Moraschini V, Fai CK, Alto RM, Dos Santos GO. Amalgam and resin composite longevity of posterior restorations: a systematic review and meta-analysis. J Dent. 2015; 43:1043-1050
Sailer I, Makarov NA, Thoma DS, Zwahlen M, Pjetursson BE. All-ceramic or metal-ceramic tooth-supported fixed dental prostheses (FDPs)? A systematic review of the survival and complication rates. Part I: Single crowns (SCs). Dent Mater. 2015; 31:603-623
Pjetursson BE, Sailer I, Zwahlen M, Hammerle CH. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part I: Single crowns. Clin Oral Implants Res. 2007; 18:73-85
Fleming PS, Koletsi D, O'Brien K, Tsichlaki A, Pandis N. Are dental researchers asking patient-important questions? A scoping review. J Dent. 2016; 49:9-13
Tsichlaki A, O'Brien K. Do orthodontic research outcomes reflect patient values? A systematic review of randomized controlled trials involving children. Am J Orthod Dentofacial Orthop. 2014; 146:279-285
Topcu AO, Yamalik N, Guncu GN Implant-site related and patient-based factors with the potential to impact patients' satisfaction, quality of life measures and perceptions toward dental implant treatment. Implant Dent. 2017; 26:581-591
Baker SK.San Francisco, CA: John Wiley and Sons; 1998
Gassem AB, Foxton R, Bister D, Newton T. Development of a measure of hypodontia patients' expectations of the process and outcome of combined orthodontic and restorative treatment. J Dent. 2016; 55:114-120
Ryan FS, Barnard M, Cunningham SJ. What are orthognathic patients' expectations of treatment outcome – a qualitative study. J Oral Maxillofac Surg. 2012; 70:2648-2655
Newton JT, Cunningham SJ. Great expectations: what do patients expect and how can expectations be managed?. J Orthod. 2013; 40:112-117
Zeithami VA, Berry LL, Parasuraman A. The behavioural consequences of service quality. J Marketing. 1996; 60:31-46
Marachlioglou CR, Dos Santos JF, Cunha VP, Marchini L. Expectations and final evaluation of complete dentures by patients, dentist and dental technician. J Oral Rehabil. 2010; 37:518-524
McCunniff M, Liu W, Dawson D, Marchini L. Patients' esthetic expectations and satisfaction with complete dentures. J Prosthet Dent. 2017; 118:159-165
Riley JL, Gilbert GH, Ford GW Judgment of the quality of restorative care as predictors of restoration retreatment: findings from the National Dental PBRN. JDR Clin Trans Res. 2017; 2:151-157
Yao J, Li DD, Yang YQ, McGrath CP, Mattheos N. What are patients' expectations of orthodontic treatment: a systematic review. BMC Oral Health. 2016; 16
Yao J, Li M, Tang H What do patients expect from treatment with Dental Implants? Perceptions, expectations and misconceptions: a multicenter study. Clin Oral Implants Res. 2017; 28:261-271
Al-Junaid SM, Hodges SJ, Petrie A, Cunningham SJ. Career satisfaction and work-life balance of specialist orthodontists within the UK/ROI. Br Dent J. 2017; 223:53-58
Weldring T, Smith SM. Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health Serv Insights. 2013; 6:61-68
O'Keeffe M, Collins JM, Cunningham SJ. Evaluation of the orthodontic component of the hypodontia care pathway. J Orthod. 2016; 43:268-275
Chapple H, Shah S, Caress AL, Kay EJ. Exploring dental patients' preferred roles in treatment decision-making – a novel approach. Br Dent J. 2003; 194:321-327
Gilmore D, Sturmey P, Newton JT. A comparison of the impact of information from a clinician and research-based information on patient treatment choice in dentistry. J Public Health Dent. 2006; 66:242-247
Oates AJ, Fitzgerald M, Alexander G. Patient decision-making in relation to extensive restorative dental treatment. Part II: Evaluation of a patient decision-making model. Br Dent J. 1995; 179:11-18
Oates AJ, Fitzgerald M, Alexander G. Patient decision-making in relation to extensive restorative dental treatment. Part I: Characteristics of patients. Br Dent J. 1995; 178:449-453
Patel U, Cobourne MT. Orthodontic extractions and the Internet: quality of online information available to the public. Am J Orthod Dentofacial Orthop. 2011; 139:e103-e109
Nason K, Donnelly A, Duncan HF. YouTube as a patient-information source for root canal treatment. Int Endod J. 2016; 49:1194-1200
Ho A, McGrath C, Mattheos N. Social media patient testimonials in implant dentistry: information or misinformation?. Clin Oral Implants Res. 2017; 28:791-800
Ghanem H, Afrashtehfar KI, Abi-Nader S, Tamimi F. Impact of a "TED-Style" presentation on potential patients' willingness to accept dental implant therapy: a one-group, pre-test post-test study. J Adv Prosthodont. 2015; 7:437-445
Stephens R, Ryan FS, Cunningham SJ. Information-seeking behavior of adolescent orthodontic patients. Am J Orthod Dentofacial Orthop. 2013; 143:303-309
Srai JP, Petrie A, Ryan FS, Cunningham SJ. Assessment of the effect of combined multimedia and verbal information vs verbal information alone on anxiety levels before bond-up in adolescent orthodontic patients: a single-center randomized controlled trial. Am J Orthod Dentofacial Orthop. 2013; 144:505-511
Al-Silwadi FM, Gill DS, Petrie A, Cunningham SJ. Effect of social media in improving knowledge among patients having fixed appliance orthodontic treatment: a single-center randomized controlled trial. Am J Orthod Dentofacial Orthop. 2015; 148:231-237
Farmahan S. Hypodontia App: Are patients better informed? A randomised controlled trial.: UCL Eastman Dental Institute; 2016
Edelmayer M, Woletz K, Ulm C, Zechner W, Tepper G. Patient information on treatment alternatives for missing single teeth – systematic review. Eur J Oral Implantol. 2016; 9:S45-57
Kalsi JS, Hemmings K. The influence of patients' decisions on treatment planning in restorative dentistry. Dent Update. 2013; 40:698-710
Measuring shared decision making: a review of research evidence. Shared Decision Making programme. 2012;
Ryan F, Cunningham SJ. Shared decision making in healthcare. Faculty Dent J. 2014; 5:124-127
Wong L, Ryan FS, Christensen LR, Cunningham SJ. Factors influencing satisfaction with the process of orthodontic treatment in adult patients. Am J Orthod Dentofacial Orthop. 2018; 153:362-370
Stacey D, Legare F, Col NF Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2014;
Johnson BR, Schwartz A, Goldberg J, Koerber A. A chairside aid for shared decision making in dentistry: a randomized controlled trial. J Dent Educ. 2006; 70:133-141
Marshman Z, Eddaiki A, Bekker HL, Benson PE. Development and evaluation of a patient decision aid for young people and parents considering fixed orthodontic appliances. J Orthod. 2016; 43:276-287
Parker K, Cunningham SJ, Petrie A, Ryan FS. Randomized controlled trial of a patient decision-making aid for orthodontics. Am J Orthod Dentofacial Orthop. 2017; 152:154-160
Thomason JM, Heydecke G, Feine JS, Ellis JS. How do patients perceive the benefit of reconstructive dentistry with regard to oral health-related quality of life and patient satisfaction? A systematic review. Clin Oral Implants Res. 2007; 18:168-188
Dimberg L, Arnrup K, Bondemark L. The impact of malocclusion on the quality of life among children and adolescents: a systematic review of quantitative studies. Eur J Orthod. 2015; 37:238-247
Javidi H, Vettore M, Benson PE. Does orthodontic treatment before the age of 18 years improve oral health-related quality of life? A systematic review and meta-analysis. Am J Orthod Dentofacial Orthop. 2017; 151:644-655
Baiju RM, Peter E, Varghese NO, Anju P. Patient reported outcome assessment of periodontal therapy: a systematic review. J Clin Diagn Res. 2017; 11:ZC14-ZC9
Thomason JM, Kelly SA, Bendkowski A, Ellis JS. Two implant retained overdentures – a review of the literature supporting the McGill and York consensus statements. J Dent. 2012; 40:22-34
Feine JS, Carlsson GE, Awad MA The McGill Consensus Statement on Overdentures. Montreal, Quebec, Canada. May 24–25, 2002. Int J Prosthodont. 2002; 15:413-414
Thomason JM, Feine J, Exley C Mandibular two implant-supported overdentures as the first choice standard of care for edentulous patients – the York Consensus Statement. Br Dent J. 2009; 207:185-186
Nogueira TE, Dias DR, Leles CR. Mandibular complete denture versus single-implant overdenture: a systematic review of patient-reported outcomes. J Oral Rehabil. 2017; 44:1004-1016
Sivaramakrishnan G, Sridharan K. Comparison of implant supported mandibular overdentures and conventional dentures on quality of life: a systematic review and meta-analysis of randomized controlled studies. Aust Dent J. 2016; 61:482-488
De Bruyn H, Raes S, Matthys C, Cosyn J. The current use of patient-centered/reported outcomes in implant dentistry: a systematic review. Clin Oral Implants Res. 2015; 26:45-56
Sadowsky SJ, Zitzmann NU. Protocols for the maxillary implant overdenture: a systematic review. Int J Oral Maxillofac Implants. 2016; 31:(Suppl)
Thalji G, McGraw K, Cooper LF. Maxillary complete denture outcomes: a systematic review of patient-based outcomes. Int J Oral Maxillofac Implants. 2016; 31:(Suppl)s169-s181
De Kok IJ, Cooper LF, Guckes AD Factors influencing removable partial denture patient-reported outcomes of quality of life and satisfaction: a systematic review. J Prosthodont. 2017; 26:5-18
Reissmann DR, Dard M, Lamprecht R, Struppek J, Heydecke G. Oral health-related quality of life in subjects with implant-supported prostheses: a systematic review. J Dent. 2017; 65:22-40
Naka O, Anastassiadou V, Pissiotis A. Association between functional tooth units and chewing ability in older adults: a systematic review. Gerodontology. 2014; 31:166-177
Tan H, Peres KG, Peres MA. Retention of teeth and oral health-related quality of life. J Dent Res. 2016; 95:1350-1357
Khan SB, Chikte UM, Omar R. An overview of systematic reviews related to aspects of the shortened dental arch and its variants in adults. Int J Prosthodont. 2017; 30:357-366
Fueki K, Baba K. Shortened dental arch and prosthetic effect on oral health-related quality of life: a systematic review and meta-analysis. J Oral Rehabil. 2017; 44:563-572
Hamasha AA, Hatiwsh A. Quality of life and satisfaction of patients after nonsurgical primary root canal treatment provided by undergraduate students, graduate students and endodontic specialists. Int Endod J. 2013; 46:1131-1139
Martensson C, Soderfeldt B, Axtelius B, Andersson P. Expectations and satisfaction with care for periodontal specialist patients. Acta Odontol Scand. 2013; 71:799-806
da Cunha MC, Santos JF, Santos MB, Marchini L. Patients' expectation before and satisfaction after full-arch fixed implant-prosthesis rehabilitation. J Oral Implantol. 2015; 41:235-239
Pacheco-Pereira C, Abreu LG, Dick BD, De Luca Canto G, Paiva SM, Flores-Mir C. Patient satisfaction after orthodontic treatment combined with orthognathic surgery: a systematic review. Angle Orthod. 2016; 86:495-508
Marachini L. Patients' satisfaction with complete dentures: an update. Braz Dent Sci. 2014; 17:5-16
de Souza FI, de Souza Costa A, Dos Santos Pereira R, Dos Santos PH, de Brito RB, Rocha EP. Assessment of satisfaction level of edentulous patients rehabilitated with implant-supported prostheses. Int J Oral Maxillofac Implants. 2016; 31:884-890
Grover M, Vaidyanathan AK, Veeravalli PT. OHRQoL, masticatory performance and crestal bone loss with single-implant, magnet-retained mandibular overdentures with conventional and shortened dental arch. Clin Oral Implants Res. 2014; 25:580-586
Zou Y, Zhan D. Personal factors determining patient satisfaction with all-ceramic crown treatment for single anterior teeth. Int J Prosthodont. 2016; 29:482-483
Adler L, Liedholm E, Silvegren M, Modin C, Buhlin K, Jansson L. Patient satisfaction 8–14 years after dental implant therapy – a questionnaire study. Acta Odontol Scand. 2016; 74:423-429
Takeshita K, Vandeweghe S, Vervack V, Sumi T, De Bruyn H, Jimbo R. Immediate implant placement and loading of single implants in the esthetic zone: clinical outcome and esthetic evaluation in a Japanese population. Int J Periodont Restor Dent. 2015; 35:715-723
, 4th edn.
