasons for this shortly.
The wider legal context
Over time, and particularly in the past 10–15 years, the courts have come to recognize that modern working relationships are often not a true employer–employee relationship at all. But each court is free to decide whether a particular working relationship, however it is described contractually or intended to operate, is ‘akin to employment’ for the purposes of determining vicarious liability. This assessment is based on criteria developed through a series of precedent cases,13–18 which provided principles that can be applied to a wide variety of business relationships. Practice owners might find it worthwhile to invest a bit of time and effort to read the actual judgements in these cases because there is no better way to understand the key considerations and how different aspects of working arrangements are interpreted, and then to reflect upon how they might apply in their own working situation.
The greater the level of control exerted by the practice owner, and the more unequal the balance of power and freedom to make decisions, the more difficult it becomes to deny that vicarious liability should apply. Put simply, does the associate/contractor appear to be, and act as a genuine free agent making all their own business decisions (effectively, running their own independent business), or are they embedded into the practice and operating as an integral part of it, on terms mostly or wholly set by the practice owner?
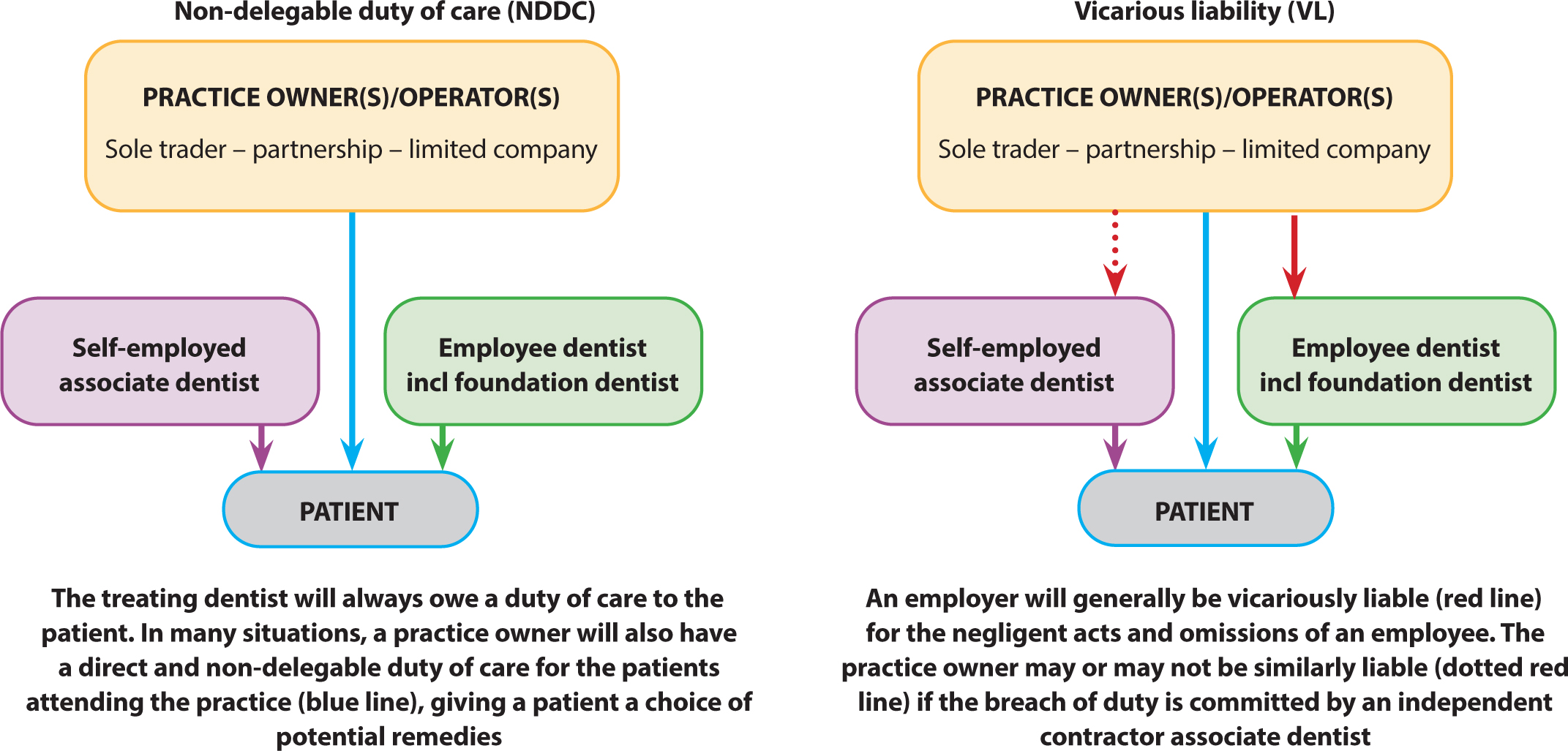
Figure 1 illustrates that alongside the issue of vicarious liability (VL), but different in key respects, sits the separate but equally important question of whether the practice owner has a more direct and non-delegable duty of care (NDDC) to any patient treated within the practice, i.e. an overarching duty of care that still exists, even when the actual treatment is provided by someone for whom the practice owner is not contractually or otherwise responsible, in short, delegating the actual treatment to an apparently competent person does not and cannot remove or absolve the practice owner's own duty of care because ultimately he/she owns and controls (and derives profits and income from) the business. As one Judge pointed out, you can't keep the money and walk away from the responsibility. The key distinction to keep in mind is that the duty of care obligation to exercise reasonable skill and care, and to avoid careless acts that could foreseeably harm others, rests with the treating dentist in the case of VL, but with the practice owner directly in the case of NDDC. But in the case of VL, the practice owner is being held responsible and liable for the treating dentist's breach of duty.
