Ethunandan M, Tran AL, Anand R, Bowden J, Seal MT, Brennan PA. Needle breakage following inferior alveolar nerve block: implications and management. Br Dent J. 2007; 202:395-397
Bedrock RD, Skigen A, Dolwick MF. Retrieval of a broken needle in the pterygomandibular space. J Am Dent Assoc. 1999; 130:685-687
Blum T. Further observations with hypodermic needles broken during the administration of oral local anesthesia: a report of sixtyfive cases. Dent Cosmos. 1924; 66
Robinson PD, Pitt Ford TR, McDonald F.Oxford: Wright; 2000
Thompson M, Wright S, Cheng LHH, Starr D. Locating broken dental needles. Int J Oral Maxillofac Surg. 2003; 32:622-624
, 8th edn. Oxford: Elsevier; 2009
Callegari L Ultrasound-guided removal of foreign bodies: personal experience. Eur Radiol. 2009; 19:(5)1273-1279
Shah A, Mehta N, Von Arx DP, Derrick P. Fracture of a dental needle during administration of an inferior alveolar nerve block. Dent Update. 2009; 36:20-25
Rout PGJ, Saksena A, Fisher SE. An investigation of the effect on 27-gauge needle tips following a single local anaesthetic injection. Dental Update. 2003; 30:370-374
Sen P, Waith C, Clarke S. Fractured dental needle at the base of skull. J Cranio-Maxillofac Surg. 2006; 34:136-137
Nezafati S, Shahi S. Removal of broken dental needle using mobile digital C-arm. J Oral Sci. 2008; 50:(3)351-353
Pogrel MA. Broken local anaesthetic needles. J Am Dent Assoc. 2009; 140:(12)1517-1522
Case report: fractured needle in the pterygomandibular space following administration of an inferior dental nerve block Edmund Bailey Jeethendra Rao Alka Saksena Dental Update 2024 42:3, 707-709.
Fortunately, needle fracture is a rare complication following the administration of dental local anaesthetic. We present a case of needle fracture following administration of an inferior dental nerve block. The fractured needle was retrieved successfully under general anaesthetic. We also provide some suggestions on how to prevent needle fracture, and advice on how to manage the situation should it arise.
Clinical Relevance: Dental practitioners are the largest user group of local anaesthesia in the UK. It is important that practitioners are aware of the risks to the patient of needle fracture, how to minimize the risk of this occurring and be aware of how to manage the situation should it arise.