Veale D, Gledhill LJ, Christodoulou P, Hodsoll J. Body dysmorphic disorder in different settings: a systematic review and estimated weighted prevalence. Body Image. 2016; 18:168-186
Cunningham SJ, Feinmann C. Psychological assessment of patients requesting orthognathic surgery and the relevance of body dysmorphic disorder. Br J Orthod. 1998; 25:293-298
Bain C, Jerome L. Patient communication/restorative dentistry: patient and dentist burnout – a two-way relationship. Dent Update. 2018; 45:22-31
Abstract: This article focuses on those aspects of patient-centred care which are relevant to dentistry. Understanding motivating factors and patient expectations of treatment are fundamental in the provision of high quality care. Ensuring that patients have realistic expectations can be enhanced by providing good information and communicating well at all stages of treatment –factors which also enhance the overall patient experience.
A wide range of factors contribute to patient satisfaction with treatment, alongside meeting expectations and ensuring that the treatment experience is positive, but some of these factors are still not fully understood and more work is required to understand, for example, how patients' psychological traits may influence satisfaction.
It is essential that clinicians consider these factors when providing care for their patients and this paper discusses current evidence relating to patient expectations, patient experience, effectiveness of treatment (primarily quality of life) and also those factors which may impact on patient satisfaction with treatment.
CPD/Clinical Relevance: Patient-centred care involves being proactive about getting patients involved in decision-making and building good professional relationships with which to enhance communication and trust.
Article
Jagdip S Kalsi
Clinicians are required to consider the quality of care provided for patients, both in terms of the process of providing that care and the outcomes of the treatment.
In dentistry, outcomes of treatment have traditionally been assessed in terms of clinician-focused measures; for example, survival rates of restorations.1, 2, 3 However, recent years have seen a move to incorporate patient-centred measures alongside these clinician-derived measures. The Darzi report in 2008, High Quality Care for All,4 played a major part in implementing plans for an NHS which works in partnership with patients to deliver the best quality care possible and this report emphasized that most people want a greater degree of control and influence over their own health and healthcare.
Lord Darzi's summary letter stated that ‘High quality care should be as safe and effective as possible, with patients treated with compassion, dignity and respect. As well as clinical quality and safety, quality means care that is personal to each individual’. The document Liberating the NHS: No decision about me without me5 further reinforced the need to increase opportunities for patients, and their representatives, to have more involvement in decisions about their care all along the patient pathway. It is on this basis that modern healthcare is delivered.
It is therefore important that research in dentistry considers both patient and clinician perspectives and this remains a challenge. Fleming et al6 performed a systematic review of the types of outcomes reported over a three-year period in eight prominent dental journals. They found that 44% of publications were primarily clinician focused, 34% were patient-centred and 22% had elements of both patient and clinician focus. The researchers concluded that there was undue emphasis on technical, clinician-centred outcomes in all dental specialties and highlighted the importance of developing and adopting core outcome sets for use in dental research.
A systematic review by Tsichlaki and O'Brien7 identified the types of outcomes in recent orthodontic trials; their findings showed that morphologic features of malocclusion were measured in 63% of the studies included in the review, but patient-centred outcomes, such as adverse effects of orthodontic treatment and quality of life effects, were measured in only 32% and 9% of studies, respectively. The lack of patient-centred measures is also evident in the implant literature, with Topcu et al stating that, in the region of only 2% of implant outcome studies focus on patient-based outcomes.8Whilst dentistry has made major efforts in incorporating patient-centred measures, there is clearly still further work to do.
Quality of care from a patient-centred perspective may be defined in many ways but three criteria have frequently been cited:
Patient safety;
Patient experience; and
Effectiveness of care.
This paper will focus predominantly on the patient experience and effectiveness of care under the following subheadings:
Understanding motivations and meeting patient expectations;
The patient experience;
Effectiveness of treatment from the patient perspective, with an emphasis on quality of life (QoL);
Patient satisfaction.
1. Understanding motivations and meeting patient expectations
Understanding motivating factors and expectations is fundamental to providing high quality care. Ensuring that patients' expectations are met is a key determinant of satisfaction with the outcomes,9 and also enhances a patient's engagement with the clinical process.10 However, motivation and expectations are complex and developed in a number of different ways.
When starting treatment for any patient, it is useful to think in terms of the problem (or the impact), the motivation and the expectations and these may be, for example:
The problem/impact: ‘I don't like the appearance of my missing front tooth’;
The motivation: ‘I would like a bridge or implant to make it look better’;
The expectations: ‘If I get the improved appearance I want, I will feel more confident when meeting people and I will smile more in photographs’. A useful question to ask patients in order to understand their expectations is how they think their life will be affected by the treatment that they are hoping to embark on and what they think will be different afterwards.
