Hellstein JW, Adler RA, Edwards BJ Managing the care of patients receiving antiresorptive therapy for prevention and treatment of osteoporosis: executive summary of recommendations from the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2011; 142:1243-1251
Ruggiero SL, Dodson TB, Fantasia J American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw – 2014 update. J Oral Maxillofac Surg. 2014; 72:1938-1956
Khan AA, Sandor GK, Dore E Canadian consensus practice guidelines for bisphosphonate associated osteonecrosis of the jaw. J Rheumatol. 2008; 35:1391-1397
Edwards BJ, Hellstein JW, Jacobsen PL Updated recommendations for managing the care of patients receiving oral bisphosphonate therapy: an advisory statement from the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2008; 139:1674-1677
Migliorati CA, Casiglia J, Epstein J Managing the care of patients with bisphosphonate-associated osteonecrosis. An American Academy of Oral Medicine position paper. J Am Dent Assoc. 2005; 136:1658-1668
Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg. 2003; 61:1115-1117
Pazianas M. Osteonecrosis of the jaw and the role of macrophages. J Natl Cancer Inst. 2011; 103:232-240
Marx RE, Sawatari Y, Fortin M Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: risk factors, recognition, prevention and treatment. J Oral Maxillofac Surg. 2005; 63:1567-1575
Woo S, Hellstein JW, Kalmar JR. Systematic review: bisphosphonates and osteonecrosis of the jaw. Ann Intern Med. 2006; 144:754-761
Durie BGM, Katz M, Crowley J. Osteonecrosis of the jaws and bisphosphonates [Letter]. N Engl J Med. 2005; 353
Bamias A, Kastritis E, Bamia C Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: incidence and risk factors. J Clin Oncol. 2005; 23
Hoff AO, Toth BB, Altundag K Osteonecrosis of the jaw in patients receiving intravenous bisphosphonate therapy. J Clin Oncol. 2006; 24
Henry DH, Costa L, Goldwasser F Randomized, double-blind study of denosumab versus zoledronic acid in the treatment of bone metastases in patients with advanced cancer (excluding breast and prostate cancer) or multiple myeloma. J Clin Oncol. 2011; 29
Saad F, Brown JE, Van Poznak C Incidence, risk factors, and outcomes of osteonecrosis of the jaw: integrated analysis from three blinded active-controlled phase III trials in cancer patients with bone metastases. Ann Oncol. 2012; 23
Jadu F, Lee L, Pharoah M A retrospective study assessing the incidence, risk factors and comorbidities of pamidronate-related necrosis of the jaws in multiple myeloma patients. Ann Oncol. 2007; 18:2015-2019
Lo JC, O'Ryan FS, Gordon NP Prevalence of osteonecrosis of the jaw in patients with oral bisphosphonate exposure. J Oral Maxillofac Surg. 2010; 68
Nicoletti P, Cartsos VM, Palaska PK Genomewide pharmacogenetics of bisphosphonate-induced osteonecrosis of the jaw: the role of RBMS3. Oncologist. 2012; 17
Qi WX, Tang LN, He AN Risk of osteonecrosis of the jaw in cancer patients receiving denosumab: a meta-analysis of seven randomized controlled trials. Int J Clin Oncol. 2014; 19:403-410
Coleman R, Woodward E, Brown J Safety of zoledronic acid and incidence of osteonecrosis of the jaw (ONJ) during adjuvant therapy in a randomised phase III trial (AZURE: BIG 01-04) for women with stage II/III breast cancer. Breast Cancer Res Treat. 2011; 127
Mauri D, Valachis A, Polyzos IP Osteonecrosis of the jaw and use of bisphosphonates in adjuvant breast cancer treatment: a meta-analysis. Breast Cancer Res Treat. 2009; 116
Vahtsevanos K, Kyrgidis A, Verrou E Longitudinal cohort study of risk factors in cancer patients of bisphosphonate-related osteonecrosis of the jaw. J Clin Oncol. 2009; 27:53-56
Scagliotti GV, Hirsh V, Siena S Overall survival improvement in patients with lung cancer and bone metastases treated with denosumab versus zoledronic acid: subgroup analysis from a randomized phase 3 study. J Thorac Oncol. 2012; 7
Guarneri V, Miles D, Robert N Bevacizumab and osteonecrosis of the jaw: incidence and association with bisphosphonate therapy in three large prospective trials in advanced breast cancer. Breast Cancer Res Treat. 2010; 122
Felsenberg D, Hoffmeister B. [Necrosis of the jaw after high-dose bisphosphonate therapy.]. Kiefernekrosen nach hoch dosierter Bisphosphonattherapie. Dtsch Arztebl. 2006; 103
Malden N, Lopes V. An epidemiological study of alendronate-related osteonecrosis of the jaws. A case series from the south-east of Scotland with attention given to case definition and prevalence. J Bone Miner Metab. 2012; 30