Article
Fortunately, needle fracture is a rare complication following the administration of dental local anaesthetic injections.1 Evidence seems to suggest that needle fracture is more common when giving an inferior dental nerve block than it is with other dental infiltration and block techniques. Since the introduction of disposable needles in the 1960s, along with improvements in metal alloys and manufacturing processes, needle fracture has become even less common.2 On reviewing historical literature, we came across a 1924 study by Blum,3 documenting 65 cases of broken needles over a 10-year period.
Needle fracture may occur due to:
Poor technique;
Patient movement during administration;
Needle manufacturing faults.
Needle selection
Commonly used needles in dental practice in the UK include:4
23 mm (short) 30 gauge (narrow) for infiltration anaesthesia; and
35 mm (long) 27 gauge (wide) for regional block anaesthesia.
Case report
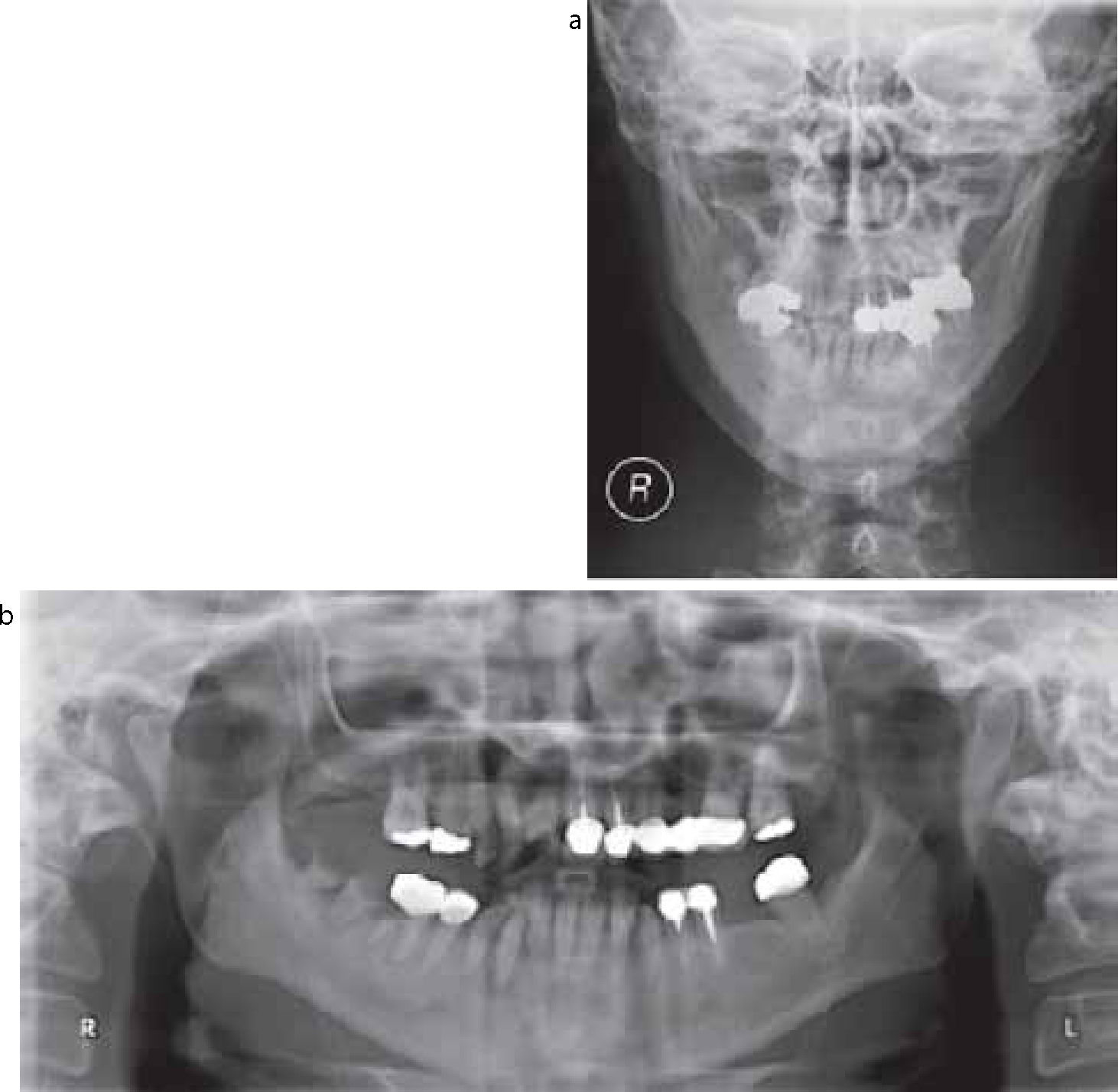
A 32-year-old medically well female attended her dentist for routine mandibular dental extractions, for which an inferior dental nerve block on the right-hand side was required. While using a disposable 23 mm 30 gauge dental needle, and during administration of a second block, the needle fractured in the soft tissues and the dentist was unable to visualize the fragment in order to retrieve it. The proposed treatment was abandoned and the patient was referred urgently to the maxillofacial department by her GDP. On presentation, the patient was somewhat distressed by the situation. On examination, there was tenderness in the retromolar region, trismus, but no sign of the needle. Orthopantomogram and posterior-anterior mandibular radiographs revealed a linear radio-opaque object with a bend, in the pterygomandibular space, representing the needle fragment (Figures 1 and 2). The patient was admitted for exploration of the pterygomandibular space for removal of the needle under a general anaesthetic. The risk of damage to the inferior dental and lingual nerves was discussed with the patient and consent was gained.