It is important to stress that the relationship between these three elements is not a straightforward linear relationship and many other factors play a part and mediate the motivation and expectations, for example the type of healthcare system, the influence of family and friends, cultural aspects, etc.11, 12 However, all three aspects need to be fully explored to ensure that a treatment plan is likely to meet the individual's expectations and, if there is any doubt as to whether the expectations will be met, these must be fully explored with the patient before commencing treatment. If expectations are not met, this may result in the patient being dissatisfied.
However Zeithami et al13 discussed the concept of the ‘zone of tolerance’, where small failures of expectation may be acceptable, depending on the importance of that particular aspect of a service. If the expectations relate to something which the patient perceives as being particularly important, then the zone of tolerance is likely to be smaller than an aspect of care which is not seen as having such great importance. It is therefore crucial that clinicians understand which are the key areas of importance for an individual patient.
A 2012 publication in the orthognathic literature explored patients' expectations and developed a typology classification which allowed a clearer view of some of the complex social phenomena which arose in the qualitative interviews undertaken.11 The authors highlighted that, by being able to classify expectations in this way, it allows a clearer understanding of the patient and his/her expectations and, in doing so, will hopefully enhance patient satisfaction.
Motivations and expectations have also been explored in various areas of the prosthodontic literature.14, 15, 16 Marachlioglou et al14 explored patients' expectations of the aesthetics and function of complete dentures and compared them with those of the dentist and the technician. The patients had significantly higher expectations of their dentures than the dental professionals, although interestingly also provided higher post-treatment scores. The important aspect of this study though was the difference in the initial expectations between the patients and the dental professionals and this is an important factor in clinical practice which must be resolved by ensuring good communication prior to undertaking any treatment and by providing patients with detailed explanations about the potential benefits and limitations of treatment.
McCunniff and colleagues15 undertook secondary data analysis of four studies which had looked at patients' expectations and post-treatment satisfaction in complete denture construction. Their findings suggested that, although patients' expectations of denture aesthetics were high, their satisfaction usually exceeded their expectations. Men showed higher expectations than women, but there were no other gender or age specific effects. Whilst such findings are reassuring, the paper highlighted the importance of further research to provide a greater understanding of those factors which affect expectations and satisfaction.
Whilst clinicians have some understanding of expectations and their importance in dentistry, there is still work to be done in this area. A better understanding is needed of how patients develop their initial expectations and how expectations change during a course of treatment; a better awareness of how expectations may influence treatment outcomes is also required.17, 18 The provision of good information is fundamental in ensuring that patients have realistic expectations and this will be discussed in further detail in the next section of this paper. The ever-important issue of good patient-clinician communication is also key to this aspect of care.
There is little doubt that patients in all areas of medicine and dentistry have increasing expectations of the services and outcomes which can be delivered and managing patient expectations is an important issue for both patients and clinicians. A recent study looking at career satisfaction and work life balance in orthodontists found that those clinicians who said that they found it increasingly difficult to manage patient expectations, had significantly poorer career satisfaction and significantly poorer work-life balance than those who felt that they managed expectations well.19 It is therefore critical that we continue to educate undergraduates, postgraduates and all members of clinical teams in the optimal management of patient expectations; ensuring this will hopefully have a positive impact for both patients and dental professionals.
2. The patient experience
There has been an increased understanding of the importance of the patient experience in recent years and the NHS has acknowledged this by embedding patient experience indicators into NHS frameworks.20 The patient experience covers a diverse range of aspects of care, including the staff and the environment, information provision and involving patients in shared decision-making about their care.
Elements of the patient experience which have frequently been found to be important include being treated with respect, being included in discussions about their own care and having kind, supportive clinicians and nurses. Recent research has confirmed that patient satisfaction is enhanced when such elements existed in their care.21, 22, 23, 24, 25
The provision of high quality information also plays an important part in the patient experience and links to the previous section of this paper. Ensuring that accurate information is provided goes some way to ensuring realistic expectations and this, in turn, may enhance satisfaction. There is much information available on the internet regarding dental treatment but patients often struggle to know which information is accurate and which is not. A 2011 study by Patel and Cobourne26 looking at internet-based information about orthodontic extractions found that this information had generally poor reliability (41%). It is therefore perhaps not surprising that patients attend for consultations with inaccurate information and potentially unrealistic expectations.
Nason et al27 highlighted concerns about the lack of evidence base and quality control in their study investigating YouTube™ videos about endodontic treatment. A search was undertaken based on three key words: endodontics, root canal and root canal treatment and 20 videos were assessed for quality for each search term. Videos posted by dental professionals and commercial sources were found to be significantly more complete than those posted by laypeople, but only 46% of the videos were actually posted by a dentist/specialist source. The study concluded that the completeness of the videos varied significantly and encouraged professionals to be aware of the information available on the internet and to direct their patients to the higher quality information, thus reducing the amount of inaccurate information they obtain.27
A similar study in the implant literature assessed the content of YouTube™ patient testimonials for dental implants.28 Encouragingly, informative points were included more frequently than misleading information, but the information provided was judged to be limited, with fewer than two points of information per video. Patients were often informed that implants could improve aesthetics and function, but information regarding pain and pain control was potentially misleading. Many of the videos were uploaded by clinicians, although they were patient opinions, and the paper highlighted the importance of clinicians being responsible for the content uploaded under their name/practice name. The paper also noted the importance of clinicians being aware of the limitations in the information present when patients search online and this is an important aspect of future work.28
However, there is evidence to show that, when accurate information is presented appropriately, it can be helpful to patients. Ghanem and colleagues29 undertook a study to investigate the effect of a TED-like presentation (Technology, Entertainment and Design website that provides short online talks by expert speakers) on patients' willingness to accept implant treatment. Patients who were interested in potentially undergoing implant treatment completed a questionnaire before and after the short presentation and the researchers found that respondents were significantly more likely to accept implant treatment after the information had been provided.29
These findings highlight the importance of the profession providing and collating high quality information in different formats and ensuring that it is readily accessible. It is also important that patients are asked how they would like information to be provided30 and the advent of individualized provision of care means that patients' views should be considered when providing this information. Recent years have seen dental research into the provision of high quality information in different formats, including audio-visual,31 social media,32 and Apps.33 Providing information in these ways has been found to enhance knowledge about a condition or treatment31, 32, 33 and has also been shown to enhance satisfaction with the treatment process.33
However, none of these adjunctive methods replaces good quality information from dentists; instead they should supplement the information provided by the clinician. A recent systematic review investigating patient information about replacement of missing teeth showed that clinicians were the most important source of information, followed by the media, family and friends. Therefore, clinicians play a key vital role in improving awareness and knowledge about treatment alternatives.34
National and international societies can also take a lead in producing high quality evidence-based patient information products; for example, the patient information provided by the American Academy of Periodontology (https://www.perio.org/consumer/patient-resources) and the information provided by the British Orthodontic Society about orthognathic treatment (https://www.bos.org.uk/Public-Patients/Your-Jaw-Surgery1). Such organizations should also consider ensuring that their sites appear on the first results page when patients undertake internet searches and this requires a knowledge of the terms which patients/members of the general public use.30 This increases the likelihood that patients will access high quality, evidence-based information regarding their treatment.
