Pace-Balzan A, Shaw RJ, Butterworth C Oral rehabilitation following treatment for oral cancer. Periodontology 2000. 2011; 57:102-117
Keyf F Obturator prostheses for hemimaxillectomy patients. J Oral Rehabil. 2001; 28:821-829
Alani A, Owens J, Dewan K, Summerwill A A national survey of oral and maxillofacial surgeons' attitudes towards the treatment and dental rehabilitation of oral cancer patients. Br Dent J. 2009; 207:540-541
Rogers SN, Lowe D, McNally D, Brown JS, Vaughan ED Health-related quality of life after maxillectomy: a comparison between prosthetic obturation and free flap. J Oral Maxillofac Surg. 2003; 61:174-181
Worthington HV, Clarkson JE, Eden OB Interventions for preventing oral mucositis for patients with cancer receiving treatment. Cochrane Database Syst Revs. 2006; CD000978-CD000978
Marx RE A new concept in the treatment of osteoradionecrosis. J Oral Maxillofac Surg. 1983; 41:351-357
Lyons A, Ghazali N Osteoradionecrosis of the jaws: current understanding of its pathophysiology and treatment. Br J Oral Maxillofac Surg. 2008; 46:653-660
Delanian S, Lefaix JL The radiation-induced fibroatrophic process: therapeutic perspective via the antioxidant pathway. Radiother Oncol. 2004; 73:119-131
Harris M The conservative management of osteoradionecrosis of the mandible with ultrasound therapy. Br J Oral Maxillofac Surg. 1992; 30:313-318
Schwartz HC, Kagan AR Osteoradionecrosis of the mandible – scientific basis for clinical staging. Am J Clin Oncol-Cancer Clin Trials. 2002; 25:168-171
Nabil S, Samman N Incidence and prevention of osteoradionecrosis after dental extraction in irradiated patients: a systematic review. Int J Oral Maxillofac Surg. 2011; 40:229-243
Reuther T, Schuster T, Mende U, Kubler A Osteoradionecrosis of the jaws as a side effect of radiotherapy of head and neck tumour patients – a report of a thirty year retrospective review. Int J Oral Maxillofac Surg. 2003; 32:289-295
Koga DH, Salvajoli JV, Alves FA Dental extractions and radiotherapy in head and neck oncology: review of the literature. Oral Dis. 2008; 14:40-44
Kayser AF Shortened dental arches and oral function. J Oral Rehabil. 1981; 8:457-462
Siddall KZ, Rogers SN, Butterworth CJ The prosthodontic pathway of the oral cancer patient. Dent Update. 2012; 39:98-106
Marx RE, Johnson RP Studies in the radiobiology of osteoradionecrosis and their clinical significance. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1987; 64:379-390
Clayman L Management of dental extractions in irradiated jaws: a protocol without hyperbaric oxygen therapy. J Oral Maxillofac Surg. 1997; 55:275-281
Kielbassa AM, Hinkelbein W, Hellwig E, Meyer-Luckel H Radiation-related damage to dentition. Lancet Oncology. 2006; 7:326-335
Walter J Obturators for acquired palatal defects. Dent Update. 2005; 32:277-284
Beumer III, Curtis TA, Marunick MTSt Louis, Toronto, London: The CV Mosby Co; 1979
Zarb GA The maxillary resection and its prosthetic replacement. J Prosthet Dent. 1967; 18
Aramany MA Basic principles of obturator design for partially edentulous patients. Part I: Classification. J Prosthet Dent. 1978; 40:554-557
Parr GR, Tharp GE, Rahn AO Prosthodontic principles in the framework design of maxillary obturator prostheses. J Prosthet Dent. 2005; 93:405-411
Kornblith AB, Zlotolow IM, Gooen J, Huryn JM, Lerner T, Strong EW Quality of life of maxillectomy patients using an obturator prosthesis. Head Neck-Journal Sci Special Head Neck. 1996; 18:323-334
Okay DJ, Genden E, Buchbinder D, Urken M Prosthodontic guidelines for surgical reconstruction of the maxilla: a classification system of defects. J Prosthet Dent. 2001; 86:352-363
Beumer J, Zlotolow I, Curtis TA, 3rd edn. Atlanta: American Cancer Society; 1990
Werning JWNew York: Thieme Medical Publishers Inc; 2007
List MA, Stracks J, Colangelo L, Butler P, Ganzenko N, Lundy D How do head and neck cancer patients prioritize treatment outcomes before initiating treatment?. J Clin Oncol. 2000; 18:877-884
Shah JP Dental oncology and maxillofacial prosthetics. In: Zlotolow IM Hamilton, Ontario, Canada: BC Decker Inc; 2001
Rehabilitation of oncology patients with hard palate defects part 1: the surgical planning phase Rahat Ali Asmaa Altaie Brian Nattress Dental Update 2024 42:4, 707-709.
