Mirth DB. Controlled-release therapeutic systems: technology applicable to the treatment of oral disease. Adv Dent Res. 1987; 1:109-118
Choudhury M, Needleman I, Gillam D, Moles DR. Systemic and local antimicrobial use in periodontal therapy in England and Wales. J Clin Periodontol. 2001; 28:833-839
Walker CB, Gordon JM, Cornwall HA, Murphy JC, Socransky SS. Gingival crevicular fluid levels of clindamycin compared with its minimal inhibitory concentrations for periodontal bacteria. Antimicrob Agents Chemother. 1981; 19:867-871
Genco RJ. Antibiotics in the treatment of human periodontal diseases. J Periodontol. 1981; 52:545-558
Slots J, Rams TE. Antibiotics in periodontal therapy – advantages and disadvantages. J Clin Periodontol. 1990; 17:479-493
Vandekerckhove BNA, Quirynen M, vanSteenberghe D. The use of tetracycline-containing controlled-release fibers in the treatment of refractory periodontitis. J Periodontol. 1997; 68:353-361
Jain N, Jain GK, Javed S Recent approaches for the treatment of periodontitis. Drug Discovery Today. 2008; 13:932-943
Greenstein G, Tonetti M. The role of controlled drug delivery for periodontitis. The Research, Science and Therapy Committee of the American Academy of Periodontology. J Periodontol. 2000; 71:125-140
Goodson JM. Pharmacokinetics principles controlling efficacy of oral-therapy. J Dent Res. 1989; 68:1625-1632
Cimasoni G. Crevicular fluid updated. Monogr Oral Sci. 1983; 12:III-VII
Needleman IG. Controlled drug release in periodontics – a review of new therapies. Br Dent J. 1991; 170:405-408
Needleman IG, Pandya NV, Smith SR, Foyle DM. The role of antibiotics in the treatment of periodontitis (Part 2 – Controlled drug delivery). Eur J Prosthodont Restor Dent. 1995; 3:111-117
Ainamo J, Lie T, Ellingsen BH Clinical-responses to subgingival application of a metronidazole 25-percent gel compared to the effect of subgingival scaling in adult periodontitis. J Clin Periodontol. 1992; 19:723-729
Goodson JM, Tanner A. Antibiotic-resistance of the subgingival microbiota following local tetracycline therapy. Oral Microbiol Immunol. 1992; 7:113-117
Larsen T. Occurrence of doxycycline resistant-bacteria in the oral cavity after local-administration of doxycycline in patients with periodontal-disease. Scand J Infect Dis. 1991; 23:89-95
Preus HR, Lassen J, Aass AM, Ciancio SG. Bacterial-resistance following subgingival and systemic administration of minocycline. J Clin Periodontol. 1995; 22:380-384
Larsen T, Fiehn NE. Development of resistance to metronidazole and minocycline in vitro. J Clin Periodontol. 1997; 24:254-259
Walker CB, Godowski KC, Borden L The effects of sustained release doxycycline on the anaerobic flora and antibiotic-resistant patterns in subgingival plaque and saliva. J Periodontol. 2000; 71:768-774
Bonito AJ, Lux L, Lohr KN. Impact of local adjuncts to scaling and root planing in periodontal disease therapy: a systematic review. J Periodontol. 2005; 76:1227-1236
Hjeljord LG, Bonesvoll P. Chlorhexidine protein interactions. J Periodontal Res. 1973; 8:11-16
Local drug delivery in the management of periodontal diseases part 1: general principles Jane E Eastham Robin A Seymour Dental Update 2025 41:8, 732-736.
Authors
Jane EEastham
BDS(Hons)
Research Assistant, School of Dental Sciences, Newcastle University, Framlington Place, Newcastle Upon Tyne, NE2 4BW, UK
Dean of Dentistry and Professor of Restorative Dentistry, School of Dental Sciences, Newcastle University, Framlington Place, Newcastle upon Tyne, NE2 4BW, UK
Periodontal pockets provide an ideal environment for the application of local drug delivery for the management of periodontitis. In this first article, consideration is given to the principles that underlie local drug delivery and the pharmacological challenges. It is essential that such systems are compatible with the periodontal tissues. Potential unwanted effects that can arise from both drug and delivery vehicle are also appraised.