A further key aspect of the patient experience is shared decision-making.35 Shared decision-making is essentially a two-way process where the patient and clinician share the responsibility for decision-making and may be defined as when ‘….clinicians and patients work together to select treatment, based on clinical evidence and the patient's own preferences…….. involves the provision of evidence-based information about options, outcomes and uncertainties….’.36, 37 Shared decision-making has replaced the traditional paternalistic way of providing treatment and is an area which is a major focus in the NHS. The importance of shared decision-making in dentistry is highlighted in recent research in looking at satisfaction with adult orthodontics, where patients discussed that shared care had enhanced their satisfaction with treatment: ‘They involved me in making decisions… they asked for my opinion, and I felt that I'd come to the right place’.38
A study conducted in both a hospital and general dental practice setting found that patients wished to have a shared decision-making role in their own care but the same patients felt that their current role was passive and they were not actually involved in shared decision-making.22 It is important to acknowledge that this research was undertaken some time ago, but nevertheless it is important that clinicians question how much they involve patients in decision-making about their own clinical care.
Shared decision-making can be enhanced by decision-making aids, which have been utilized in medicine for some time now. These aids can take a number of different formats (leaflets, decision boards, etc) and a recent Cochrane review highlighted the benefits of using decision aids; including, improved patient knowledge, better informed patients, more accurate expectations and allowing patients to be more effectively involved in decision-making.19, 39 Interest in decision-making aids has increased in dentistry in recent years and decision aids have now been tested in endodontics40 and orthodontics.41, 42 An example of shared decision-making is given in Case 1.
3. Effectiveness of treatment from the patient perspective, with an emphasis on quality of life (QoL)
Effectiveness of treatment covers numerous aspects but one which has received much interest in recent years is quality of life. There are many definitions which have been used, including that by the World Health Organization43 which states that Quality of Life is ‘A state of complete physical, mental, and social well-being not merely the absence of disease’. Dental treatment has a number of aims from the patient perspective, including pain relief, enhanced function, improved aesthetics and enhanced psychosocial aspects of life. All of these come under the term ‘quality of life’ and effectiveness of dental treatment therefore often focuses on one or more elements of quality of life. Clinicians see individual patients on a daily basis who report enhanced quality of life as a result of dental interventions and the literature publishes a wide range of dental studies looking at this area of research and showing quality of life benefits. However, the challenge to the profession is in providing high quality evidence of QoL benefits through studies undertaken using optimum quality methodology, systematic reviews and meta-analyses.
In one of the early systematic reviews investigating QoL effects in dentistry, Thomason et al concluded that there were insufficient studies in reconstructive dentistry to reach any robust conclusions regarding QoL effects and called for more studies in this area.44 Only a decade later progress has definitely been made and this increasing evidence base is reassuring, but there are still limitations in terms of heterogeneity related to study design, inclusion and exclusion criteria, questionnaires/instruments utilized to measure QoL, duration of follow-up, etc. Overcoming some of these issues is the challenge for future quality of life research in dentistry.
It is important to acknowledge that there are now systematic reviews which have allowed more definite conclusions to be reached and these findings are encouraging. A number of these reviews and their findings are discussed below:
Orthodontics: Dimberg et al45 highlighted the negative effects on quality of life in children/adolescents with malocclusion in their systematic review and, more recently, Javidi et al46 concluded that there is evidence that correction of such malocclusions by orthodontic treatment is associated with improved quality of life after treatment, especially in the emotional and social well-being domains. They did, however, highlight the limited quality of the evidence.
Periodontology: Baiju and colleagues47 concluded that both surgical and non-surgical periodontal treatment significantly influenced QoL, although there was no significant difference between the two treatment modalities. They also highlighted the need to develop appropriate condition specific measures to assess changes in QoL and the need to undertake more high quality longitudinal studies.
Complete dentures: Thomason et al48 found substantial evidence that QoL improvements with implant-retained overdentures (IODs) were significantly greater than for conventional dentures, which is reflected in both the McGill and York Consensus Statements.49, 50 In contrast, Nogueira et al51 undertook a systematic review to investigate whether single-implant mandibular overdentures (SIMO) improved patient-reported outcomes more than conventional dentures in edentulous patients. Of the eleven studies included, all studies reported that SIMO resulted in marked improvements in quality of life, but unfortunately there was insufficient evidence to compare the two treatment modalities. The authors called for better reporting and more standardization of instruments to allow data to be compared more readily. Similar positive findings associated with implant-supported mandibular overdentures compared with conventional dentures were noted in the systematic reviews by Sivaramakrishnan and Sridharan52 and De Bruyn et al.53 Sadowsky and Zitzmann,54 in their review of maxillary implant-retained overdentures, also found that provision of implant-supported dentures provided enhanced satisfaction and quality of life. However, it must be noted that the picture is not quite as clear for maxillary dentures as it is for the mandible and studies, including Thalji et al55 who also found improved QoL with conventional mucosal borne complete dentures.
