Elliot AJ, Cross KW, Fleming DM Acute respiratory infections and winter pressures on hospital admissions in England and Wales 1990–2005. J Public Health. 2008; 30:91-98
Jordan RE, Hawker JI, Ayres JG, Adab P, Tunnicliffe W, Olowokure B, Kai J, McManus RJ, Salter R, Cheng KK Effect of social factors on winter hospital admission for respiratory disease: a case-control study of older people in the UK. Br J Gen Pract. 2008; 58:400-402
Cheng LH, Newman L Overnight-stay patients in a day surgery unit to overcome shortage of inpatient beds. Br J Oral Maxillofac Surg. 2005; 43:169-172
Jones NP, Hayward JM, Khaw PT, Claoue CM, Elkington AR Function of an ophthalmic “accident and emergency” department: results of a six month survey. Br Med J (Clin Res Ed). 1986; 292:188-190
Anderson R, Thomas DW, Phillips CJ The effectiveness of out-of-hours dental services: II. Patient satisfaction. Br Dent J. 2005; 198:151-156
Mercer SW, Watt GC The inverse care law: clinical primary care encounters in deprived and affluent areas of Scotland. Ann Fam Med. 2007; 5:503-510
Pennycook A, Makower R, Brewer A, Moulton C, Crawford R The management of dental problems presenting to an accident and emergency department. J R Soc Med. 1993; 86:702-703
Lemmens PH, Knibbe RA Seasonal variation in survey and sales estimates of alcohol consumption. J Stud Alcohol. 1993; 54:157-163
Laverick S, Patel N, Jones DC Maxillofacial trauma and the role of alcohol. Br J Oral Maxillofac Surg. 2008; 46:542-546
Fasola AO, Lawoyin JO, Obiechina AE, Arotiba JT Inner city maxillofacial fractures due to road traffic accidents. Dent Traumatol. 2003; 19:2-5
Blatchford O, Capewell S, Murray S, Blatchford M Emergency medical admissions in Glasgow: general practices vary despite adjustment for age, sex, and deprivation. Br J Gen Pract. 1999; 49:551-554
Mittal N, Gupta P Management of extra oral sinus cases: a clinical dilemma. J Endod. 2004; 30:541-547
Celberg L, Linn LS, Rosenberg DJ Dental health of homeless adults. Spec Care Dentist. 1988; 8:167-172
Scribner RA, MacKinnon DP, Dwyer JH The risk of assaultive violence and alcohol availability in Los Angeles County. Am J Public Health. 1995; 85:335-340
Sterk CE, Elifson KW Drug-related violence and street prostitution, 1st edn. In: De La Rosa M, Lambert EY, Gropper B Rockville, MD: National Institute on Drug Abuse; 1990
Allison ME, Wreghitt T, Palmer CR, Alexander GJ Evidence for a link between hepatitis C virus infection and diabetes mellitus in a cirrhotic population. J Hepatol. 1994; 21:1135-1139
Zachariades N, Mezitis M, Anagnostopoulos D Changing trends in the treatment of zygomaticomaxillary complex fractures: a 12-year evaluation of methods used. J Oral Maxillofac Surg. 1998; 56:1152-1156
A festive case series of emergencies, admissions and friendship at a busy oral and maxillofacial unit Ross Keat Paul Leavy Mathew Thomas Dental Update 2024 43:10, 707-709.
Authors
RossKeat
BDS, MFDS, PgCert
DCT in Oral and Maxillofacial Surgery, Sheffield Teaching Hospital NHS Foundation Trust, Charles Clifford Dental Hospital, Wellesley Road, Sheffield S10 2SZ, UK (rosskeat@gmail.com)
DCT in Oral and Maxillofacial Surgery, Sheffield Teaching Hospital NHS Foundation Trust, Charles Clifford Dental Hospital, Wellesley Road, Sheffield S10 2SZ, UK
Specialty Registrar in Oral and Maxillofacial Surgery, Sheffield Teaching Hospital NHS Foundation Trust, Charles Clifford Dental Hospital, Wellesley Road, Sheffield S10 2SZ, UK
The festive season presents oral and maxillofacial surgery (OMFS) dental core trainees (DCTs) with the challenges of managing an eclectic mix of emergencies. We present three such patients in this case series. First, Patient A, a 39-year-old homeless male who presented with a maxillary extra-oral draining sinus. Secondly, Patient B, a 38-year-old intra-venous (IV) drug user who suffered pan-facial fractures following an alcohol-fuelled assault. Finally, Patient C, a 38-year-old male who sustained a left zygomatic complex fracture a week previously, in attendance for corrective surgery. Despite the hardship, there was still festive cheer to be had by these individuals.
