
Article


Oral cancer in the initial clinically detectable stage is usually a red or red and white (erytholeukoplastic) area without symptoms. In more advanced stages, there is a single ulcer or lump with irregular margins, which are rigid to touch (indurated), and pain is the most frequent symptom – especially in tongue and floor of mouth cancers.
The most important task is to establish an early diagnosis in the first stages of the disease, when treatment needed is less severe and the prognosis is best. The different diagnosis for oral cancer includes other malignant diseases (eg lymphomas, sarcomas and metastases), which usually grow more rapidly than a typical oral cancer; and chronic infections (eg syphilis, tuberculosis, or a fungal condition such as histoplasmosis).
Location
The most common locations for mouth cancer are the lower lip (40%), and the tongueand the floor of the mouth (50%). The lip is involved more frequently in some geographic areas with sunny climes. Other oral areas involved include the buccal mucosa, retromolar area, gingiva, soft palate and, less frequently, the posterior tongue and hard palate.
Symptoms
Early carcinomas often go unnoticed because they are asymptomatic. Pain often appears only when lesions have reached some size, and it may vary from mild discomfort to severe pain. In cancer of the tongue, the movement of the tongue against the teeth can increase the discomfort. In contrast, carcinomas of the lip or buccal mucosa only produce pain at advanced stages.
Other cancer symptoms may include:
Symptoms such as ear pain, voice changes, and dysphagia are more common in tumours at the tongue base. Occasionally, patients present with cervical lymphadenopathy. In terminal stages, skin fistulas, bleeding, severe anaemia and cachexia may develop.
Clinical presentation
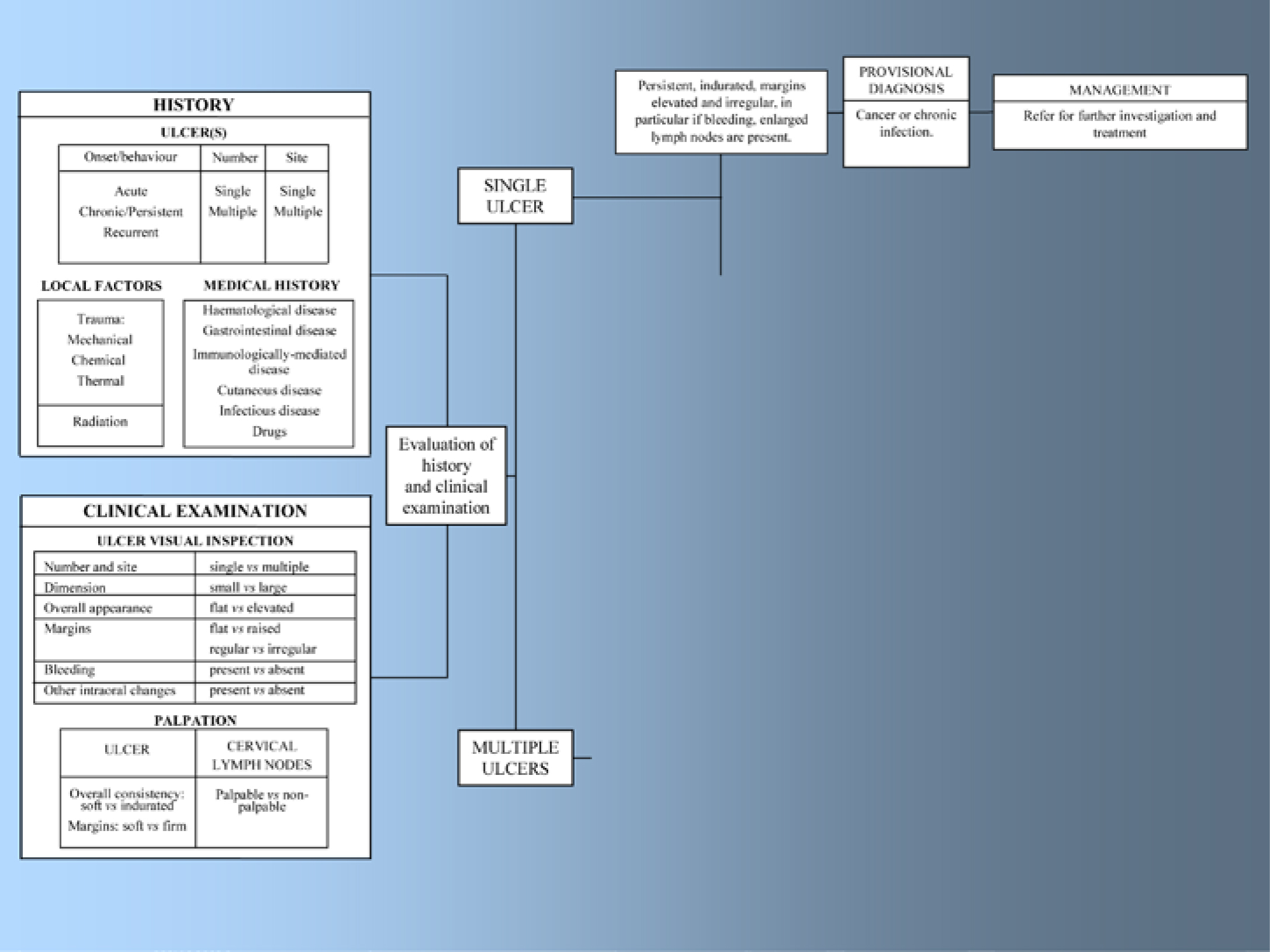
A full history and thorough and systematic clinical examination of the oral mucosa is mandatory, particularly of those sites that are especially predisposed to cancer, such as the sides of the tongue and the floor of mouth. It is crucial also to palpate the neck lymphoid tissue (cervical lymph nodes) to detect masses which might represent metastases.
Lesions of oral cancer can range from a few millimetres, to several centimetres in diameter. The initial lesions are usually solitary and asymptomatic when they are small and thus, in the early stages, misdiagnosis is possible. The clinical presentation in advanced stages, however, is so characteristic that there is usually a firm suspicion of malignancy. Cancer must be suspected in patients with any single oral lesion persisting for more than 3 weeks (Figure 1).
It is always necessary to establish the diagnosis by a biopsy and histopathological examination, because the clinical characteristics alone are insufficient to be absolutely certain.
The clinical presentation of early cancer is usually as an erytholeukoplastic lesion – a well-demarcated red or red and white area with a slight roughness. The elasticity of the soft tissue changes to a harder sensation on palpation (‘induration’) as the lesion progresses.
The classic features at a later stage include ulceration, nodularity and fixation to underlying tissues. Ulceration usually has an irregular floor and margins, and is raised and hard on palpation (indurated). The patient often then has severe pain, radiating from the lesion to the ipsilateral ear (Figure 2).