Removable partial dentures (RPDs): De Kok et al56 found modest increases in QoL in RPD wearers but their systematic review failed to find any evidence of better quality of life than in untreated partially dentate patients or where restoration using fixed prostheses or implants was undertaken. Satisfaction appeared to relate to the replacement of anterior teeth or numerous posterior units on RPDs.
Dental implants: Reissmann et al57 investigated the outcomes of QoL in partially dentate and edentulous patients. They found that lower QoL scores prior to treatment were strongly associated with greater improvements in post-treatment QoL. There was insufficient evidence that fixed implant prostheses improved QoL more than tooth-borne fixed prostheses. Moderate quality evidence suggested that fixed implant prostheses perform better than conventional RPDs. As noted above, evidence from some of the included studies for partially dentate subjects suggested that the magnitude of QoL improvement after treatment was linked to the number and location of implants to replace missing teeth. Greater improvements were expected for anterior than posterior tooth loss and when more teeth were replaced.
Maintaining a functional natural dentition: Naka et al58 investigated subjective chewing ability relative to functional tooth units and found that patients reported a satisfactory chewing ability with a shortened dental arch (SDA), and stressed the importance of dentists focusing on preventive and restorative regime to maintain functional dentitions for a patient's lifetime. Similar findings were noted by Tan et al. 59 in their systematic review which showed that higher numbers of retained natural teeth were associated with better oral health-related quality of life, (OHR)QoL, and that anterior tooth loss and absence of posterior occlusion were associated with impaired QoL. Khan et al.60 also reported positive findings associated with the SDA concept in their review. Fueki and Baba's systematic review61 investigated prosthodontic and SDA approaches for the free-end saddle but showed no significant difference in QoL outcomes between the SDA and removable denture groups; however, they did highlight the small number of papers/patients included in the review.
Whilst there are an increasing number of systematic reviews focusing on QoL in dentistry, evidence is still lacking in some areas. However, it must be stressed that lack of evidence does not mean there is no effect, rather that the evidence currently available does not allow definite conclusions to be drawn. This is one of the aspects of research in dentistry which must be a focus for the future.
Case 1
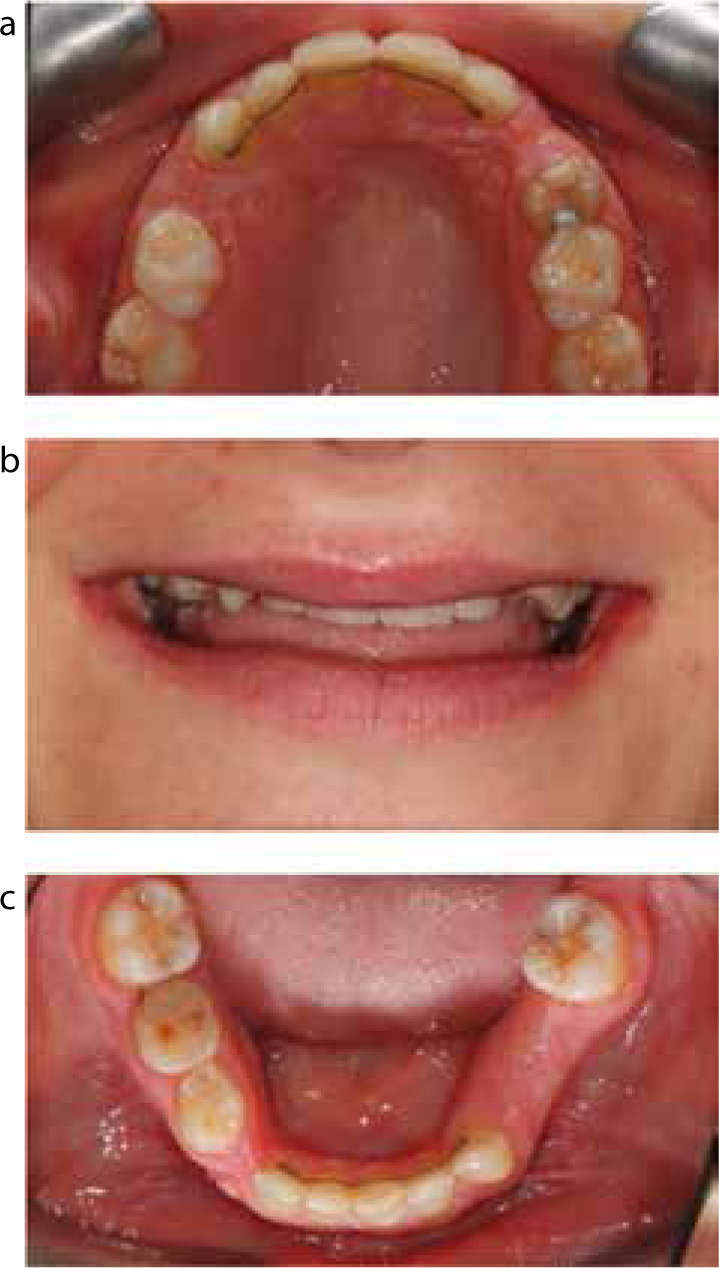
A 21-year-old patient (Figure 1) attended a prosthodontic clinic for advice regarding her severe hypodontia. The patient was given several options regarding treatment but was extremely anxious about the treatment process itself and also about the potential aesthetic and functional outcomes associated with the various options available. The potential treatment options were discussed in general terms initially and then in more detail over a number of visits. The patient was also directed to online resources where she could find out further evidence-based information. The patient's anxiety levels reduced but she still felt unable to make a treatment decision. Encouragement was given that this was not an urgent decision to make and as much time as was needed should be taken to make the right decision. At that stage the clinician also offered the chance to speak to another patient who had faced similar treatment decisions but who had now completed treatment. The clinician was comfortable that the previous patient would give a balanced, informed view and had already offered to speak to prospective patients if this was ever helpful. The two patients spoke by telephone and the potential patient asked a number of questions which she felt that the clinicians would not have been able to answer. After some further time considering the options, the patient felt comfortable making a decision on how to proceed and was ultimately very happy with the outcome (Figure 2).