Grbic JT, Black DM, Lyles KW The incidence of osteonecrosis of the jaw in patients receiving 5 milligrams of zoledronic acid: data from the health outcomes and reduced incidence with zoledronic acid once yearly clinical trials program. J Am Dent Assoc. 2010; 141
Papapoulos S, Chapurlat R, Libanati C Five years of denosumab exposure in women with postmenopausal osteoporosis: results from the first two years of the FREEDOM extension. J Bone Miner Res. 2012; 27
Kyrgidis A, Vahtsevanos K, Koloutsos G Bisphosphonate-related osteonecrosis of the jaws: a case–control study of risk factors in breast cancer patients. J Clin Oncol. 2008; 26:4634-4638
Barba-Recreo P, Del Castillo Pardo de Vera JL, García-Arranz M. Zoledronic acid-related osteonecrosis of the jaws. Experimental model with dental extractions in rats. J Craniomaxillofac Surg. 2014; 42:744-750
Badros A, Weikel D, Salama A Osteonecrosis of the jaw in multiple myeloma patients: clinical features and risk factors. J Clin Oncol. 2006; 24
Assael LA. Oral bisphosphonates as a cause of bisphosphonate-related osteonecrosis of the jaws: clinical findings, assessment of risks and preventive strategies. J Oral Maxillofac Surg. 2009; 67:35-43
López-Jornet P, Camacho-Alonso F, Martínez-Canovas A Perioperative antibiotic regimen in rats treated with pamidronate plus dexamethasone and subjected to dental extraction: a study of the changes in the jaws. J Oral Maxillofac Surg. 2011; 69:2488-2493
Ferlito S, Puzzo S, Liardo C. Preventive protocol for tooth extractions in patients treated with zoledronate: a case series. J Oral Maxillofac Surg. 2011; 69:e1-e4
Montefusco V, Gay F, Spina F Antibiotic prophylaxis before dental procedures may reduce the incidence of osteonecrosis of the jaw in patients with multiple myeloma treated with bisphosphonates. Leuk Lymph. 2008; 49:2156-2162
Bagán J, Blade J, Cozar JM Recommendations for the prevention, diagnosis, and treatment of osteonecrosis of the jaw (ONJ) in cancer patients treated with bisphosphonates. Med Oral Patol Oral Cir Bucal. 2007; 12:e336-e400
Regev E, Lustmann J, Nashef R. Atraumatic teeth extraction in bisphosphonate-treated patients. J Oral Maxillofac Surg. 2008; 66:1157-1161
Hoefert S, Grimm M, Sharghi F Atraumatic tooth extraction in patients taking bisphosphonates: a review of literature and experience with three cases. Oral Maxillofac Surg. 2014; 18:341-349
Damm DD, Jones DM. Bisphosphonate-related osteonecrosis of the jaws: a potential alternative to drug holidays. Gen Dent. 2013; 61
Malan J, Ettinger K, Naumann E The relationship of denosumab pharmacology and osteonecrosis of the jaws. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012; 114:671-676
Tsao C, Darby I, Ebeling PR Oral health risk factors for bisphosphonate-associated jaw osteonecrosis. J Oral Maxillofac Surg. 2013; 71:1360-1366
Badros A, Weikel D, Salama A Osteonecrosis of the jaw in multiple myeloma patients: clinical features and risk factors. J Clin Oncol. 2006; 24:945-952
Sedghizadeh PP, Kumar SK, Gorur A Identification of microbial biofilms in osteonecrosis of the jaws secondary to bisphosphonate therapy. J Oral Maxillofac Surg. 2008; 66:767-775
Aguirre I, Akhter MP, Kimmel DB Oncologic doses of zoledronic acid induce osteonecrosis of the jaw-like lesions in rice rats (Oryzomys palustris) with periodontitis. J Bone Min Res. 2012; 27:2130-2143
Aghaloo TL, Kang B, Sung EC Periodontal disease and bisphosphonates induced osteonecrosis of the jaws in the rat. J Bone Min Res. 2011; 26:1871-1882
Kang B, Cheong S, Chaichanasakul T Periapical disease and bisphosphonates induced osteonecrosis of the jaws in mice. J Bone Min Res. 2013; 28:1631-1640
Yamazaki T, Yamori M, Ishizaki T. Increased incidence of osteonecrosis of the jaw after tooth extraction in patients treated with bisphosphonates: a cohort study. Int J Oral Maxillofac Surg. 2012; 41:1397-1403
Reddy MS, Weatherford TW, Smith CA Alendronate treatment of naturally-occurring periodontitis in beagle dogs. J Periodontol. 1995; 66:211-217
Weinreb M, Quartuccio H, Seedor JG Histo-morphometrical analysis of the effects of the bisphosphonate alendronate on bone loss caused by experimental periodontitis in monkeys. J Periodontal Res. 1994; 29:35-40
Yaffe A, Herman A, Bahar H Combined local application of tetracycline and bisphosphonate reduces alveolar bone resorption in rats. J Periodontol. 2003; 74:1038-1042