CPD/Clinical Relevance: Primary and secondary care practitioners should be aware of the advanced clinical presentation of dental and maxillofacial emergencies that occur over holiday periods.
Article
The winter and Christmas period often sees a surge in admissions at many hospitals, when in-patient demand for beds frequently outweighs capacity.1 This is no different for OMFS units.2,3 Emergency Departments (EDs) are often the first port of call for patients who have sustained maxillofacial injuries, similar to findings in ophthalmology.4 Patients who experience dental emergencies when their regular dental practice is closed may attend out of hours (OOHs) primary care services. There is, however, evidence to suggest that perceived or actual challenges in accessing walk-in services during OOHs periods may act as a barrier to patients accessing such services.5 When patients cannot readily access primary care dental services, they may attend their local ED department for treatment. This is particularly true for the socioeconomically deprived.6 ED-based, medically qualified professionals may not have sufficient training in managing dento-facial emergencies,7 therefore it is the role of the OMFS team to provide care for individuals who present with dental as well as maxillofacial emergencies.
Increased alcohol consumption during the festive period is well documented, as is the link between alcohol consumption and maxillofacial trauma.8,9 The link between road traffic accidents leading to maxillofacial trauma during the Christmas period has also been documented.10 We present a summary of three cases, all OMFS in-patients at Sheffield Teaching Hospitals, who were managed during the Christmas period in 2015.
Case reports
Patient A, a 39-year-old male of Afro-Caribbean descent, presented with a left maxillary swelling and associated extra-oral discharging sinus (Figure 1). Of note, his social history included alcohol and nicotine dependence and homelessness. On examination, an intra-oral maxillary swelling in the upper left premolar region was tender on palpation with active, purulent discharge evident extra-orally. During the Christmas period, the patient had been unable to visit his regular dentist and he expressed dissatisfaction with the care offered by the local