Figure 1.
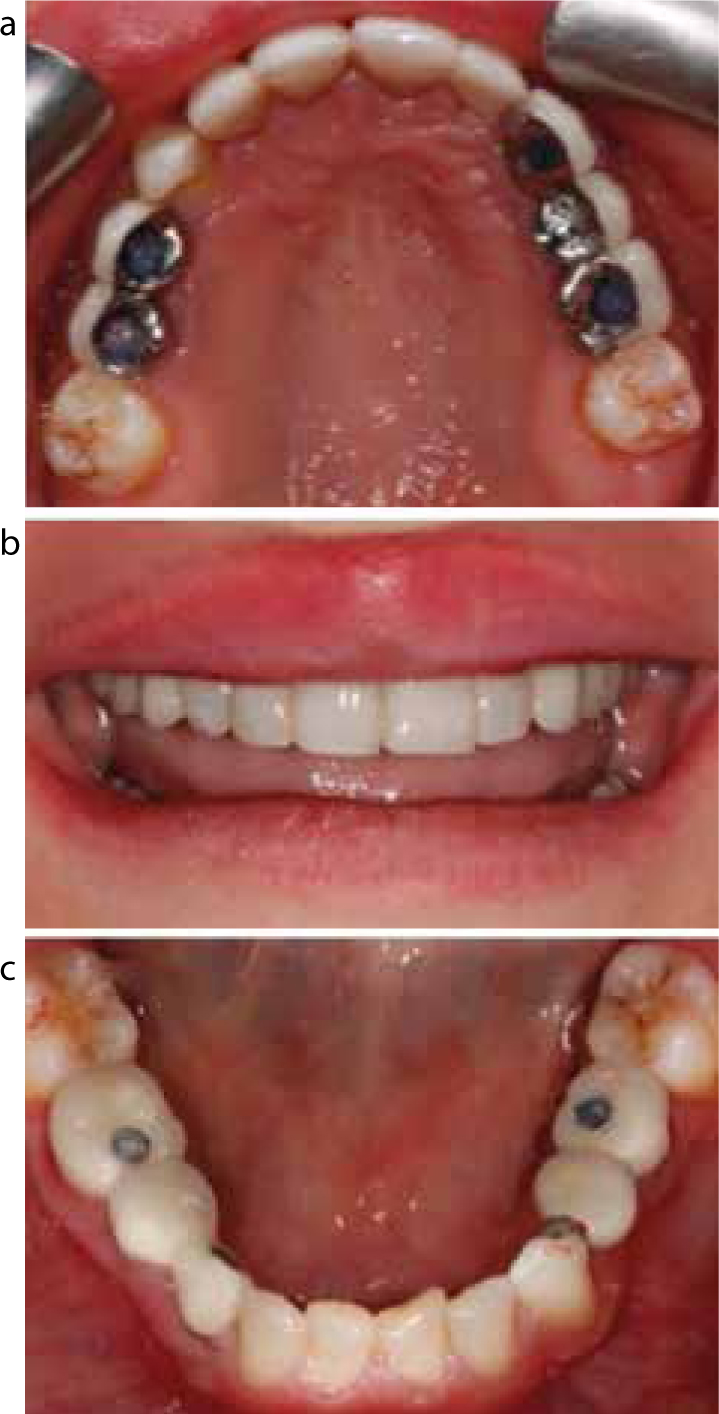
(a–c) Case 1: pre-operative views.Figure 2.
(a–c) Case 1: Views after maxillary anterior composite build-ups, and fit of dental implant-retained crown and bridgework with alveolar bone augmentation and sinus lifts, and a resin-retained bridge, posteriorly. The implant screw access chambers were due to be restored definitively with composite resin
This scenario highlights the importance of ensuring patients have all of the information they need to make treatment decisions and that they are not rushed into making decisions. It also illustrates how previous patients can be helpful in aiding that process.
Case 2
A 22-year-old patient attended for treatment to enhance the appearance of the maxillary incisors which were affected by hypoplasia (Figure 3) and had previously been restored with composite veneers that had stained. The patient was under the impression that she would have porcelain veneers but a decision was made that it would be more appropriate to replace the composite veneers as this would be less destructive. The patient was upset that she would not be able to have porcelain veneers as that was what she was expecting. The clinician spent some time explaining why this decision had been made and the patient appeared satisfied to proceed with treatment. When the composites were replaced, the patient was upset and clearly not satisfied with the result (Figure 4). It transpired that the patient wanted a ‘glossy finish’ and was not aware that the composite veneers would not result in the same level of gloss as porcelain veneers and she had spent a lot of time on the internet looking at images of the expected outcome.
Figure 3. Case 2: pre-operative view of hypolastic maxillary incisors.Figure 4. Case 2: replacement composite veneers.
Although a considerable period of time was spent explaining why composite veneers were planned rather than porcelain veneers, the patient was expecting porcelain aesthetics and the clinician had not been aware of this. The patient was willing to consent for porcelain veneers, accepting the risks of biological damage, and the composite veneers were replaced with porcelain, with which that patient was happy (Figure 5).
Figure 5. Case 2: definitive porcelain veneers.
In hindsight it would have been sensible to show images of both types of veneers to illustrate the different aesthetics and also to show the extent of the preparation which would be required if porcelain veneers were undertaken. The importance of ensuring that the patient's expectations are fully understood cannot be over emphasized and all appropriate resources should be utilized in an attempt to show patients what the likely outcomes of a course of treatment may be.
4. Patient satisfaction
It is sometimes easy to assume that, if good quality of care is delivered and a good outcome is achieved, then the patient will be satisfied, but as clinicians we all know this is not necessarily the case and other factors contribute to satisfaction with treatment. The factors associated with patient satisfaction are complex and still not fully understood. This is, however, an area of research which is showing increased interest in the medical and dental literature.