But even where the treating dentist is contactable, there are other reasons why law firms acting for claimants might conduct these claims in what might appear to be illogical ways, looking beyond the treating dentist and targeting the practice owner:
- The situation could arise that a treating dentist's indemnity proves to be lapsed or otherwise non-existent, illusory or non-responsive for the reasons set out above, so the ‘no win-no fee’ law firms have a strong financial interest in giving themselves a second bite of the cherry. Several of the landmark dental cases of recent years (see Table 1) were deliberately chosen to be conducted in this way, partly in order to lay down a base of precedent case decisions that could help to support subsequent litigation in other more problematic cases. Bear in mind that the legal weight of the precedent is lowest at the County Court level, stronger at High Court, stronger still at Court of Appeal, and highest at the level of the Supreme Court of the UK.
- Running these speculative VL and NDDC arguments against practice owners from the very earliest stages in case correspondence, even when the associate who treated the patient is in plain sight, willing to co-operate and known to have their own indemnity, creates an opportunity for the claimant's solicitors to generate significant additional fees from over-working these preliminary arguments, perhaps involving more than one indemnity provider. When they have finished going around the houses, earning fees along the way, they know that they still have the fall-back option of suing the treating associate anyway. Obscenely high legal costs have sometimes been claimed using this ploy, and this compounds the pain for any practice owner who discovers that their personal indemnity does not provide cover for vicarious liability claims and the associated costs.
- One of these no win-no fee law firms has regularly threatened practice owners with statements such as:‘As practice owner, you are directly liable for any negligence of any clinical staff at your practice, regardless of their employment status.’ One of them has even asserted that:‘Practice owners are now responsible, and potentially legally liable, for treatment provided by every associate they employ, and have ever employed, including those who have long since departed from their practice.’ This is actually not true (and was never true), as confirmed by Baroness Hale in the Supreme Court,18 who explained:‘The key (to determining whether or not it is fair, just and reasonable to impose vicarious liability) will usually lie in understanding the details of the relationship’. That assessment is both case- and situation-specific and because each working arrangement is likely to be different, the legal outcome may well be different too. This is well illustrated in Table 1.
Table 1. Recent legal decisions that provide guidance regarding the existence of VL and NDDC in dental practice.
| Year and Court | Case | Nature of business ownership | Vicarious liability? | Non-delegable duty of care ? | Explanatory comments |
|---|---|---|---|---|---|
| 2014HC | Whetstone v Medical Protection Society19 | Dentist sole trader | Yes | Yes | VL and NDDC were dealt with as preliminary issues in a case which related to the refusal of discretionary indemnity to a practice owner for claims based on VL and NDDC for treatment provided by an associate who was known to be unindemnified |
| 2020CC | Ramdhean v Agedo and Forum Dental Practice Ltd20 | Limited company | Yes | Yes | Agedo was an associate who had left UK and could not be traced, so claim proceeded against the practice owners, who traded as a limited company. Although the principal dentist/director had discretionary indemnity, he discovered that the cover did not extend to the limited company |
| 2020SC | Various claimants v Barclays Bank plc18 | Public limited company | No | Not claimed | (Not a dental case, but still very relevant and instructive)Ruled that a doctor providing medical reports was a wholly independent contractor running his own business and providing Barclays with professional services for which he invoiced them |
| 2021CC | Breakingbury v Croad21 | (Retired) dentist sole trader | Yes | Yes | The practice owner had never treated the patient, having already retired, but still owned and operated the practice where the treating associates worked |
| 2021EWCA | Pawley v Whitecross Dental Care Ltd and Petrie Tucker & Partners Ltd22 | Limited companies (large dental corporates) | Yes | Yes | Established that a claimant has no obligation to pursue a treating dentist if they wish to pursue the business owner instead |
| 2022EWCA | Hughes v Rattan23 | Dentist sole trader | No | Yes | High Court had ruled that both VL and NDDC applied. Court of Appeal upheld the NDDC decision but overturned the decision on VL |
SC: Supreme Court of United Kingdom; EWCA: Court of Appeal of England and Wales; HC: High Court; CC: County Court.