Lane N, Armitage GC, Loomer P Bisphosphonate therapy improves the outcome of conventional periodontal treatment: results of a 12-month, randomized, placebo-controlled study. J Periodontol. 2005; 76:1113-1122
Rocha ML, Malacara JM, Sanchez-Marin FJ Effect of alendronate on periodontal disease in postmenopausal women: a randomized placebo-controlled trial. J Periodontol. 2004; 75:1579-1585
Pradeep AR, Kumari M, Rao NS 1% alendronate gel as local drug delivery in the treatment of Class II furcation defects: a randomized controlled clinical trial. J Periodontol. 2013; 84:307-315
Sharma A, Pradeep AR. Clinical efficacy of 1% alendronate gel in adjunct to mechanotherapy in the treatment of aggressive periodontitis: a randomized controlled clinical trial. J Periodontol. 2012; 83:19-26
Ficarra G, Beninati F, Rubino I Osteonecrosis of the jaws in periodontal patients with a history of bisphosphonates treatment. J Clin Periodontol. 2005; 32:1123-1128
Khosla S, Burr D, Cauley J Bisphosphonate-associated osteonecrosis of the jaw: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2007; 22:1479-1491
Madrid C, Sanz M. What impact do systemically administrated bisphosphonates have on oral implant therapy? A systemic review. Clin Oral Implants Res. 2009; 20:87-95
Fugazzotto PA, Lightfoot WS, Jaffin R Implant placement with or without simultaneous tooth extraction in patients taking oral bisphosphonates: postoperative healing, early follow-up, and the incidence of complications in two private practices. J Periodonol. 2007; 78:1664-1669
Grant BT, Amenedo C, Freeman K Outcomes of placing dental implants in patients taking oral bisphosphonates: a review of 115 cases. J Oral Maxillofac Surg. 2008; 66:223-230
Memon S, Weltman RL, Katancik JA. Oral bisphosphonates: early endosseous dental implant success and crestal bone changes. A retrospective study. Int J Oral Maxillofac Implants. 2012; 27:1216-1222
Wang HL, Weber D, McCauley LK. Effect of long-term oral bisphosphonates on implant wound healing: literature review and a case report. J Periodontol. 2007; 78:584-594
Yip JK, Borrell LN, Cho SC Association between oral bisphosphonate use and dental implant failure among middle-aged women. J Clin Periodontol. 2012; 39:408-414
López-Cedrún JL, Sanromán JF, García A Oral bisphosphonate-related osteonecrosis of the jaws in dental implant patients: a case series. Br J Oral Maxillofac Surg. 2013; 51:874-879
Shirota T, Nakamura A, Matsui Y Bisphosphonate-related osteonecrosis of the jaw around dental implants in the maxilla: report of a case. Clin Oral Implants Res. 2009; 20:1402-1408
Bedogni A, Bettini G, Totola A Oral bisphosphonate-associated osteonecrosis of the jaw after implant surgery: a case report and literature review. J Oral Maxillofac Surg. 2010; 68:1662-1666
Allen MR, Burr DB. The pathogenesis of bisphosphonate-related osteonecrosis of the jaw: so many hypotheses, so few data. J Oral Maxillofac Surg. 2009; 67
Lazarovici TS, Yahalom R, Taicher S Bisphosphonate-related osteonecrosis of the jaw associated with dental implants. J Oral Maxillofac Surg. 2010; 68:790-796
Kim I, Ki H, Lee W The effect of systemically administered bisphosphonates on bony healing after tooth extraction and osseointegration of dental implants in the rabbit maxilla. Int J Oral Maxillofac Implants. 2013; 28
Abtahi J, Agholme F, Sandberg O Effect of local vs. systemic bisphosphonate delivery on dental implant fixation in a model of osteonecrosis of the jaw. J Dent Res. 2013; 92:279-283
Tengvall P, Skoglund B, Askendal A Surface immobilized bisphosphonate improves stainless-steel screw fixation in rats. Biomaterials. 2004; 25:2133-2138
Kettenberger U, Ston J, Thein E Does locally delivered Zoledronate influence peri-implant bone formation? – Spatio-temporal monitoring of bone remodeling in vivo. Biomaterials. 2014; 35:9995-10006
Abtahi J, Tengvall P, Aspenberg P. A bisphosphonate-coating improves the fixation of metal implants in human bone. A randomized trial of dental implants. Bone. 2012; 50:1148-1151
Wermelin K, Suska F, Tengvall P Stainless steel screws coated with bisphosphonates gave stronger fixation and more surrounding bone. Histomorphometry in rats. Bone. 2008; 42:365-371
Periodontal disease, dental implants, extractions and medications related to osteonecrosis of the jaws Neha P Shah Helen Katsarelis Michael Pazianas Daljit K Dhariwal Dental Update 2024 42:9, 707-709.