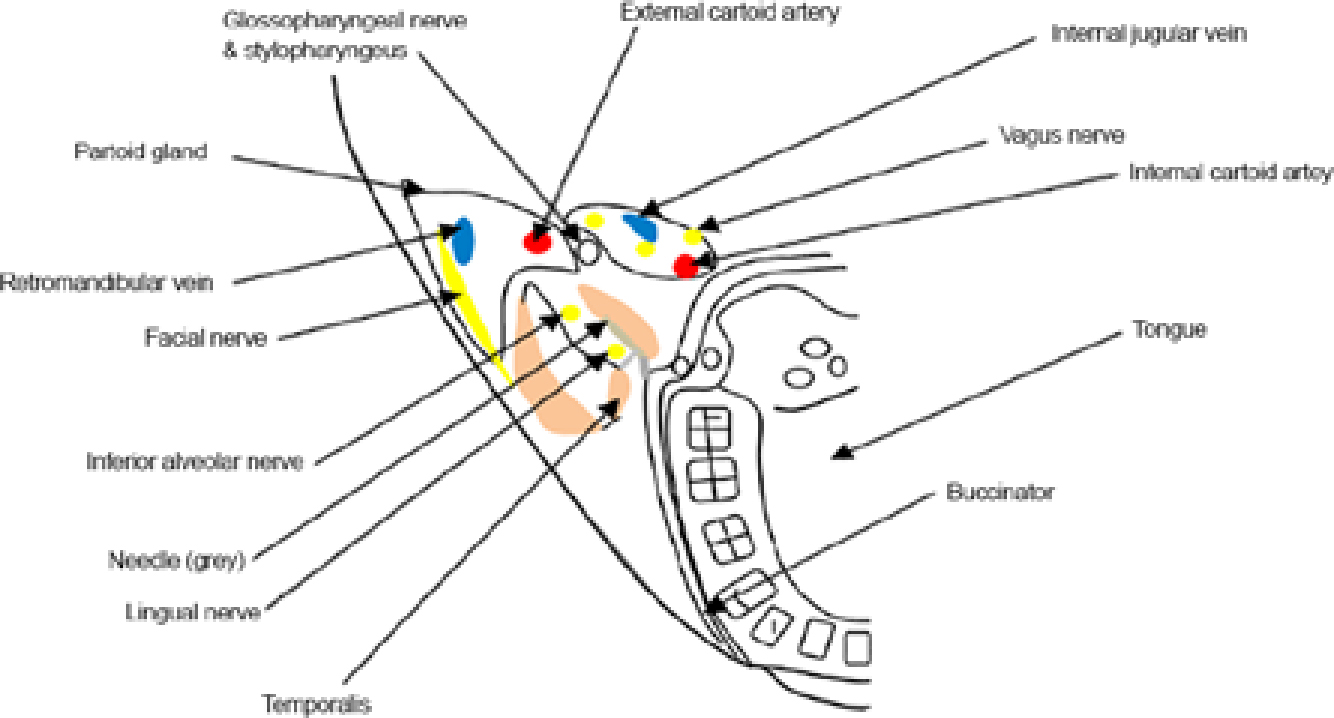
Figure 1. Horizontal section through the pterygomandibular space above the mandibular foramen.Figure 2.
(a) Posterior/anterior view of the mandible and (b) an orthopantomogram showing needle location.
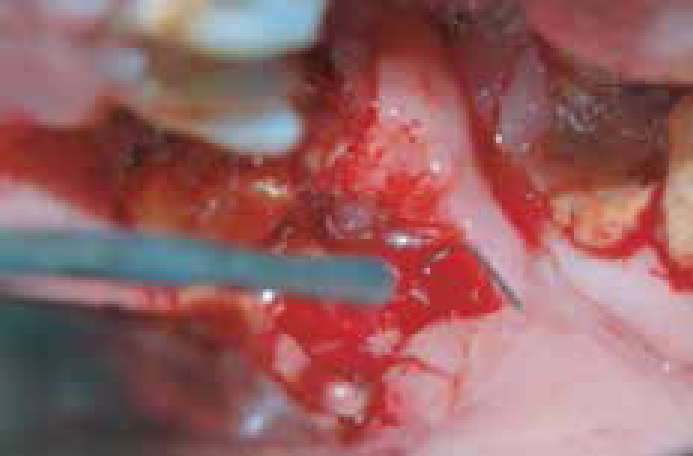
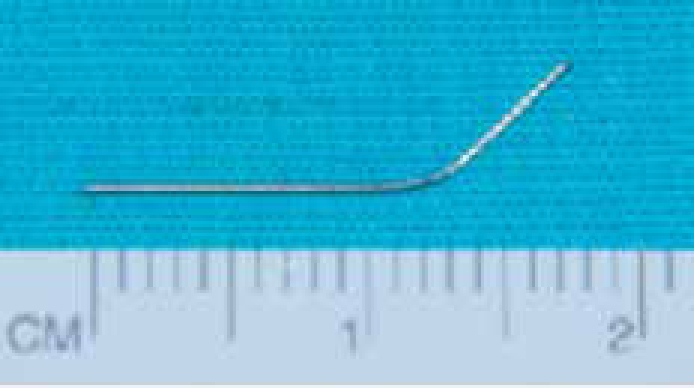
During surgery, a retromolar incision medial to the ascending ramus was made, followed by superficial blunt dissection of the pterygomandibular space in order to minimize risk of damage to the mandibular division of the trigeminal nerve and associated blood vessels (Figure 3). The retrieved needle was noted to be bent (Figure 4). The patient was discharged later the same day and made an uneventful recovery. At 3 week review, the patient was found to have no labial or lingual paraesthesia and her trismus had almost fully resolved.
Figure 3. Intra-operative view of needle retrieval via supraperiosteal incision at the antero-medial aspect of the ramus of the mandible.Figure 4. The needle following retrieval.