In a number of the cases in Table 1, the courts have found it unacceptable that a deserving claimant can be denied access to compensation properly due to them, simply because of the way in which the associate and practice owner have chosen to make their working, contractual and indemnity arrangements. In general, the associate's self-employed status for employment law and HMRC purposes is not hugely material to the determination of VL, and a court will be more persuaded by how the arrangement actually appears to have operated in practice than by how it is viewed by third parties and/or portrayed in any contract between the parties.
In one case, the further question arose of whether, as a principle of social justice and public policy, it was right or fair that the NHS and NHS bodies should have no vicarious liability for independent contractor practice owners who have agreed to provide NHS services that are tightly specified and controlled by the NHS, at a price determined by the NHS and its commissioners, and leaving these NHS bodies able to walk away from any responsibility for dental services that they had elected to commission. It starts to feel like the practice owner(s)/provider(s) have conveniently become the default meat in the legal sandwich, carrying the can on behalf of the NHS on the one hand, and associates on the other.
Managing the risk
Dental claims are often characterized by extended delays between the date of treatment, and the date when a claim is subsequently brought in relation to it. In the meanwhile, a dentist may have left the practice (or the UK), or retired, so the potential risk to a practice owner continues long after the associate dentist has moved on.
It is important to understand that the landscape has fundamentally changed, and while it was understandable in the past that a practice owner might become a litigation target when (for whatever reason) the claimant was unable to obtain compensation by pursuing the treating dentist, today's patients are just as likely to sue the practice owner as any dentist(s) who actually treated them. Until 2021, it was commonplace for a practice owner's indemnity provider to resist the VL/NDDC argument and simply direct the patient's lawyers to the treating dentist's own indemnity provider. But since the Pawley judgement,22 this optimistic deflection strategy, and similarly the option of joining the treating associate into the original proceedings (Part 19 of the Civil Procedure Rules 19989), is unlikely to succeed.
It will be apparent from even a brief perusal of Table 1 that refuting the existence of NDDC may well prove to be an even greater challenge than resisting VL. Although the cluster of legal decisions gathered pace from 2020 onwards, the British Dental Association was ahead of the game, well aware of the pattern of cases coming through and had already identified and flagged up the direction of travel in 2019.5 Indeed, it was with this in mind that it included both VL and NDDC as an automatic feature of policy coverage when launching its ‘BDA Indemnity’ product in 2019. Key points to consider are as follows:
- Have a written agreement Any prudent business owner will want to protect their asset – not least the goodwill - and most contracts between practice owners and either employees or independent contractors, will include clauses designed to achieve this. But ironically, the greater the control and restrictions, the less independent and autonomous the associate will appear and the greater the chance that a court will decide that VL and/or NDDC applies. The standard BDA contract has been designed to strike an appropriate balance, reflecting all of the above legal decisions and other considerations like HMRC's stance on self-employment, but even this is not bombproof because each court will come to its own conclusions based on this and lots of other information from a variety of sources.
- NHS or private? The NHS regulations and NHS contracts and their associated terminology, coupled with the wording of the various documentation relating to NHS treatment itself, paints a picture of whose care the patient is in (or might believe themselves to be in), who they pay NHS dental charges to, the relationships between practice owner/provider, associate/performer and patient, and the respective responsibilities of each party – making it more difficult to demonstrate that VL and/or NDDC should not apply. These additional complications do not arise when treatment has been provided privately.
- Quality control and oversight: On the one hand, it might seem like sound advice to choose your associates carefully, check all available references and to require the associate to participate in regular quality assurance, oversight and internal peer review and clinical audit to flag up potential issues before they arise. Perversely, while laudable for other reasons, this kind of governance risks making the associate seem less independent and much more like an employee subject to the practice owner's supervision and control.
- Indemnity: The associate should be required to supply evidence of their indemnity and annual renewals, and practice owners should not only keep copies of these documents safely, but also establish the nature, scope, conditions and limits of that indemnity (i.e. whether it is discretionary or contractual, occurrence based or claims made. If the latter, what is the position regarding run-off? Is it dependent upon further premiums being paid long into the future? How will the practice owner know if the policy lapses?)