OOHs dental service. As the swelling worsened, he admitted that he did not have sufficient funds to re-attend the OOHs dental service and, therefore, he presented to the ED. He was discharged from the ED without OMFS input 12 hours prior to re-attending with a significantly increased facial swelling. An OPG radiograph revealed a grossly carious dentition for which the patient received intra-venous antibiotic therapy followed by incision and drainage and multiple extractions under general anesthetic. In a fitting fashion, his sole request was to maintain his central incisors.
Figure 1. Patient A, showing the location of his extra-oral draining sinus.
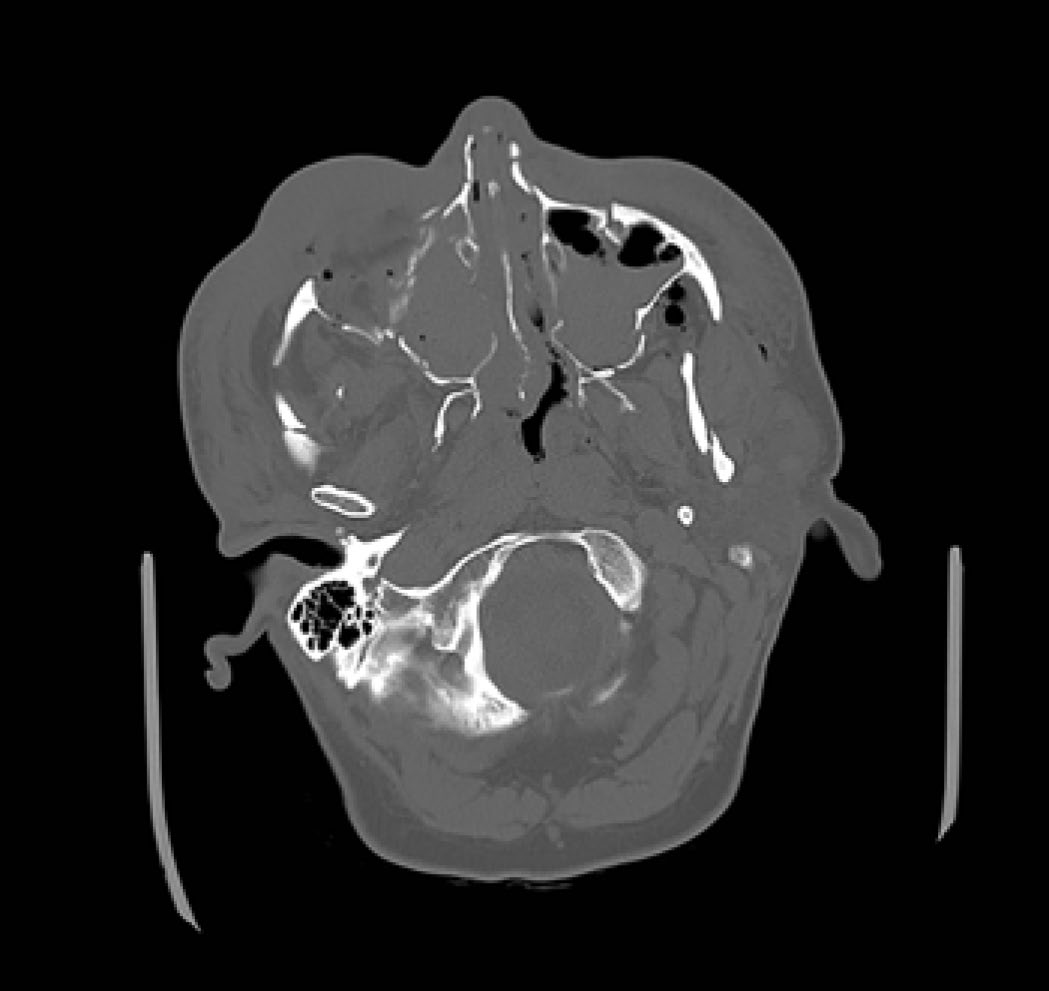
Patient B, a 38-year-old Caucasian male, presented in the early hours of Boxing Day (26 December 2015) having been referred from the ED following an alleged assault that left him with multiple facial fractures. Medically, the patient was hepatitis C positive with poorly controlled type 2 diabetes. His social history included nicotine dependency and a long-term history of intravenous drug abuse. Despite his extensive injuries, he presented with a Glasgow Coma Scale score of 15 with no reduction in cranial nerve function. Imaging revealed widespread, comminuted fractures, including Le Fort III, displaced orbital floors and left mandibular angle and condylar fractures (Figures 2 and 3).
Figure 2. A computed tomography (CT) scan slice of patient B, demonstrating multiple pan-facial fractures.Figure 3. A posterior-anterior mandible view of patient B, where the fractured left mandibular angle and condyle are visible.
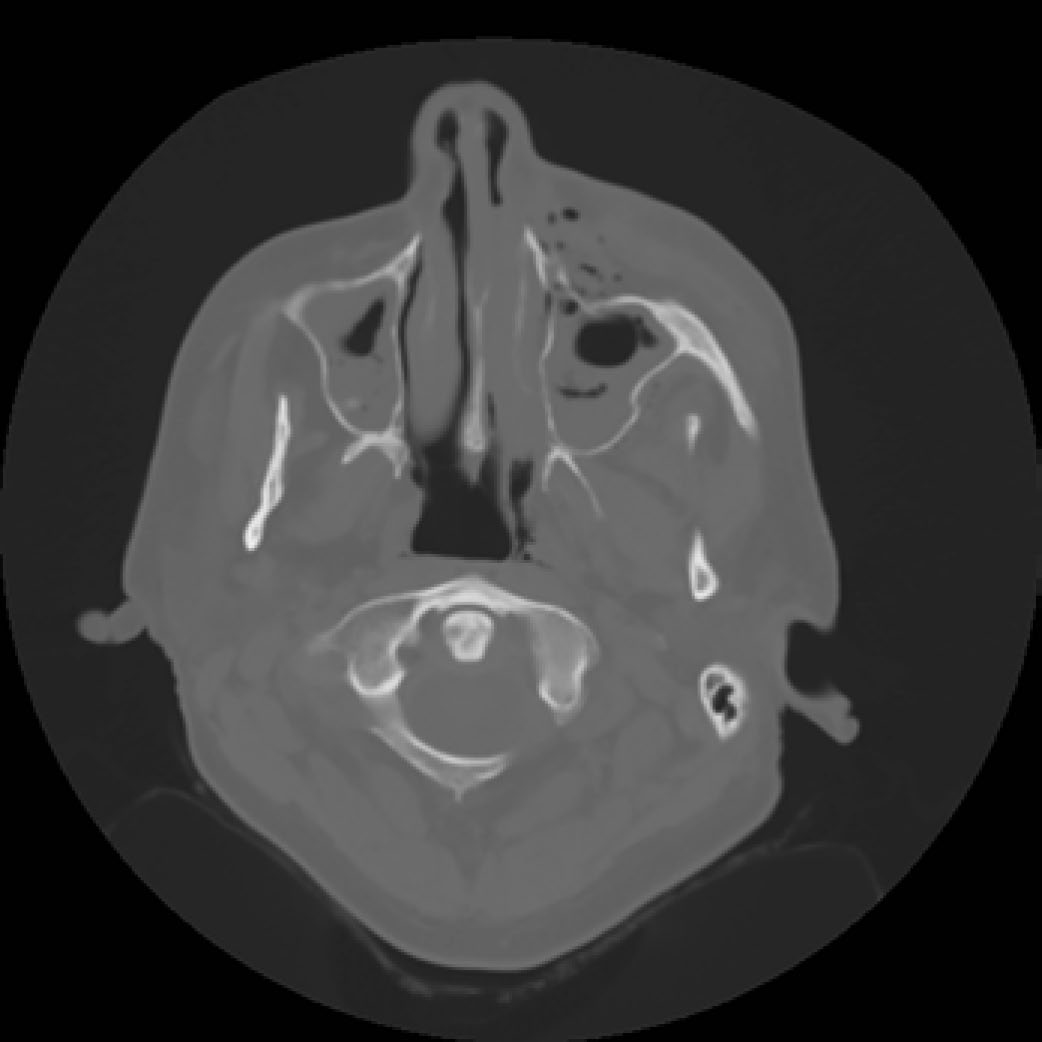
Finally, Patient C, a 38-year-old Caucasian male, presented to the OMFS unit five days following a road traffic accident for a planned left zygomatic arch lift (Figure 4). His medical history included poorly controlled epilepsy. Indeed, the patient experienced five epileptic seizures on the day of his admission, which resulted in surgery being postponed until his condition was brought under control. The patient had no evidence of eye injury or muscle entrapment, and his sole complaint was of a small area of paraesthesia to the left cheek. All three patients underwent surgical procedures on the same day, 27 December 2015.