Discussion
Different imaging modalities have been suggested when locating needles embedded in the soft tissues: a stereotactic technique5 using an image intensifier and standard venepuncture needles as reference points can be used. Images are quickly available (compared to intra-operative radiographs) and can be viewed immediately. Image intensifiers are usually readily available owing to their common use in orthopaedic surgery. Image intensifiers are electronic devices used to produce a fluoroscopic image with a low-radiation exposure. A beam of x-rays passing through the patient is converted into a pattern of electrons in a vacuum tube. The electrons are accelerated and concentrated onto a small fluorescent screen, where they present a bright image, which is generally displayed on a video monitor.6 However, in this case, plain radiographs adequately aided the retrieval. Ethunandan et al discuss the difficulties encountered in location of the fractured needle when only plain radiographs are utilized.1 Cone Beam Computerized Tomography (CBCT) or conventional Computerized Tomography (CT) imaging provides the precise location of the needle within the pterygomandibular space in the coronal, sagittal and transverse planes. It also provides a 3-dimensional reformatted image and can be invaluable for the surgeon undertaking retrieval of the fractured needle. Ultrasound-guided retrieval of foreign bodies can also be used,7 the advantages of this real-time procedure and the use of small instruments minimize bleeding time and avoid injury to surrounding structures. Patient compliance is enhanced by the fact that the procedure has little or no aesthetic impact. This would not be appropriate in this case as the foreign body (the needle) was impacted deep in the soft tissues, the examples used in the study by Callegari et al7 are retained in the soft tissue underneath the skin.
Needle fracture in tissues is an uncommon but devastating event for both the patient and clinician. In the literature there are several examples of this occurring following the administration of an inferior dental nerve block,1,2,3,5,8,9,10,11,12 with the majority of these involving short needles. Short needles are more prone to fracture when used for inferior dental nerve blocks as they have to be inserted to the hub (where the needle attaches to the thread) to provide adequate anaesthesia. It is known that needles are at their weakest at the hub.4 Manipulation of the needle by bending it mid shaft can potentially generate forces that can weaken it at the hub. We were unable to find any examples of needle fracture relating to other dental anaesthetic injections. In several of these cases, the needle fracture occurred on the second or subsequent administration of local anaesthesia.8,12 This would imply that the needle might be weakened on re-use. In a study examining long needles used in single inferior dental nerve blocks, scanning electron microscopy revealed 95% had needle tip damage.9 The study advised that needles are replaced after each injection, as per the manufacturer's guidance.13
Needle fracture should be dealt with promptly to reduce pain and to avoid risk of wound infection and swelling, which may inhibit its retrieval. There is also the possibility of migration of the needle into other spaces such as the peritonsillar space medially, infratemporal fossa and skull base superiorly,10 parotid gland and lateral pharyngeal space posteriorly, and sublingual and submandibular spaces inferiorly.
Contents of the pterygomandibular space (Figure 1) include the mandibular division of the trigeminal nerve and inferior alveolar artery and vein. Contents of the lateral pharyngeal space include the carotid artery and branches together with the 9th (glossopharyngeal), 10th (vagus) and 12th (hypoglosssal) cranial nerves. Deep infratemporal contents include the pterygoid plexus, which communicates with the cavernous sinus and ophthalmic veins, the interior maxillary artery and vein and the mandibular division of the trigeminal nerve. The patient must be advised of the inherent risks associated with surgical intervention of these spaces and consequences of spread of infection and/or damage to the blood vessels and nerves which are present.14
To reduce the risk of needle fractures it is recommended that:
Needles should conform to European standards and be CE certified;
Only long (35 mm) needles are used for inferior dental nerve blocks;
Needles should not be manipulated prior to use, by bending or breaking;
When giving local anaesthetic injections, needles should not be subject to extreme or repeated movements, nor should they be inserted to the hub;
Needles should be replaced after every use, due to needle point damage. Disposal would also avoid the risk of needle stick sharps injury.
Management
Upon realizing that a needle has fractured, the dentist should immediately attempt retrieval with a fine mosquito/haemostatic clip if the needle is visible. If the needle cannot be retrieved, the patient should be informed, advised of the clinical risks of leaving the needle in situ and referred to the nearest oral and maxillofacial surgery unit for further investigation and management. Following appropriate radiographic imaging and patient consent, the patient should undergo surgical exploration and retrieval of the fractured needle under general anaesthesia. Retrieval should be performed as soon as possible to prevent complications, such as migration of the needle,1,10 tissue space infection, and also to prevent the pain and discomfort caused by having a needle imbedded in the soft tissues.1
Conclusion
Needle fracture during inferior dental block administration is rare but continues to be reported in the dental literature. By use of a careful technique and the following of manufacturer's instructions, dental local anaesthetic needle fractures can be minimized. Following fracture of a dental needle, prompt retrieval in a specialist oral and maxillofacial department is required to minimize risk of developing serious complications.