Authors
Neha PShah
BDS
Specialty Dentist, Department of Oral Surgery, Guy's Hospital, London
Patients taking bisphosphonates and other anti-resorptive drugs are likely to attend general dental practice. The term ‘bisphosphonate’ is often immediately associated with osteonecrosis of the jaws (ONJ). Risk assessment and subsequent management of these patients should be carried out taking into account all the risk factors associated with ONJ. The introduction of newer drugs, also shown to be associated with ONJ, demands increased awareness of general dental practitioners about these medications.
CPD/Clinical Relevance: This paper provides an update on medication-related ONJ and considers the effects of anti-resorptive drugs on the management of patients needing exodontia, treatment for periodontal disease and dental implant placement.
Article
Routine medical history screening in general dental practice will reveal patients taking nitrogen-containing bisphosphonates (N-BPs) and other anti-resorptive drugs, used most commonly in oncology patients with metastatic disease and in the treatment of osteoporosis in post-menopausal women. The term ‘bisphosphonates’ (BPs) can immediately prompt concerns of drug-related osteonecrosis of the jaws (ONJ), a reported complication of certain drug groups; N-BPs being the most documented family of drugs associated with a higher risk. Recently approved anti-resorptive agents, such as denosumab and other anti-angiogenic drugs used in oncology, have also been associated with ONJ and are expected to be used increasingly in the future; hence the American Dental Association Council on Scientific Affairs expert panel proposed all cases of ONJ related to the administration of anti-resorptive therapeutic agents to be termed ‘anti-resorptive agent-induced ONJ’ (ARONJ) in 2011;1 this term has now been updated to ‘medication-related ONJ’ (MRONJ) by the American Association of Oral and Maxillofacial Surgeons (AAOMS),2 allowing inclusion of the effects of anti-angiogenic agents.
Currently there are no guidelines from British institutions on the management of patients taking drugs associated with ONJ. Expert panels from other countries, however, have produced recommendations on the management of these patients.2,3,4,5,6 The aim of this article is to revise ONJ, and to review the current literature on the potential effects of anti-resorptive drugs on the management of patients needing exodontia, treatment for periodontal disease and dental implant placement.
MRONJ: Diagnosis, aetiology, epidemiology and risk factors
The diagnosis of MRONJ is based on the presence of exposed bone or bone that can be probed through an intra-oral or extra-oral fistula(e) in the maxillofacial region that has persisted for more than eight weeks in the absence of radiotherapy or obvious metastatic disease to the jaw, on a background of current or previous treatment with anti-resorptive or anti-angiogenic agents.2 The AAOMS have produced a recommended staging system for MRONJ (Table 1).
Stage
Characteristics
At risk category
No apparent necrotic bone in patients who have been treated with either oral or IV bisphosphonates
Stage 0
No clinical evidence of necrotic bone, but non-specific clinical findings, radiographic changes or symptoms
Stage 1
Exposed and necrotic bone, or fistulae that probes to bone, in patients who are asymptomatic and have no evidence of infection
Stage 2
Exposed and necrotic bone, or fistulae that probes to bone, associated with infection as evidenced by pain and erythema in the region of the exposed bone with or without purulent drainage
Stage 3
Stage 2 patients and one or more of the following: exposed and necrotic bone extending beyond the region of alveolar bone (ie inferior border and ramus in the mandible, maxillary sinus and zygoma in the maxilla) resulting in pathologic fracture, extra-oral fistula, oral antral/oral nasal communication, or osteolysis extending to the inferior border of the mandible or sinus floor
The first case of ONJ-related to bisphosphonate use (BRONJ) was reported in 2003,7 though the full pathophysiological mechanism(s) of MRONJ is (are) yet to be fully understood. Current theories are centred on the drug's inhibitory role on osteoclastic bone resorption that affects bone remodeling, endothelial cell angiogenesis (certain drugs) and the presence of infection and/or inflammation.8
MRONJ is more commonly associated with the mandible compared to the maxilla (2:1) but can also affect both jaws in any one particular patient.9,10 The published incidence of MRONJ varies (Table 2). Oncology patients are at a higher risk for MRONJ than those treated for osteoporosis since the anti-resorptive drugs used in this group are administered at higher doses, more frequently (ie monthly in oncology versus yearly or 6-monthly in osteoporosis indications) and parenteral administration allows greater drug exposure11,12,13 (Table 2). Increased duration of the drug therapy has been reported as a risk factor for ONJ related to denosumab,14,15 IV N-BPs14 and oral N-BP use,16,17,18 as has concomitant corticosteroid use.15 Information on the association of ONJ with anti-angiogenic agents (in the absence of bisphosphonate therapy) is limited to case reports, and the incidence from a large analysis of patients treated with bevacizumab has been quoted in Table 2. The presence of certain genes19 and other medical co-morbidities, such as anaemia and diabetes,15 have been mentioned as risk factors, however further research is needed in these areas.