There is now good evidence that the relationship between the dentist and the patient is an important factor in achieving satisfactory patient outcomes in a number of areas of dentistry, including prosthodontics,24, 25 endodontics,62 periodontics,63 implant dentistry64 and orthodontics.65 This is an important area for all clinicians, especially when considering areas such as staff development and training. It is essential that all members of the team are aware of the importance of good communication skills, effective patient management and providing treatment in a holistic way.
Patient satisfaction is associated with a number of different factors, as illustrated in a recent systematic review of patient satisfaction in orthodontics.65 This review separated those factors which were associated with satisfaction and those which appeared to be associated with dissatisfaction. The authors found that satisfaction was associated with the quality of the aesthetic outcome, the quality of care delivered, the patient-clinician relationship and certain personality traits. In contrast, dissatisfaction was associated with treatment duration, pain, retainers and other specific personality traits (eg neuroticism). This review highlighted the importance of ‘internal’ patient factors, including personality traits, when considering the factors which may influence outcomes of treatment.
A publication looking at satisfaction with complete dentures highlighted similar factors. A study of the literature since 2001 showed that factors affecting satisfaction included personality and psychological factors, the patient's perception of the dentist and the care provided, the patient-dentist communication and the actual treatment undertaken (implant-retained prostheses were associated with higher levels of satisfaction than conventional dentures).66 The authors highlighted the importance of more research in this area in order to enhance understanding of how to provide the very highest quality care.
Although clinical factors, such as age, bone quality, speech and mastication, have been shown to affect satisfaction with prosthodontic and implant outcomes,67, 68, 69 overall the evidence suggests that patients are satisfied with fixed and removable prostheses. However, the effect of neurotic personality traits may reduce those levels of satisfaction64, 67, 68, 69, 70 and further research is required to investigate how best to manage such patients effectively.
Interestingly, dentists' satisfaction with the technical quality of their implant and denture work does not necessarily correlate well with the patients' satisfaction. Takeshita et al71 showed that only half of the implant cases assessed were rated as satisfactory by the dentist, but 96% of patients were satisfied. Additionally, Marachliglou et al14 found that patients reported significantly more benefits related to their denture treatment than dentists. This shows that patients may well be satisfied with treatment, despite dentists' perceptions of the outcome. This is important to consider when treatment planning, as further intervention may sometimes not be in a patient's best interest if there is unlikely to be a significant improvement for him/her.
The importance of considering personality traits and psychological factors is highlighted in this area of research and it is also important to consider the condition body dysmorphic disorder (BDD) in this section. BDD is a psychiatric condition in which there is a preoccupation with an imagined or minor defect in appearance, which causes significant distress in social, occupational and other important areas of functioning and is not better accounted for by another mental disorder (eg anorexia nervosa).72 In the dental context, this is typically patients who attend with excessive concern about a dental problem which is having a much greater impact on their life than would be anticipated considering the relative severity of the problem. A recent systematic review of the dental literature showed that the prevalence of BDD is 5% in orthodontics and the cosmetic dentistry population and 11% in the orthognathic population, compared with around 2% in the general population.73 It is therefore possible that we all see patients with BDD in our clinical practice and should be vigilant to this possibility. BDD is of particular importance in this context for two reasons: first, and most importantly, from a patient safety perspective as patients with BDD are at risk of suicidal thoughts and suicide attempts, so any patient who is thought to be potentially suffering from BDD must be sent for appropriate assessment and care. Secondly, patients with BDD show an increased chance of being dissatisfied with the outcome of care, even if the outcome is good from the clinician's perspective. Physical treatment is rarely the best treatment option in this group of patients and, unless supported by an appropriate mental health professional, will often be associated with dissatisfaction if undertaken.74
Recently, Bain and Jerome75 identified the concept of patient burnout in dentistry, defined as an emotionally exhausted dental patient. Patient burnout is associated with complex treatment, high and unrealistic expectations, and a focus on treatment rather than care, with less emphasis on diagnosis and treatment planning than on performing procedures. The authors also proposed a two-way relationship between patient and dentist burnout whereby dentists exposed to a number of burnout patients may cumulate in burnout for the dentist. Patient burnout can be minimized by good non-verbal, verbal and written communication, not progressing with complex treatment too fast, under promising and over delivering and keeping treatments simple.75
Although patients seek dental treatment in an attempt to achieve enhanced aesthetics, function, and psychosocial outcomes, the factors affecting ultimate satisfaction with the outcomes of treatment are complex and not yet completely understood. An example of patient satisfaction is given in Case 2.
Conclusions
There have been significant efforts in recent years to ensure that patient-centred care in dentistry is provided and the evidence base in this area continues to increase. There is undoubtedely work still to do though and the key areas are highlighted in this paper.
Clinicans want to provide high quality care for all patients and the vast majority of patients appear to be satisfied with the work provided for them. Based on the current evidence, patient complaints and disappointment may be reduced with the practical tips included in Table 1.
Motivation and expectations:Take a detailed history and always ask patients what they expect from treatment: explore the expectations as well as the problem and the motivation. If a clinician has concerns, ask for a specialist opinion.
The patient experience:Discuss this with the whole team in the practice.Ring the practice and see if any changes need to be made, visit another practice and see if there are areas of good practice that could also be used, etc.Is there the right balance of risks and benefits for different treatments in the practice information leaflets and on the website.What other websites might be useful to recommend to patients?
Effectiveness of treatment and quality of life surveys:Could any outcome surveys be usefully be introduced in the practice? More information from studies carried out in both practice and hospital settings will be invaluable.
Patient satisfaction:Good communication is important at all stages of patient care. Check satisfaction with communication on a personal level. Is the practice's communication training updated regularly? Could any changes be made? Would treated patients be happy to discuss their treatment with those who may undertake similar treatment?