This article is the first in a series of three papers that will discuss the conventional non-implant retained prosthodontic rehabilitation of oncology patients with surgically acquired hard palate defects. In this first paper, the dental challenges posed by the oncology patients will briefly be discussed. The interface between the specialist restorative dentist and the maxillofacial surgeon when planning the conventional dental rehabilitation of an oncology patient with a hard palate defect will be discussed in detail.
Clinical Relevance: To highlight the importance of the restorative dentistry/surgical interface when planning a treatment for a patient requiring a maxillectomy and conventional obturation.
Article
Maxillary hard palate defects can be congenital or acquired in nature. Acquired palatal defects can be created by the surgical treatment of benign or malignant tumours. Although head and neck cancers are relatively rare in the UK (with 8000 new cases being reported per year),1 patients who present with such malignancy require careful planning and treatment. If the tumour is managed surgically, this treatment can have major effects on the physical, psychological and social wellbeing of these patients.2 Removal of the palate by ablative surgery creates a significant anatomical defect that allows the oral cavity, maxillary sinus, nasal cavity and nasopharnyx to become one confluent chamber. This has a significant impact on patients in terms of their ability to speak, swallow and chew. Food and liquids will pass from the oral cavity into the nasal cavity, making adequate feeding very difficult. Air escape from the oral cavity into the nasal passages can also create an unnatural hypernasal speech pattern.3 Furthermore, the presence of the defect can constantly (and adversely) remind patients of their experience with cancer. Management of the resected site can be by surgical reconstruction or prosthetic rehabilitation with an obturator.
Palatal defects: surgical reconstruction or prosthetic obturation?
The number of individuals undertaking surgical reconstructions has increased from 38% to 91% from 1995 to 2009,4 with the use of microvascular free flaps becoming more common. Surgically reconstructing a defect will mean that patients will not be dependent on an obturator for feeding and speech. However, reconstructed sites frequently have significantly altered anatomy and may require rehabilitation with implant-supported superstructures for optimal stability, retention and support. Alani et al have also reported a concurrent increase in the use of dental implants to rehabilitate head and neck oncology patients from 43% to 93%, between 1995 and 2009.4 This increase is probably due to more training for restorative dentists/maxillofacial surgeons in implantology, as well as necessity, as it may not be possible to provide an optimally stable prosthesis in a surgically reconstructed site without using dental implants. However, arguments in favour of prosthetically obturating a maxillary defect include the provision of an immediate set of teeth, the ability to restore cheek support with the prosthesis and the ability to gain support/retention from within the resected site. One could argue that the ability to remove the prosthesis will allow the surgeon to inspect the surgical site for re-occurrence of the tumour. However, with the accuracy and clarity of modern imaging technologies (such as MRI and CT scanning), this should not be the sole reason for prosthetic obturation over reconstruction. Rogers et al have failed to find any statistically significant differences in terms of recreation, physical functioning and quality of life issues between maxillectomy patients reconstructed with free flaps and those receiving prosthetic obturation.5 Although the obturator group appeared to be less satisfied with function, their appearance and having more problems with oral pain/soreness, the differences between this group and the reconstruction group did not reach statistical significance. A failure to find such a difference may be due to the relatively small sample size in this study, and reflects the need for further and larger studies to evaluate fully whether actual quality of life differences exist between surgically reconstructed and prosthetically obturated oncology patients, a conclusion echoed by the authors.5
Choosing the appropriate treatment modality depends on a number of factors and all head and neck cancer patients should be discussed by a formal multidisciplinary team (MDT)1 to maximize the chances of an optimal outcome for each individual patient.
Ideally all patients should be surgically reconstructed. However this may not be appropriate for all patients (such as those with significant medical co-morbidities or those lacking suitable donor sites). For these patients, prosthetic obturation may be more appropriate. The use of dental implants in the residual alveolus or zygomatic implants can significantly improve the retention of a maxillary obturator. However, for certain patients (who are still growing, unwilling to have more surgery or are medically compromised), the provision of implants to support an obturator is more complicated and may not be appropriate. The construction of a satisfactory obturator can be a daunting task for clinicians who are new to maxillofacial prosthetics. With this in mind, this series of three papers discusses the non-implant retained prosthodontic rehabilitation of oncology patients with hard palate defects. It is hoped that clinicians who are treating their first oncology patients and rehabilitating them with an obturator find this series useful. In the first paper, the dental challenges posed by the oncology patient will briefly be discussed. The interface between the specialist restorative dentist and the maxillofacial surgeon when planning the conventional dental rehabilitation of an oncology patient with a hard palate defect will be discussed in detail. The second paper will discuss the principles of basic obturator design and the third paper, the clinical stages involved in the fabrication of an acrylic resin, one part, hollow bulb obturator for a patient with a hard palate defect.
Dental challenges posed by the oncology patient
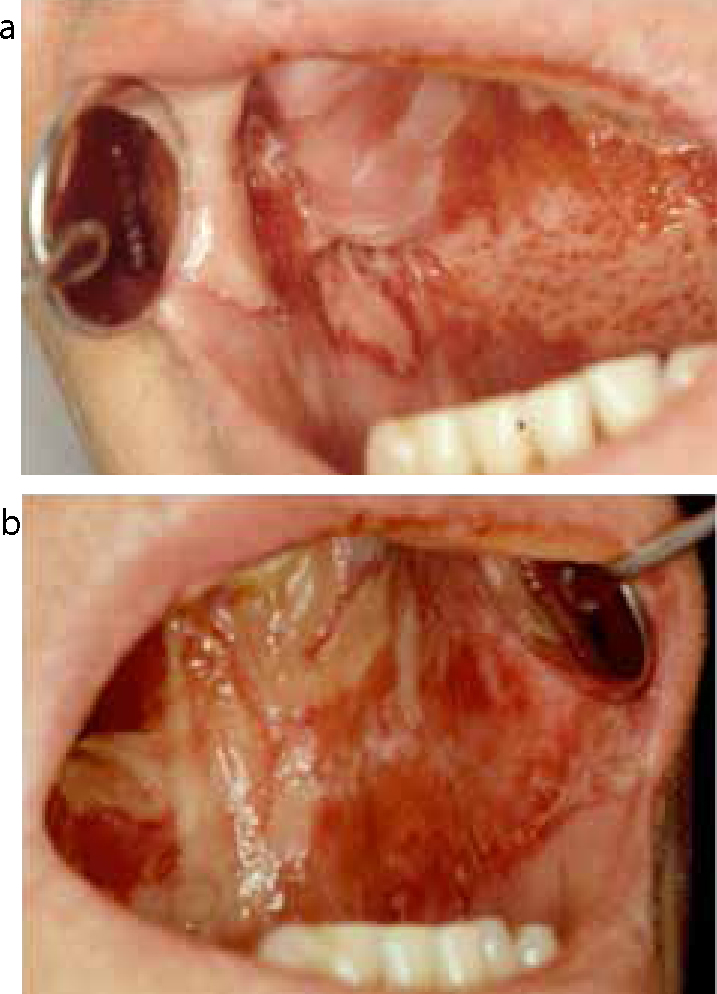
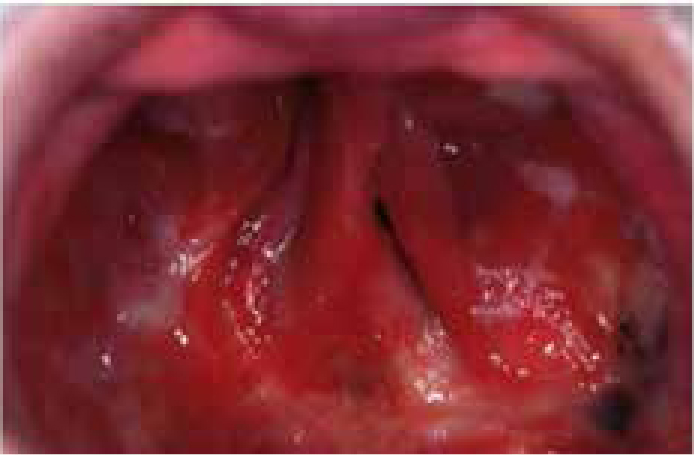
A combination of surgery and post-operative radiotherapy may be used to manage some head and neck oncology patients. The side-effects of radiotherapy to the head and neck region cannot be underestimated and include xerostomia, cervical caries (exacerbated by the high calorific intake of refined sugars which the patient may be asked to consume to maintain their weight), increased plaque levels (due to the decreased salivary flow), candidal infections, taste alteration (dysgeusia/hypogeusia) and dysphagia. Furthermore, radiation to the oral mucosa can cause mucositis which can manifest in a variety of forms ranging from erythema to severe