Korenromp EL, Bierrenbach AL, Williams BG, Dye C. The measurement and estimation of tuberculosis mortality. Int J Tuberc Lung Dis. 2009; 13:(3)283-303
Amin Z. Clinical tuberculosis problems and management. Acta Med Indones. 2006; 38:(2)109-116
United States: Centers for Disease Control and Prevention (CDC); 2008
Menon K, Bem C, Gouldesbrough D, Strachan DR. A clinical review of 128 cases of head and neck tuberculosis presenting over a 10-year period in Bradford, UK. J Laryngol Otol. 2007; 121:362-368
Tovaru S, Costache M, Sardella A. Primary oral tuberculosis: a case series from Bucharest, Romania. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 105:(5)41-45
Erbaycu AE, Taymaz Z, Tuksavul F, Afrashi A, Güçlü SZ. What happens when oral tuberculosis is not treated?. Monaldi Arch Chest Dis. 2007; 67:(2)116-118
Taegtmeyer M, Beeching NJ, Scott J, Seddon K, Jamieson S, Squire SB, Mwandumba HC, Miller ARO, Davies PDO, Parry CM. The clinical impact of nucleic acid amplification tests on the diagnosis and management of tuberculosis in a British hospital. Thorax. 2008; 63:317-321
Franken WPJ, Timmermans JF, Prins C, Slootman EHJ, Dreverman J, Bruins H, T van Dissel J, Arend SM. Comparison of Mantoux and QuantiFERON TB Gold Tests for diagnosis of latent tuberculosis infection in army personnel. Clin Vacc Immunol. 2007; 477-480
National Institute for Health and Clinical Excellence [Tuberculosis] [CG117].London: National Institute for Health and Clinical Excellence; 2011
An unusual extranodal presentation of mycobacterium tuberculosis in the upper lip Rachel B Taute Jennifer Wylie Lachlan Carter Dental Update 2024 42:5, 707-709.
Authors
Rachel BTaute
MBChB, BChD, MFDS RCS(Ed)
Clinical Fellow, Oral and Maxillofacial Surgery, Leeds Dental Institute, Leeds Dental Institute, Clarendon Way, Leeds LS2 9LU, UK
Tuberculosis (TB) is a leading cause of morbidity and mortality worldwide, with a peak incidence in South-East Asia and Sub-Saharan Africa. A significant number of patients in the UK are affected. Extra-pulmonary TB presentation varies, and includes head and neck manifestations that can present on routine examination in the dental practice setting. We report an unusual case of extra-nodal TB in the upper lip, and provide some guidance to general dental practitioners on the presenting features of such lesions, and what to refer for further investigation where TB is included in the differential diagnosis.
CPD/Clinical Relevance: This case report highlights important factors in TB diagnosis, with particular emphasis on presenting features relevant to general dental practitioners, and informs on the accepted and current treatment regimen.
Article
Tuberculosis (TB) ranks among the ten principal causes of death and disability worldwide.1 According to the World Health Organization, one-third of the world's population has been infected. Approximately eight million people contract the disease annually, and two to three million deaths occur every year due to TB.2 In the United Kingdom, it is a notifiable disease.
TB disproportionately affects poor people, mostly in the developing world where HIV infection increases the likelihood of contracting the disease. In developed countries, the rates of TB have fallen over the past 80 years, mainly due to the development of effective treatments, active case findings and the BCG vaccine. Recently, however, there has been a slowing decline in TB incidence,3 particularly visible in high-risk groups, such as immigrants, patients with HIV infection, those with poor general health, and patients living in areas of social disruption.
The disease can be broadly classified as pulmonary TB or extrapulmonary TB, the most common form found in the head and neck being lymph node TB.4 Other reported sites in the head and neck include the submandibular salivary glands, larynx, eyes, ears, skin, oral cavity, retropharynx, parotid gland, thyroid and nasopharynx.
TB of the oral cavity is rare.5 Blood or lymphatic spread of the infection to extra-pulmonary sites may occur, and coughed sputum from the lungs may result in extra-pulmonary deposition of the bacteria. The oral lesions may present in a variety of forms, such as persistent ulcers or granulomatous masses.6 We report an unusual case of extra-nodal TB in the upper lip.
Case report
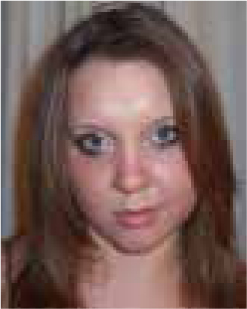
A 24-year-old Pakistani female presented to the Leeds General Infirmary Accident and Emergency Department complaining of a four-week history of an increasing, painful swelling in the upper lip. She was referred in urgently by her general medical practitioner, having seen her twice over the previous five days. She had been treated with co-amoxiclav, but the swelling continued to increase in size, and was now becoming painful. She was fit and healthy with no significant medical history. She was a non-smoker and did not consume alcohol. There was no history of overseas travel within the previous 12 months.
On examination, there was a 2 cm x 1 cm fluctuant swelling in the upper lip (Figure 1). Small, mobile, smooth, non-tender cervical lymph nodes were palpable bilaterally. There was no obvious dental cause, and no similar lesions elsewhere. The patient was apyrexial with no systemic complaints.
Figure 1. Mycobacterium tuberculosis in the upper lip.
Blood tests were unremarkable except for a raised CRP of 25 mg/L.
An ultrasound scan of the upper lip and surrounding tissues confirmed a 15 x 10 x 10 mm lesion, cystic in appearance and suggestive of a small abscess collection.
The lesion was aspirated and approximately 4 ml of pus were sent for microscopy, culture and sensitivity (MC&S). Microscopy detected polymorphs. The culture had no growth after 3 days' incubation. The patient was sent home with one weeks' course of oral flucloxacillin 500 mg QDS and amoxicillin 500 mg TDS, and an outpatient review appointment was arranged.