*It must be noted that incidences vary with the size of the studies; detailed investigation of each study is strongly advised.
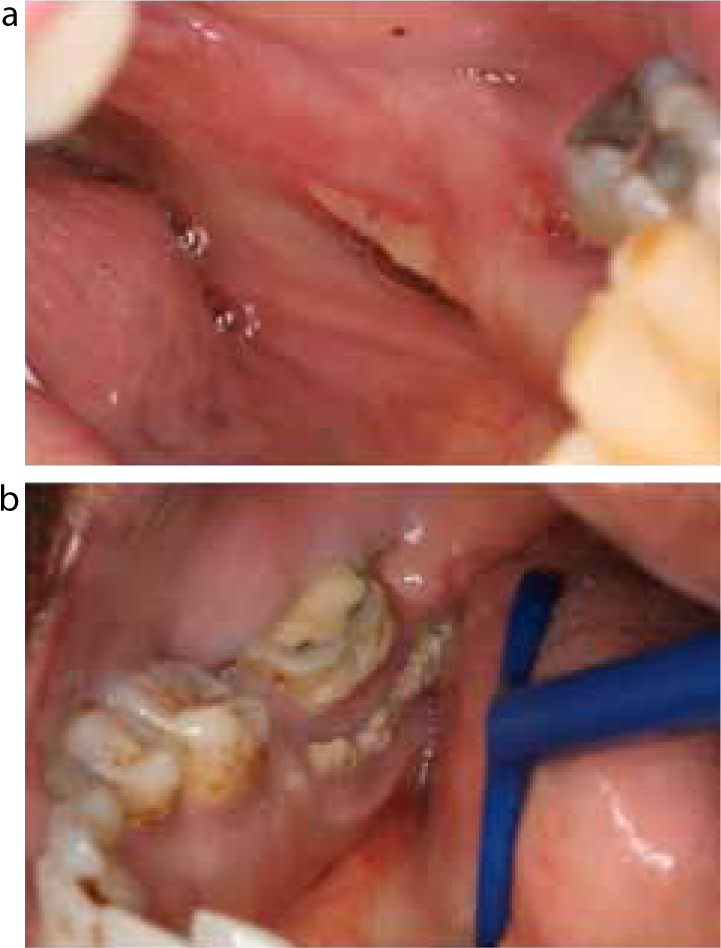
In addition to these systemic factors, local risk factors include denture wearing23 (Figure 1a and 2), the presence of inflammation or infection in the structures supporting the teeth4,30 and procedures stimulating the bone around the teeth, such as extractions (Figure 3), implant placement, and periodontal treatment; all of which are procedures commonly carried out in general dental practice. The second part of this article addresses the risk of ONJ for these procedures in patients on anti-resorptive drugs, predominantly N-BPs.
Figure 1.
(a) MRONJ in the lingual sulcus of a denture wearer who had a history of 3 years of alendronate therapy; stage 1. (b) MRONJ in a similar region in a non-denture wearer who had a history of 90 doses of zometa; stage 1.Figure 2. MRONJ lesion in the anterior maxilla of a patient with a history of 57 doses of zometa. Despite the size of the lesion, this patient was asymptomatic and there was no evidence of infection on clinical examination; stage 1.Figure 3. Post-dental extraction MRONJ; stage 2 based on symptoms of pain, and signs of exposed bone, erythema and a purulent discharge on clinical examination.
Extractions (and other dento-alveolar surgery)
Dental extractions have been used in animal ONJ models31 and dento-alveolar surgery has been suggested as an inciting event for the development of ONJ in patients on anti-resorptive drugs.9,15,23,30,32 In one example, in a case control study of cancer patients exposed to anti-resorptive drugs, patients with a history of tooth extraction were associated with a 16-fold increased risk for ONJ when compared to cancer patients without ONJ,30 implicating the tooth extraction as a risk factor itself in addition to the IV use of the anti-resorptive agent. In addition to the extraction process causing local trauma, the presence and contribution of dental infection to the development of ONJ should not be excluded from the equation, as most dental extractions are carried out on teeth with periodontal disease or periapical pathology.