ulceration. Symptoms of mucositis vary from pain/discomfort to an inability to tolerate food or fluids. This can create a hostile oral environment which can debilitate the patient and pose a challenging setting for the dentist to manage (Figure 1). Worthington et al's Cochrane Review identified numerous interventions to prevent the mucositis seen in oral cancer patients.6 A number of them, including benzydamine, ice chips and zinc sulphate may reduce the severity of mucositis. However, the strength of the studies was variable and the general reporting of the studies (especially randomization) was poor.
Figure 1.
(a, b) A patient with severe radiation-induced mucositis of the oral cavity.
Trismus may also be seen in head and neck oncology patients. It may develop due to tumour invasion of the muscles of mastication or due to muscle fibrosis caused by radiotherapy. The limited mouth opening can make it exceptionally difficult to provide all aspects of future dental treatment.
The most serious sequelae of radiotherapy to the head and neck region is osteroradionecrosis (ORN). Marx suggested that radiation therapy may cause the formation of hypoxic/hypocellular/hypovascular tissue.7 Breakdown of the tissue may lead to a chronic non-healing wound (driven by the persistent hypoxia) in an area of irradiated bone.8 However, the more recent radiation-induced fibrosis theory9 suggests that radiation therapy causes an abnormal population of fibroblasts to form. During the late fibro-atrophic phase, tissue remodelling results in the formation of very fragile healed tissues which have the potential to become persistently inflamed if injured.8 Once the tissue is traumatized, ORN can develop.
ORN has been defined as an area of irradiated bone that becomes exposed through the overlying skin/mucosa and fails to heal after a period of 3 months.10 Once established, it is extremely difficult to manage.8 ORN is more common in the mandible than the maxilla, and tends to be seen when a radiation dose of more than 60 Gy has been administered.11 Nabil and Samman's systematic review suggested that extraction of teeth post 60 Gy irradation of the mandible constituted a high risk factor for ORN,12 a finding also echoed by Reuther et al.13 To reduce the chances of ORN developing, it is imperative that any necessary dental extractions are carried out before radiotherapy is started.
Pre-radiotherapy assessment
Before a head and neck oncology patient is due to start radiotherapy, it is important that he/she is dentally screened to identify any potential sources of odontogenic infection.14 The patient should be carefully examined both clinically and radiographically. Teeth in the radiation field must be carefully scrutinized. Any simple restorations and non-surgical periodontal therapy should be carried out as soon as possible. Any unrestorable teeth, teeth affected by advanced bone loss, severe periodontal disease or partially erupted teeth should be extracted before radiotherapy is started.15 Such teeth may require extraction in the future and are therefore potential sites where ORN could develop. Given how serious and difficult it is to manage ORN, the authors suggest that a more aggressive approach is utilized when screening patients pre-radiotherapy. Any non-vital teeth, teeth with sub-standard root fillings or any tooth which has a guarded long-term prognosis and is in the radiotherapy field should also be considered for extraction. Clinicians should consider leaving patients with a shortened dental arch16 pre-radiotherapy, if the posterior jaw is to be irradiated and all the posterior teeth have a poor long-term prognosis. The remaining anterior teeth will be easier for the patients to maintain and will be more accessible for clinicians should they need treatment.17 If posterior teeth remain and develop dental disease in the future, the degree of trismus may simply not allow clinicians to access the teeth to carry out remedial treatment.2
Marx and Johnson have suggested that there is a direct link between the incidence of ORN and the time allowed for healing (post extraction) before the start of radiotherapy.18 ORN did not develop when the oral tissues were allowed to heal for 3 weeks or more. Therefore teeth of guarded prognosis should preferably be extracted 3 weeks pre-radiotherapy. Ten days pre-radiotherapy is acceptable but should be considered an absolute minimum period.19
Dentate patients post radiotherapy are at significant risk from caries as a result of damage to the salivary glands (the resultant xerostomia) and possible direct damage to the dentition by the radiation.20 The need to maintain body weight and nutrition may require the patient to use highly calorific (yet cariogenic) food supplements such as Fortisips. This will only compound the problem of dental caries. The dental team should work with the dieticians to keep the length of time for their use to a minimum. Patients should be advised to rinse their mouths after each intake or to use sugar-free alternatives. They should use GC Tooth Mousse to provide a topical supply of calcium and phosphate in addition to brushing with 5,000 ppm fluoride toothpaste twice a day14 to promote remineralization of any early carious lesions. Fluoride gel trays should be provided for dentate patients post radiotherapy, which they can load with 5000 ppm fluoride toothpaste and wear on a daily basis. For patients with xerostomia, a number of recommendations have been made to keep the mucosa lubricated, including taking frequent sips of water and saliva replacement products such as Biotene. Patients should see their own dentist regularly for check-ups and professional scaling/oral hygiene advice as they are at high risk from dental disease. If the aforementioned measures are taken, the chances of the patient developing caries should be minimized.
Combined restorative/surgical planning for the oncology patient
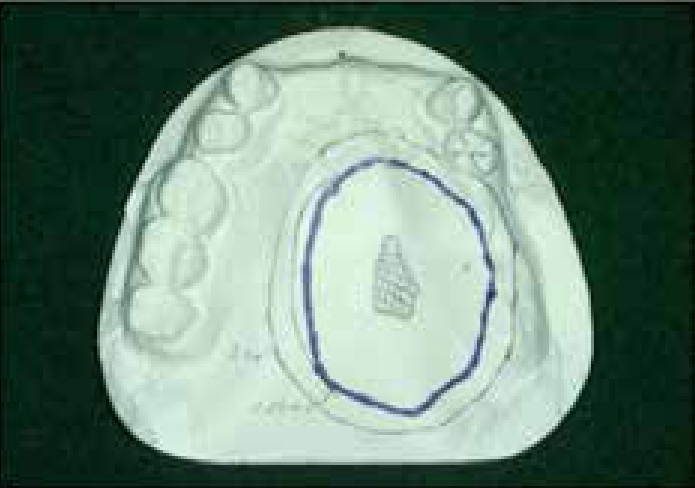
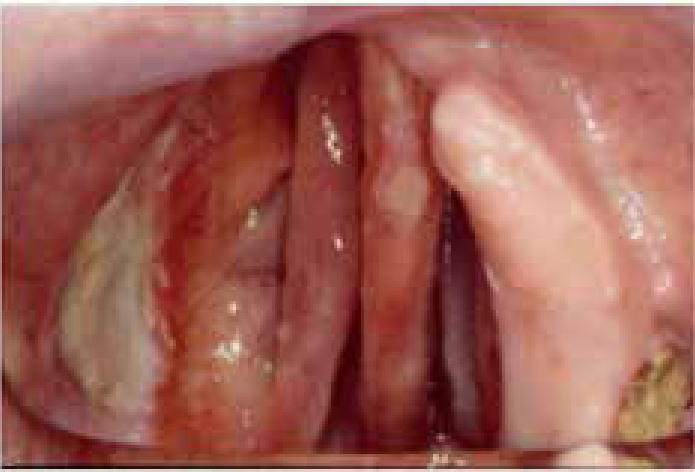
The dental journey of the head and neck oncology patient begins with the pre-radiotherapy assessment. If a resection (without primary closure or reconstruction) is being planned, it is essential that good quality pre-operative study casts are obtained. The clinician should discuss the dimensions of the proposed resection site with the surgical team and then mark this on the pre-operative models (Figures 2 and 3).
Figure 2. Pre-operative study model with the proposed surgical site marked out by the surgeon.Figure 3. Post-operative view of the same patient shown in Figure 2. Notice how the resulting resection site closely mirrored the proposed surgical site marked out on the preliminary study cast.
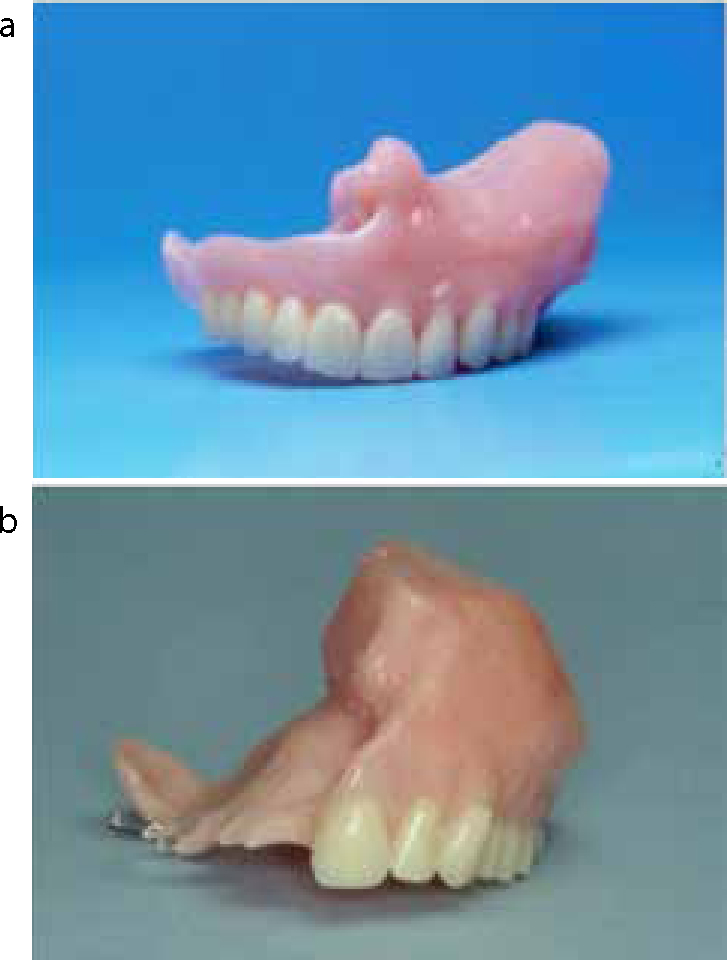
The technician should then remove the tumour (and any teeth associated with it) from the cast as per the surgical team's plan. The baseplate made on the altered cast will form the foundation of the surgical obturator. The plate should have wire ‘goal posts’ positioned over the proposed resection site. The wire ‘goal posts’ will unite the surgical bung with the baseplate at the time of prosthetic obturation (Figures 4a, b, c). At the time of resection, the acrylic ‘goal posts’ can be modified with impression compound or a silicone putty bung so that it is well adapted to the surgical site, ensuring that it is not overbuilt in the vertical plane. Silicone putty is easy to manipulate and dimensionally stable. However, it cannot be reshaped once it has set. Impression compound is more difficult to manipulate. However, it can be reheated and readapted to the surgical site if the first attempt to produce a bung proves unsatisfactory (Figures 4d, e). Once adapted to the resection site, the surgical obturator can be secured to the patient's palate with titanium screws, clasps engaging the remaining teeth (Figures 4b–e) or historically transnasal and zygomatic wires.21
Figure 4.
(a) Pre-operative study model showing the tumour. (b) The altered primary cast to simulate the proposed resection. (c) The baseplate with wire ‘goal posts’ for a surgical obturator made from the cast in (a). (d, e) The surgical obturator from (b, c). Impression compound was used to develop the bung. Anterior teeth have been added on for aesthetic reasons. (f) A surgical obturator for a patient with a right-sided maxillary resection. His existing denture was duplicated and had wire ‘goal posts’ added to it near the resection site. The bung was developed with impression compound before being screwed into place. (g) The surgical obturator in (d, e) being duplicated in laboratory putty.
If the patient is satisfactorily wearing a complete maxillary denture, it can be duplicated and used as the foundation for the surgical obturator (Figure 4f).
The surgical obturator will help to minimize the psychological trauma of surgery by restoring normal palatal contour and allowing the patient to swallow and speak. It can be used to retain a surgical pack and reminds the patient that dental rehabilitation has already begun.3 The surgical obturator can be made of clear acrylic resin so that its extensions can be visualized more easily at surgery.3 However, this is a matter of personal preference as pink acrylic is equally acceptable (Figure 4f). It should terminate short of the skin graft/mucosal junction, should be lightweight and can have anterior teeth added to it for aesthetic reasons. No form of posterior occlusal contact should be developed on the resection side until the wound has healed22 (Figure 4d, e).
After 7–10 days, the surgical obturator can be removed.22 Impressions can then be taken for the interim obturator to be made. Given that the restorative dentist will already have a preliminary cast, a special tray can be prepared on the modified cast and used to take the master impression for the interim obturator. Impression techniques and the clinical stages for making an obturator will be discussed in Part 3 of this series.
If the patient is wearing a complete denture as part of his/her surgical obturator, consideration can be given to duplicating it and using it to make the interim obturator using the copy denture technique (Figure 4g). Utilizing this technique will clearly require less adaptation on the part of the patient if he/she is happy with the complete denture.
Once this has been fitted, the patient should be reviewed regularly every 2–4 weeks as rapid soft tissue changes will occur during the first 6–12 months post resection.23 The interim obturator may need significant modification, which may include modifying the bung with Viscogel (Densply Caulk, Germany), Coe-Comfort (GC America INC, USA), UFI Gel (VOCO, Germany) or self-cured acrylic resin (Tokuyama Dental, Japan) to improve its fit around the resection site. The patient should be advised to wear the obturator all the time and remove it only for cleaning. The restorative dentist has been listed as one of the core members who should be present when a multidisciplinary team convenes to discuss the management of a head and neck oncology patient. If tumour resection (without reconstruction) is being planned, it is imperative that the restorative dentist examines the patient and takes pre-operative study casts. These models are invaluable and can be used by the restorative dentist and maxillofacial surgeon for planning purposes such that an optimal denture-bearing area remains post resection.
A number of surgical procedures can be used to optimize retention and support for the future obturator. These include preservation of the anterior teeth (both ipsilateral and contralateral) to the defect, if it does not compromise tumour resection.24 Such teeth can be used for both direct and indirect retention when an obturator is provided (Figure 5).
Figure 5. Example of a resection patient where retention of teeth both ipsilateral and contralateral to the surgical site was planned to aid retention of any future prosthesis.
The placement of a split thickness skin graft along the posterolateral and lateral margins of the defect has also been suggested (Figure 6). The skin graft will not be easily abraded, will not secrete mucus and may aid retention of a prosthesis by forming a lateral scar band (and therefore an undercut). This scar band will flex on insertion of the prosthesis and resist its displacement25 (Figure 7). Preservation of as much of the hard and soft palate in addition to the tuberosity on the side of the defect can significantly improve the support and retentive capacity of a future obturator (Figure 8). Indeed, it was reported that the quality and function of an obturator was considerably less when more than one quarter of the hard palate and one third of the soft palate had been resected.26 Such patients reported more problems with oral/nasal leakage, speech, swallowing and feeding. The prognosis of an obturator made when the contralateral teeth, maximal palatal tissue and the tuberosities have been preserved will clearly be higher than an appliance constructed on a reduced denture-support area (Figure 9).
Figure 6. Placement of a split thickness graft along the lateral margin of the defect will form a scar band and undercut to help retain the bung of an obturator.Figure 7.
(a) Placement of a split thickness graft along the lateral margin of the defect formed an undercut that helped to retain the obturator. The undercut has been engaged by the bung provided in the obturator. (b) A split thickness graft was not placed along the lateral margin of the defect. No lateral undercut was available for any future prosthesis. The bung of the obturator was found to be unretentive clinically.Figure 8. Post-surgical resection site where it was possible to preserve the tuberosity and therefore improve the retention of an obturator. Notice how reasonable amounts of hard palate have also been preserved which will help to support a future prosthesis.Figure 9. A patient where the entire hard and soft palate was resected. The prognosis for any conventionally made prosthesis will be guarded.
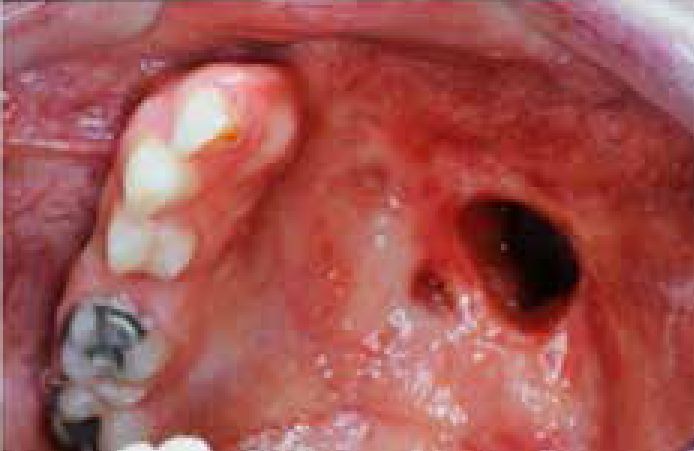
The surgeon should be encouraged to place an osteotomy cut through an extraction site adjacent to the defect. This crucial step will preserve the alveolus of the abutment tooth and therefore improves its ability to support a prosthesis27 (Figure 10). Another surgical modification is the removal of the coronoid process to prevent displacement of the obturator and to reduce trismus. As the mandible moves downward and forward the coronoid may displace the distolateral aspect of the obturator, resulting in irritation to the mucosa.28 To prevent this, it is advisable to remove the coronoid process (especially when the resection extends posterior to the soft palate).
Figure 10. A patient where most of the alveolus on the left-hand side had been resected. Notice how the osteotomy cut has been positioned to preserve the mesial alveolus of the UR2.
Others have advocated that the patient's turbinates should be shaved back to improve air flow and allow at least a 10 mm high bung to engage the defect. This will allow the bung to engage a reasonable height within the defect, without touching the relatively sensitive nasal turbinates.29
Given the complex surgical/restorative considerations, it is clear that active discussion and careful planning is required between the restorative dentist and maxillofacial surgeon if an optimal denture support area is to be achieved post treatment.
Discussion
Oral cancer patients pass through an exceptionally difficult journey. It begins with the diagnosis of oral cancer, followed by complex treatment stages. This has a major lifelong impact on the patient's psychological, physical and social well-being. Survival is the primary concern of the affected individuals at the stage of diagnosis.30 However, following treatment, patients' concerns shift towards improvement and maintenance of their quality of life and this includes their dental well-being. Rehabilitation of a maxillary defect requires precise evaluation and planning by a multidisciplinary team. Oncology patients have several dental challenges which make treatment more difficult for the dentist and collaboration between restorative dentists and maxillofacial surgeons (from an early stage) is extremely important to optimize treatment outcomes. Restorative dentists are critical members of the multidisciplinary team. Their recommendations to the maxillofacial surgeons to preserve tissues (or improve the existing anatomical structures) is most important and can significantly affect the retention, stability and support of an obturator.31 The restorative dentist is charged with ensuring that the patient is dentally fit before surgery/chemoradiotherapy begins, as well as producing good quality surgical, interim and definitive obturators. The authors feel that carrying out a pre-radiotherapy dental assessment and construction of an obturator is not an easy task. Clinicians who wish to carry out these duties need suitable training, practice and experience if they are to provide optimal care for their patients.
The next article in this series will describe the basic principles of obturator design which need to be appreciated when prosthetically rehabilitating a patient with a hard palate defect.