Clinical Relevance: Local drug delivery systems still have a place in the management of periodontal diseases. This first article considers the pharmacological principles and unwanted effects that can arise from the use of such systems.
Article
Local drug delivery
A local drug delivery device consists of a drug reservoir and a limiting element that has a control over the amount of active ingredient released. This can be divided into two classes:
Sustained release devices; and
Controlled delivery devices.
The sustained release devices release a drug over a period of 24 hours, whereas the controlled delivery device has duration of drug release greater than 1 day.
Several areas are targeted by locally delivered pharmacological agents in the treatment of periodontal disease. These include the bacteria which reside in the periodontal pocket, the soft tissue walls of the pocket itself and exposed cementum or radicular dentine. The periodontal pocket provides a natural environment which is easily accessible for the positioning of a drug delivery device and offers theoretical benefits to local drug delivery technology, such as:
A well defined and protected site;
Reasonably good access for placement;
The potential for adhesion to the soft and hard tissues.
The delivery device should be able to expand into the volume of the periodontal pocket and remain dimensionally stable.
A local drug delivery device is designed to deliver a pre-determined amount of drug to a specific anatomical site for an extended period of time.1
While local antimicrobial therapy for periodontitis is not widespread, many dentists use this form of therapy and most believe it is more effective than root surface instrumentation (RSI) alone.2
The aim of this paper is to review the local drug delivery systems in the management of periodontal disease.
Local drug delivery versus systemic drug delivery
Systemic antibiotics
Systemic antibiotic use for the treatment of periodontitis has shown some beneficial effects.3,4 In recent years, systemic antimicrobials are mainly recommended for the treatment of aggressive periodontitis.5,6 Multiple systemic doses of these drugs have several drawbacks.7 These include:
An antibiotic concentration that is inadequate at the site of the periodontal pocket;
A rapid decline of the plasma antibiotic concentration to sub-therapeutic levels;
Development of resistant bacteria;
High peak plasma antibiotic concentration that may be associated with side-effects;
Drug interactions and medical contra-indications;
Patient compliance.
Local drug delivery (LDD)
Local drug delivery can avoid most of the problems associated with systemic drug delivery by limiting the amount of drug to its target site with little or no systemic uptake. The local concentration achieved can be much higher (100 x) than is possible via the systemic route. Safe and intrinsically efficacious medications can be delivered into periodontal pockets to suppress or eradicate the pathogenic microbiota or modulate the inflammatory response, thereby limiting tissue destruction. As described by Greenstein and Tonetti,8 local application of pharmacological agents must fulfil three criteria; the medication must:
The main challenge is the ability to maintain effective concentrations of chemotherapeutic agents at the site of action for long periods, despite drug loss from crevicular fluid clearance.8
The gingival crevicular fluid (GCF) provides a leaching medium for the release of a drug and for its distribution throughout the pocket. The characteristics of GCF have been reviewed by Cimasoni.10 Healthy sites are associated with small volumes (0.04 microlitres) and low flow rates (0.03 microlitres per minute). It has been calculated that the turnover rate of gingival fluid is 40 fold per hour.9 Thus, if an antibacterial agent is placed subgingivally, its local concentration rapidly declines. The expected half-life of a pharmacological agent in the gingival crevice is about 1 minute.9 The high rate of clearance is the major obstacle to maintaining effective concentrations of an antimicrobial agent within the pocket. To counteract the continuous loss of drug in the crevicular fluid, a subgingival drug reservoir is required to release the active ingredient at a rate which will counteract its continuous loss due to crevicular fluid flow.8
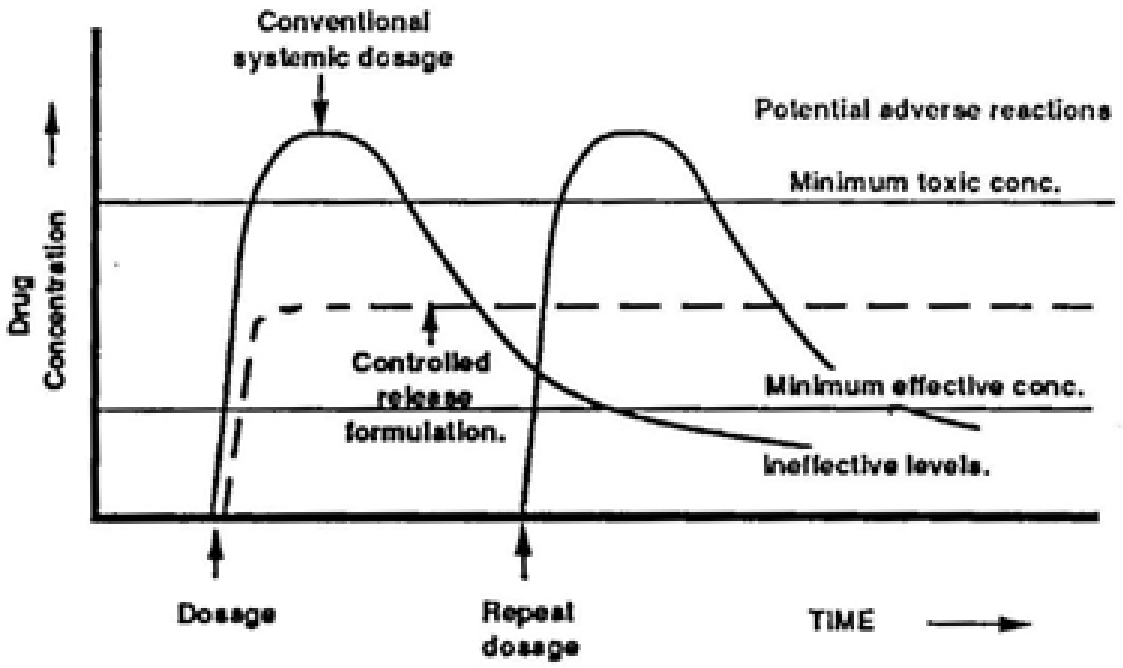
Intrapocket drug delivery systems are desirable due to the potentially lower incidence of unwanted effects, improved efficacy and enhanced patient compliance. The advantages of treating periodontal disease by the intrapocket drug delivery system are based on the fact that high levels of drug can be maintained in the GCF for a prolonged period of time to produce the desirable clinical benefits. LDD devices do not produce fluctuating concentrations typically seen with multiple dose regimens. This is depicted in Figure 1, which compares drug concentrations after systemic dosing when compared to local delivery.11 The transient spikes in drug concentration are not present, therefore the risk of unwanted effects is decreased. The ideal properties of a local drug delivery system are listed in Table 1.
Figure 1. Comparison of drug concentrations resulting from conventional systemic dosage and controlled release formulations.
Easy to use
Cost-effective
Effective against periodontal pathogens
A high viscosity or the ability to result in reduced clearance of the active agent from the periodontal pocket
Anti-inflammatory actions
Effective drug presence: sufficient duration and concentration
Lack of significant unwanted effects
Is biodegradable and biocompatible
Low risk for bacterial resistance
Inhibits collagenases and promotes healing
Inhibits bone resorption
Low systemic absorption
Enhances the effect of scaling and root surface instrumentation
Indications for the use of controlled drug delivery 12
The indications for the use of controlled drug delivery are shown in Table 2. For the most part, these drugs are used as an adjunct to root surface instrumentation (RSI), and this is indicated in the number of studies completed to evaluate efficacy. RSI is necessary for success long term because:
Subgingival plaque and calculus will reduce the ability of the drug to penetrate the pocket tissues;
Residual deposits on the root surface are likely to result in less effective periodontal maintenance;
Residual plaque on the root surface will encourage bacterial repopulation and possible treatment failure.