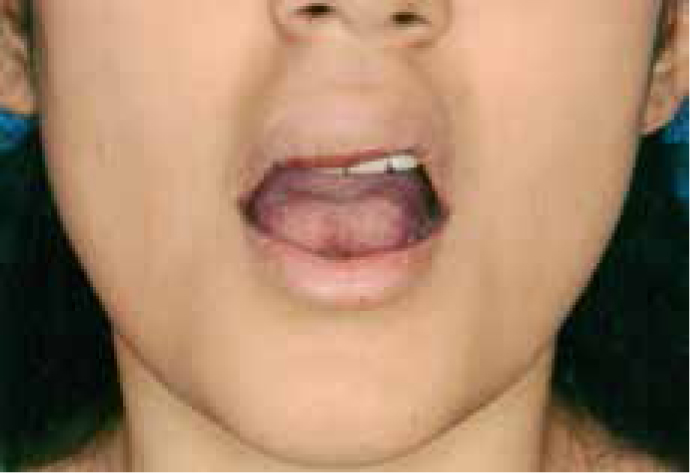
When the patient returned a week later, the swelling had grown to 2.5 cm x 2cm and was pointing intra-orally. The patient was complaining of malaise, night sweats and fever. She was therefore admitted acutely for an incision and drainage of the lip lesion. The differential diagnosis at this point included infection, possibly atypical mycobacteria, TB and malignancy.
At operation, the mass was necrotic and contained pus, and was therefore fully excised (Figure 2). A pus sample was sent for MC&S and tissue samples sent to Microbiology and Histopathology. A chest x-ray taken during admission showed nothing of note. Following this, the lip wound healed uneventfully and the patient's symptoms improved.
Figure 2. The mass removed was necrotic and contained pus.
The Histopathology report described fibrocollagenous tissue diffusely infiltrated by chronic inflammatory cells with areas of hyalinization and tissue necrosis. There was no evidence of malignancy. Ziehl-Neelsen stains for atypical bacteria were negative. Acid-fast bacilli (AFB) were not seen on microscopy of the pus sample, but some four weeks later, mycobacterium tuberculosis was isolated.
The patient was referred to the Infectious Diseases department, and a sputum sample taken. Again AFBs were not seen, but mycobacterium tuberculosis was isolated after two weeks' incubation. Standard tuberculosis therapy (ethambutol, pyridoxine, and rifater) was started and continued for nine months.
Discussion
The case described highlights the importance of considering TB (especially in high-risk patients) as an early differential diagnosis, particularly where oral lesions present without common clinical findings, such as pyrexia, altered haematology and biochemistry, radiological and microbiological findings, and an obvious source of infection. In this case, the lesion presented as a painful swelling, but in previous literature painless swellings, lymph nodes and ulcers have also been described. Early inclusion in the differential diagnosis allows appropriate use of the diagnostic tools available for TB identification.
Staining for AFBs can be a helpful and speedy method of narrowing the differential diagnosis but is not specific for mycobacterium tuberculosis alone. Culture or polymerase chain reaction (PCR) allow a definitive diagnosis of TB to be made.
Diagnosis for this case was made primarily from the pus and tissue samples taken in theatre which, although conclusive, led to a delay in commencing treatment.
Nucleic acid amplification tests (NAAT) based on PCR provide rapid identification of mycobacterium tuberculosis7 and are particularly useful when histology or bacteriology are inconclusive,4 however, this is not yet widely available. Quantiferon TB gold tests may also be used to isolate TB-specific antigens ESAT-6, CFP-10 and TB7.78 and can be of use in latent TB following a positive tuberculin skin test for screening purposes.
The National Institute for Health and Clinical Excellence9 advises on diagnosis and management of TB in certain clinical scenarios. Biopsy is indicated in those with suspected active extrapulmonary TB where the benefit outweighs the operational risk. Treatment should commence if the clinical and histological findings are consistent with TB, without waiting for culture results. In our case, we were unable to commence treatment until culture results were confirmative for mycobacterium tuberculosis, as histological findings did not suggest TB.
Concerns for the general dental practitioner
Owing to the infrequent presentation of TB lesions in the oral cavity, lack of familiarity may lead to missed or delayed diagnosis. A routine dental check-up includes palpation for lymph nodes and examination of any intra-oral and peri-oral lesions.
On finding such a lesion, a thorough history must be taken. Medical, social and travel history may provide the practitioner with vital clues in provisionally diagnosing extra-pulmonary TB. In addition to the history, it is worth bearing in mind both the differential diagnoses for lip lesions (Table 1), and the variable clinical presentation of TB: a variety of lesions are seen (Table 2), sometimes in the presence of pain, and sometimes with systemic disturbance, but we have seen that this is not always the case. A high index of suspicion and knowledge of TB diagnostic procedures are essential to enable practitioners to make an early referral and for rapid confirmation of diagnosis, allowing timely treatment.
It is also worth noting special cross-infection control issues when treating patients with suspected or known TB, which is only communicable when cavitating pulmonary TB is present, and is spread through infected airborne aerosol droplets.
Routine dental treatment should be delayed until the patient is healthy but, where emergency treatment for pain is required, it should be carried out at the end of the day, with minimal staff involvement. Patients can be asked to wear a mask in communal areas and staff involved in treatment should wear high efficiency particulate air (HEPA) filtering masks, clinical gowns and full coverage visors. The use of dental drills and ultrasonic scalers should be avoided owing to aerosol formation. High volume suction should be used throughout any procedure undertaken, and the clinical area disinfected routinely following the appointment. In those patients with resistant TB, an opinion should be sought from the local Infection Control Team regarding appropriate management.