Figure 4. A computed tomography (CT) scan slice of patient C, showing a depressed fracture to the anterior wall of the left maxillary sinus.
Discussion
Each of these subjects was from a low socioeconomic background. Patient A was of no fixed abode, while Patients B and C were unemployed and in receipt of social welfare payments. Those from lower social classes are referred from primary care more often than those from higher socioeconomic backgrounds.11
In the absence of suitable primary care services over the Christmas period, Patient A's condition had deteriorated to such an extent that it required surgical intervention. Studies have shown that extra-oral draining sinuses of dental origin can be prevented and treated in the early stages through successful endodontic management or extraction in primary care, precluding the need for surgical intervention.12 Inadequate dental care amongst the homeless is endemic, with this sector of society having a higher incidence of dental caries and missing teeth, higher use of tobacco and fewer dental visits compared to the general population.13 It should be noted that, whilst emergency surgical intervention may not be the dental treatment of choice, in Patient A's case it allowed for the formulation of a treatment plan which included extraction of non-viable teeth. This was paramount in the prevention of further episodes of pain and sepsis.
Patient B was subject to an alleged assault whilst under the influence of alcohol. There is widespread evidence to suggest that alcohol consumption is related to increased incidence of violent assault.14 As this patient had a history of intravenous drug abuse, it is also important to note the link between drug abuse and violent crime.15 Furthermore, the patient was hepatitis C positive and suffered from poorly controlled diabetes – a link between these conditions has been found, but the mechanism is poorly understood.16 Owing to the severity of Patient B's craniofacial injuries, he required an elective tracheostomy to ensure a patent airway post-surgery. Multidisciplinary input was therefore required for this particular in-patient episode, including from the OMFS and neurosurgery teams, speech and language therapists, endocrinologists and dietitians. Such input allowed each aspect of Patient B's overall health to be monitored and managed appropriately during his in-patient episode.
Patient C attended the department requiring a routine zygomatic complex fracture reduction under general anaesthetic. This fracture was not fixated, however, semi-fixation with mini plates has been shown to be the most reliable method for treatment of zygomatic complex fractures.17 Despite this, subsequent imaging of this patient has shown adequate healing of the zygomatic complex and the patient was happy with the aesthetic outcome.
The happy coincidence in the case series comes from the inclusion of Patient C, who attended the same school as Patient B. They were close friends until losing contact with one another seven years earlier. Their admission onto the OMFS ward allowed them to enjoy the festive period together and rekindle an old friendship.
Conclusion
Christmas is a time for family, friends, celebration and, all too often, hospital admission for OMFS emergencies. Awareness among dental and medical practitioners of the potential for reduced access to primary care dental services during the Christmas period is important. Patients with significant dental emergencies may present to the secondary care setting during this busy period. Therefore, ensuring that adequate access to appropriate primary care is available to all in the run-up to holiday periods should be at the forefront of practitioners' and healthcare policy makers' minds alike. Practitioners should be aware of the dento-alveolar injuries that can present secondary to alcohol consumption. A logarithm for the management of dental emergencies could be utilized in EDs to ensure that referrals to OMFS units are made in a timely manner. This could aid in avoiding significant escalation of readily preventable conditions.
The multidisciplinary approach to care which was adopted for these patients resulted in beneficial outcomes; in this instance, such teamwork allowed us to help one of those who needed it the most, alongside treating and reuniting two old friends.