Sites where pocketing and bleeding on probing persists despite root surface instrumentation and oral hygiene measures
Odd sites of recurrent disease which appear during maintenance
To prolong the life of teeth with a poor prognosis
The acute periodontal abscess – as an adjunct to drainage and RSI
The maintenance of furcation involved teeth
In the management of aggressive periodontitis
Local delivered antimicrobial application into periodontal pockets as a monotherapy offers no advantage over root surface instrumentation.13,14
Concern with respect to the possibility local drug delivery with antibiotics might induce resistant strains of bacteria have been addressed in several studies.15,16,17,18,19 Investigators noted a transient increase in resistant bacteria after administration of local drug delivery. However, after 6 months, there was bacterial repopulation of sites and no detectable increase in the number of resistant strains.
In a systematic review of local adjuncts to RSI in periodontal therapy, it was shown that adjunctive antimicrobial drugs appear to be efficacious.20 The most positive results occurred with tetracycline, minocycline, metronidazole and chlorhexidine(CHX). The systematic review also showed that the adjunctive benefits of LDD increased pocket depth reductions in the range 0.25–0.50 mm.
However, even though the differences were statistically significant, the additional improvement in pocket depth (PD) was a fraction of the reported mean of 1.45 mm after RSI alone. Major clinical attachment level (CAL) gains were in the range 0.10–0.50 mm. These gains were smaller and statistical significance was less common.
Combining PD and CAL results suggests that minocycline might be the most promising adjunctive therapy, followed by tetracycline.20 The effectiveness of adjunctive treatment was greatest in patients with advanced disease.
Contra-indications to local drug delivery systems
Bleeding has an adverse affect on local drug delivery systems. If an LDD device is placed in a periodontal pocket immediately after root surface instrumentation, its efficacy is reduced. This is because the drug binds to the protein in blood hence reducing its activity. A prime example is chlorhexidine, whose activity is reduced in the presence of organic matter such as blood.21 A further unwanted effect can arise if the vehicle degrades into materials which interfere with repair and regeneration of the periodontal tissues.
A possible barrier to the use of LDD in the management of periodontal disease is cost.2 Several LDD agents are now available. The various products together with their active ingredients and cost are shown in Table 3.
Active Ingredient
Chlorhexidine
Tetracycline
Minocycline
Doxycycline
Metronidazole
Azithromycin
Commercial products
PerioChip® £12.50 per chip
Periodontal Plus AB® Cost N/A
Periocline® or Dentomycin® £114
Atridox® £45.50 per syringe
Elyzol® £42.50 (2x 1g applicators)
AZM gel Cost N/A
Chlo-site® £40 per syringe
Arestin® £19.50 per dose
Conclusions
Antimicrobial agents have shown to be of benefit in the management of periodontal diseases. Systemic antimicrobials have numerous drawbacks. Local drug delivery can overcome most of these drawbacks by limiting the drug to its target site with little or no systemic uptake. The high turnover rate of gingival crevicular fluid results in a high rate of clearance, which presents an obstacle to maintaining effective concentrations of an antimicrobial agent within the periodontal pocket. Use of a subgingival drug reservoir releases the antimicrobial to counteract its continuous loss due to GCF flow. Use of locally delivered antimicrobials as a monotherapy provides no benefit over RSI alone. It is important for the clinician to use RSI at the infected pocket sites before administering a local drug delivery device. Local drug delivery is expensive and its benefits have to be weighed against the cost.
Although LDD devices have restricted use in general practice, they may have more indication in specialist periodontal practices. As new drug reservoirs become available, with improved drug release characteristics, the use of local drug delivery in the management of periodontal diseases may become more widespread.