Although the risk of ONJ is much smaller in patients on oral N-BPs, there have been numerous cases of ONJ in patients taking oral BPs33 and, as previously discussed, other systemic and/or local factors can increase this risk, such as greater than 4 years of BP therapy or concomitant corticosteroid or anti-angiogenic medication use. Recommendations by AAOMS for oral surgery in patients on oral BPs have been summarized in Table 3.
Oral bisphosphonates (BPs): Recommendations by AAOMS
Prior to starting anti-resorptives for osteoporosis:
Education of the potential risks of MRONJ as the anti-resorptive therapy is likely to exceed beyond 4 years of treatment
Emphasis on the importance of optimizing dental health throughout this treatment period
If implants are to be considered, informed consent should be provided related to the long-term possibility of implant failure and low risk of developing ONJ if the anti-resorptive is continued. Regular review and discussion with the prescribing physician to consider alternate dosing of the BPs, drug holidays, or an alternative to the BP therapy is advised
Oral BPs < 4 years and have no clinical risk factors*
No alteration or delay in the planned surgery (all procedures common to oral and maxillofacial surgeons, periodontists and other dental providers)
Oral BPs < 4 years and have also taken corticosteroids or anti-angiogenic medications concomitantly
Liaise with the prescribing provider to consider drug holiday for at least 2 months prior to oral surgery, if systemic conditions permit
Anti-resorptive should not be restarted until osseous healing has occurred
Oral BPs > 4 years and with or without any concomitant medical therapy
Liaise with the prescribing provider to consider drug holiday for at least 2 months prior to oral surgery, if systemic conditions permit
Anti-resorptive should not be restarted until osseous healing has occurred
*eg concomitant use of corticosteroid or anti-angiogenic medications.
Patients with a background of intravenous administration of anti-resorptive or anti-angiogenic agents, especially cancer patients, should be treated with extreme caution and careful planning, often with multidisciplinary input. For this group of patients, AAOMS recommend:
Where possible, delay the start of intravenous anti-resorptive or anti-angiogenic treatment for cancer therapy in order to optimize dental health, including extraction of non-restorable teeth and those of poor prognosis and any other necessary elective dento-alveolar surgery. If systemic conditions permit, delay the therapy until the extraction site has undergone mucosalization (14–21 days) or until there is adequate osseous healing.
Avoid procedures that involve direct osseous injury and non-restorable teeth may be treated by removal of the crown and endodontic treatment of the remaining roots.
In many circumstances, dento-alveolar surgery cannot be avoided. Studies have looked at other factors such as pre- and post-operative antibiotic treatment, antibacterial mouthwashes, drug holidays and alternative methods of exodontia that could potentially reduce the risk of ONJ in patients undergoing dento-alveolar surgery whilst taking BPs.
Antibiotics
To date there is no clear consensus for the use of peri-operative antibiotics during dento-alveolar surgery in the prevention of BRONJ. A study on rats treated with pamidronate and dexamethasone with and without (control) perioperative antibiotics undergoing dento-alveolar surgery demonstrated a significant decrease in BRONJ34 when antibiotics were used. A case series of 43 oncology patients with a history of zoledronate therapy underwent single or multiple extractions with a preventive protocol consisting of the removal of alveolar bone supported with antimicrobial therapy (antibiotics and mouthwash) showed encouraging results with no evidence of BRONJ at 12 month follow up.35 The average duration of BP therapy was, however, only 16.2 months and there were no controls in this study. Similarly, in a retrospective analysis of multiple myeloma patients receiving IV BP, when comparing ‘high risk’ procedures (eg tooth extraction) carried out with antibiotic prophylaxis to ‘high risk’ procedures without prophylaxis, it was found that patients in the first group (prophylaxis group) had a significantly reduced the risk of ONJ (p = 0.012).36 The prophylaxis regimen used in this study consisted of an oral dose of amoxicillin-clavulanate 1g twice daily, or much less frequently, in case of intolerance or allergy, an oral dose of levofloxacin 500mg once daily, both from 1 day before to 3 days after any dental procedure.
Chlorhexidine mouthwash
Pre- and post-extraction use of chlorhexidene mouthwash has been suggested in guidelines;4,37 recommended regimens vary from twice daily use for 15 days followed by review or for as long as 2 months, depending on healing.
Alternative techniques
‘Atraumatic’ extractions using orthodontic elastics around the roots of teeth to cause slow and gradual exfoliation of teeth have been suggested by few authors, however, the practicality of this suggested technique for use in general practice is questionable and follow-up period in both studies was only nine months or less.38,39 Another author has suggested the avoidance of vasoconstrictors in local anaesthetic, however, there is limited evidence to support this.17
Drug holiday
A bisphosphonate drug holiday is currently a controversial suggestion. The Food and Drug Administration (FDA) have stated that there is no evidence for the initiation or duration of a drug holiday.17,40 Despite little evidence to support it, it has been advocated by various panels (AAOMS and CAOMS) for patients on intravenous BPs, and even for patients on oral BPs for osteoporosis with prolonged exposure and/or co-existing risk factors, based on the theoretical benefit it may have.2,41 Denosumab on the other hand has a significantly different mechanism of action and a relatively short half-life compared with that of bisphosphonates which accumulate in bone, therefore a drug holiday may be beneficial.42 The prescribing physician and the dental practitioner should consider the appropriateness of a drug holiday on an individual basis, depending on the risks and benefits of ceasing anti-resorptive therapy and the alternative or urgency of the dento-alveolar surgery.
MRONJ and periodontal disease
Presence of periodontal disease
Although the treatment for periodontal disease is not recognized as a ‘high-risk’ procedure causing obvious trauma to the supporting tissues, the presence of this chronic low-grade inflammatory disease itself has been suggested as a risk factor in the development of MRONJ.9,43 Although the mechanism in which periodontal disease may contribute to ONJ needs further research, periodontal pathogens, such as Prevotella, Porphyromonas and Fusobacterium, have been isolated in BRONJ lesions.44,45 In a large case series by Marx et al, 84% of the patients with BRONJ presented with periodontal disease (29% had advanced disease).9 Furthermore, animal studies have shown ONJ or ONJ-like lesions develop in rodents given high doses of zoledronic acid, with existing laboratory-induced periodontitis46,47 and periapical pathology.48 An association between BRONJ incidence and alveolar bone loss due to periodontal disease in patients receiving intravenous BP therapy has also been observed.49
On the contrary, other animal and human studies have shown some benefits of oral BPs on induced periodontitis models and periodontal disease, respectively.50,51,52,53,54 Many of these prospective studies were carried out early in the millennium when the concept of BRONJ was only just emerging and they are based on the expectation that osteoclastic resorption of bone in periodontal disease is reduced by BPs. Improved outcomes of non-surgical treatment or periodontal disease in patients on BPs, compared to patients on a placebo drug, in terms of significantly improved clinical attachment level (CAL), bleeding on probing53 and probing depths (PD)53,54 have been shown. Although in the absence of osteoporosis BPs would not be recommended as an adjunct to routine periodontal treatment, the latter studies suggest that positive clinical outcomes in periodontal therapy are achievable in patients on BPs; neither study described cases of ONJ. Using similar hypotheses, more recent studies have shown significantly improved PD reduction, CAL gain, and improved bone fill in chronic and aggressive periodontal disease at 6 months using a locally applied gel containing a high concentration of alendronate.55,56 The studies cannot comment on the long-term clinical, histologic and radiographic effect of the treatment.
Management of periodontal disease
The principles of management of periodontal disease remain the same in all patients whether they are taking anti-resorptives or not; preventive care, early detection, early non-surgical management with regular monitoring and maintenance. Since periodontal disease is a known risk factor for ONJ, efforts should be made to prevent the development and progression of the disease, ultimately reducing the likelihood of future infections in the tooth-supporting tissues, particularly in patients on parenteral anti-resorptives or anti-angiogenic agents. Routine non-surgical periodontal treatment is not contra-indicated in any patient group, however, procedures involving direct osseous injury, including surgical periodontal treatment, are best avoided in patients on anti-resorptive and anti-angiogenic therapy for oncology purposes.2
Teeth with severe periodontal involvement requiring extraction are often less surgically demanding owing to the reduced alveolar bone height surrounding the tooth. However, these teeth should be disregarded as a risk in patients with IV BP use. In a single centre, BRONJ was diagnosed in 9 patients, following removal of ‘hopeless’ teeth with severe periodontal involvement; all these patients had had IV bisphosphonate drug therapy.57 It is unclear whether the presence of periodontal disease or the surgical procedure was the initiating factor in this study, however, many of the reported cases of ONJ following dental extractions occur in teeth with existing periodontal or periapical pathology, suggesting the role of dento-alveolar disease in ONJ.
MRONJ and dental implants
Implants are an increasingly common treatment requiring careful surgical planning. For dental patients, costly treatment such as this carries expectations for success and longevity. Amongst other factors, the process of osseointegration of the dental implant is critical to the implant's survival. For this reason, questions arise when considering dental implants on patients who are taking medications that affect bone remodelling, ie anti-resorptives: does placing implants in patients taking anti-resorptive medications increase risk of ONJ and, furthermore, is the success rate of the implant affected? Since the placement of a dental implant is a traumatic procedure with bone removal at the osteotomy site, similarly to dento-alveolar surgery, it is contra-indicated in patients who have taken anti-resorptives for cancer by numerous expert panels.2,3,58 The incidence of ONJ associated with dental implants and anti-resorptive drugs for osteoporosis, however, remains uncertain within the literature. A summary of the papers cited in this article is shown in Table 4.
No evidence of detrimental effects
Madrid and Sanz, 200958Fugazzotto et al 200759Grant et al 200860Memon et al 201261
Negative effects
Delayed wound healing
Failure to osseointegrate
Failure post osseointegration
Wang et al 200762Yip et al 201263Yip et al 201263López-Cedrún et al 201364Shirota et al 200965Bedogni et al 201066
A systematic review of one prospective and three retrospective human studies by Madrid and Sanz concluded that there was no evidence that placement of implants in patients on oral BPs (< 4 years) was associated with ONJ in the short follow-up period.59 Some of the studies included were, however, of poor quality; one study had no control group;60 another followed patients up by questionnaires rather than clinical examination.61 The success rates of implants placed in the oral BP groups were high (95–100%), comparable to the control groups with no N-BP treatment (96.5–100%), however, the studies were unable to report on the long-term outcome of both implant success or development of ONJ. Crestal bone changes at the second stage of implant placement were compared in oral BPs users and a control group by Memon et al, with no significant differences seen between the groups.62
Case reports and case series have reported a spectrum of complications associated with implant placement in bisphosphonate patients, such as delayed wound healing at site of placement,63 failure to osseointegrate64 and subsequent failure of the implant post-osseointegration.65,66,67 Several studies have looked into possible mechanisms for failure of dental implants in patients taking BPs, concluding that BPs significantly reduce alveolar bone turnover and wound healing, thereby increasing the risk for ONJ and implant failure.68 However, only a few studies take into consideration the role of co-existing conditions, such as hypertension, corticosteroid use and smoking status. As previously discussed, the presence of infection has been indicated as a risk factor for ONJ, however, authors describing ONJ associated with dental implants do not mention peri-implant disease, a potential source of infection. A study looking at failed implants in middle-aged women found a significant odds ratio of 2.5 for a history of oral BP use.64 Failure was defined by unsuccessful osseointegration or mobility once the implant had osseointegrated. In a case series of 27 patients, ONJ presenting less than 6 months from the time of implant placement (classified as surgically related) was observed in six patients (22.2%).69 ONJ occurred in patients with oral BPs as well as IV treatment. ONJ took longer to present (mean: 68 months) following implant placement in patients on oral BPs (alendronic acid) compared to patients who had a history of IV zolendronic acid use (mean: 16.4 months), emphasizing the need for long-term follow-up for any patient on BPs. In their cohort, four patients developed ONJ even though BP use commenced after implant placement. Notably, in this group, two patients had already had implant(s) in situ for over 9 years but developed BRONJ within 4 months of commencing IV BPs; rapid progression compared to one of the other patients whose BRONJ took longer to develop (156 months) after starting oral BPs.
With limited knowledge on the long-term affects of oral BPs on dental implants, when considering treatment patients should be warned of the risks of ONJ prior to implant treatment, and cases should be selected carefully, taking into consideration other systemic and local factors. AAOMS have suggested an informed consent process should be undertaken prior to implant placement in patients on oral BPs (Table 3) owing to the long-term possibility of implant failure and low risk of developing ONJ if the anti-resorptive is continued. This advice is based on a study evaluating the effects of intravenously administered BPs on bone healing after tooth extraction and osseointegration of dental implants in a rabbit model, where the experimental group demonstrated good initial stability at 4 weeks but impaired healing around the implants at 8 weeks compared to the control.70 The conclusions we are able to draw from this study are limited.
Interestingly, studies involving local application of BP to implant surfaces have been carried out with positive results in animal71,72,73 and human74 models without causing ONJ. The local delivery of the anti-resorptive agents have shown improved early fixation, increased bone density, both close to and further away from the screw.75 The long-term clinical outcome of BP coatings on dental implants is an area of future research.
Conclusion
Medication-related ONJ is a complex, multi-factorial process. The key to the management of patients at risk for ONJ in primary care involves taking a thorough medical history and understanding the indications and nature of any anti-resorptive or anti-angiogenic therapy, which will subsequently determine their dental management. Cancer patients are at a higher risk of ONJ than patients with osteoporosis and should be managed with caution, however, oral health screening and preventive care would benefit any patient receiving these agents. Dentists should familiarize themselves with the names and indications of newer agents associated with ONJ to help identify those patients at higher risk for the disease. Dental extractions and periodontal disease have been identified as risk factors for ONJ, especially in high risk patients, and the long-term success rates of implants in oral BP users is yet to be determined, as does the long-term outcomes of locally applied BPs in animal and human models.