- Right of recovery: For all the reasons explained in this article, it may not be possible to prevent the claim being made against the practice owner. However, employers/business owners do still have a legal right to seek and, hopefully, recover ‘contribution and indemnity’ from employees or contractors whose actions have resulted in a financial loss for the business owner, and it makes sense to confirm this mutual understanding in the contract between the parties. This third party recovery is also permitted by Part 20 of the Civil Procedure Rules,9 which govern proceedings relating to clinical negligence claims, or alternatively it could be made the subject of separate proceedings.
- Contact details: Wherever possible, ensure that you have a dependable way of contacting the dentist after they have left the practice. If a claimant cannot find the treating dentist in order to serve proceedings on them, they will almost certainly turn their attention to the practice owner. Similarly, there is no point having a clause in the contract whereby the associate agrees to indemnify the practice owner, if you have no way of enforcing this. It had been suggested that a departing associate could provide a practice owner with a written authority to act on their behalf after they had left, but some defence organizations have suggested that under their Articles of Association, members must request assistance in person and in writing, and be available to co-operate in the ongoing case management, so a signed and witnessed legal authority presented by the practice owner would still not be sufficient for them to accept and respond to the claim.
- Check your own indemnity: Make sure your indemnity arrangements cover you for claims brought on the basis of your vicarious liability for the negligent actions and omissions of others (many do not, or are subject to tight conditions and exclusions). If you run the practice as a partnership or limited company, check that you are still covered whether the patient chooses to sue you, or the partnership or limited company. If this latter caveat is met, a claim against a practice owner on the basis of NDDC alone is generally less likely to raise doubts regarding scope of cover because it is the practice owner's own duty of care, rather than that of a third party, that is being alleged to have been breached.
Summary
It should be clear from this article that there is no magic formula that allows practice owners to enjoy 100% protection against VL or NDDC claims being brought against them, regarding negligent acts and omissions on the part of their associates. The risk can also present itself in several different ways, so the days of protecting yourself against one such threat and hoping for the best are long gone. Instead one needs to acknowledge that the risk exists, and ensure that you understand it and have taken reasonable steps to protect yourself from the financial, business and other consequences.
Having clear and unambiguous cover for VL claims means that you need not change your chosen working arrangements or weaken or compromise the associateship contract, which is equally important in terms of protecting the practice and its goodwill. Whether or not the time has come to reflect the new reality of VL/NDDC in the financial arrangements between the parties is an individual decision, but as things stand, there is no way of predicting whether claims would be directed against the treating associate, or the practice owner, or both. It is fair to say, however, that the risk of practice owners shouldering this additional burden, solely or jointly, has markedly increased.
Although the GDC has only recently reviewed and updated its guidance on indemnity,6 there is still not a single mention of either vicarious liability or non-delegable duty of care in the new guidance – an omission that is at best curious, and at worst, very unhelpful given all the legal cases and changes in the litigation landscape in recent years. Nor is there any guidance for dentists who trade as, or through, a limited company. A further consideration at the time of writing is the long-overdue decision from the Department of Health and Social Care (DHSC) regarding appropriate indemnity for clinical negligence claims brought against those health professionals (including dentists) who are not covered by NHS indemnity7,8. This was subject to a consultation as long ago as December 2018, since when the Paterson Inquiry and subsequent response (2020/2021) has raised further concerns regarding the status quo and the risk of patients being left uncompensated after receiving negligent care. As an interim measure, DHSC has recently announced that it will allow time for the discretionary defence organizations to jointly agree a new code of practice for how they respond to requests for assistance with clinical negligence claims, including a further review period to assess its effectiveness. The government's final decision on the future of discretionary indemnity still remains one for the future.
Finally, a further imminent legal development may well swing the pendulum yet again and deliver one of the unfulfilled aims of the 2013 (‘LASPO’) reforms,4 which was to achieve greater proportionality of legal costs relative to damages. It is proposed that for lower level clinical negligence claims (up to £25,000, which includes most dental claims), recoverable legal costs for successful claimants will be fixed and capped. The proposals, with a planned introduction date of April 2024, have been vocally opposed by claimant lawyers whose ability to overwork claims and generate disproportionate fees – including from VL and NDDC cases – would be radically curtailed. No doubt the claimant law firms are already hatching new ways to circumvent these changes, but they remain a very encouraging and positive development.
The best advice to practice owners right now is to keep themselves informed, take reasonable steps to protect themselves and ‘watch this space’. Very carefully.