In advanced stages, exophytic tumours may be seen with warty surfaces, and poorly defined boundaries which are difficult to palpate (Figure 3).

Less common manifestations include:
| Red lesion (erythroplasia or erythroplakia) |
| Mixed red/white lesion (erythroleukoplakia); irregular white lesion (verrucous leukoplakia) |
| Lump |
| Ulcer with fissuring or raised exophytic margins |
| Pain or numbness |
| Abnormal blood vessels supplying a lump |
| Loose tooth |
| Extraction socket not healing |
| Induration beneath a lesion, ie a firm infiltration beneath the mucosa |
| Fixation of lesion to deeper tissues or to overlying skin or mucosa |
| Lymph node enlargement |
| Dysphagia |
| Weight loss |
Occasionally, cervical lymph node enlargement is found in the absence of any obvious primary oral tumour – when the likely site for the primary (in order of predilection) is the tongue base, tonsil or nasopharynx.
The factors most associated with mortality are: location on the gingival or in the retromolar trigone, large tumour size, and lymph node involvement.
Diagnosis
In 1998, the UK White Paper – ‘The New NHS’ – set a target for all patients with suspected cancer to be seen by a specialist within 2 weeks of their GP deciding that they need to be seen urgently and requesting an appointment. QED – Quick, Early Diagnosis – was the aim. The report of the Head and Neck Cancer Working Party to the Department of Health Steering Group on The Development of National Guidance Relating to Urgent Referral of Patients with Suspected Cancer recognized the importance of multiple factors of varying significance.
Factors which should give rise to a high index of suspicion by the GP/GDP included:
Early diagnosis is the most important factor for improving patient survival (rates as high as 80–90% may be achievable) and also minimizes the extent of treatment required.
Conventional oral exploration (visual and palpation examination) constitutes the gold standard for the diagnosis of oral precancer and cancer; but biopsy and histopathological diagnosis are essential to confirm any diagnosis of cancer. Some specialists advise that the biopsy should be done by the surgeon, and some take several biopsies. If adequate specimens and clinical data are provided by the clinician, the pathologist can perform optimally but, even then, the best pathologists can still err.
Informed consent is mandatory for biopsy as for all operative procedures, particularly noting the likelihood of post-operative discomfort, the possibility of bleeding or bruising, and any possible less transient adverse effects such as post-operative reduction or loss of sensation. Care must be taken not to produce undue anxiety.
Perhaps the most difficult and important consideration is which part of the lesion should be included in the biopsy specimen. As a general rule, the biopsy should include lesional and normal tissue. Any red area should ideally be included in the specimen and, in some potentially malignant lesions where no obvious site can be chosen, vital staining with ‘toluidine blue’ may first be indicated (Article 7). Suspect areas absorb the dye preferentially and stain a deep blue.
Another consideration is whether to use a scalpel or a biopsy punch. When a scalpel is used, a specimen of elliptical shape is usually taken, most commonly from an edge of the lesion. Suturing is usually required. The punch has the advantage that the incision is more controlled, an adequate specimen is still obtained (typically 4 mm or 6 mm diameter) and suturing may not be required.
Complete the histopathology request form with the:
The biopsy specimen container must be labelled clearly with the:
There are also a number of additional techniques that may variously contribute to the diagnosis of oral cancer, as discussed in Article 7.
Differential diagnoses include a chronic infection (Figure 4) or:
