Velasco MG, Ysunza A, Hernandez X, Marquez C. Diagnosis and treatment of submucous cleft palate: a review of 1008 cases. Cleft Palate J. 1988; 25:171-173
Reiter R, Brosch S, Wefe Hl, Schlomer G, Haase S. The submucous cleft palate: diagnosis and therapy. Int J Pediatr Otorhinol. 2011; 75:85-88
The incidence of submucous cleft palate is between 1:1250–1:6000. It is important for this relatively silent deformity to be identified early and referred appropriately as a delay in diagnosis may affect the patient's quality of speech in the long term. This paper presents a case of submucous cleft palate which was diagnosed late (age 14). Nevertheless, by the appropriate intervention of the multidisciplinary cleft team, the patient was treated successfully.
Clinical Relevance: Dentists and doctors need to be aware of the signs and symptoms associated with submucous cleft palate so that they can refer the patient to an appropriate specialist centre for further investigation and treatment. Moreover, patients with this condition are shown to have a higher incidence of dental abnormalities, such as hypodontia and peg-shaped laterals.
Article
Submucous cleft palate is a subgroup of cleft palates and describes an intact palatal mucosa with a cleft in the musculature of the soft palate. This congenital deformity is a result of incomplete fusion of the muscles of the soft palate during palatogenesis and sometimes the palatine bone is also involved. It occurs at approximately the 6th–7th week of intrauterine life. The incidence of submucous cleft palate is between 1:1250–1:6000.1
Signs
The clinical signs associated with this deformity have been described by Calnan in 1954 (also known as the Calnan triad).2 They are:
Notched posterior hard palate: one study showed it to be present in 100% of the cases (108 patients).3 A more recent study, however, stated a value of 68% (439 patients).4
Bifid uvula: this sign is present in 59% of cases (439 patients)4 and provides the easiest means of identification of the potential underlying condition.
Zona pellucida: this is a thinning of the midline mucosa which can be seen as a translucent zone in the midline of the palate and is a manifestation of a cleft in the palatal muscles, ie levator veli palatine muscle. This is present in 45% of cases.4
However, the complete classic triad of signs described by Calnan are only present in 23.9% of cases.4 This may account for the late detection of this condition, particularly when the uvula is intact.
Symptoms
Speech
Speech-related abnormalities are generally not fully developed in the early stages of life. They often present themselves late, which can result in delayed detection by the cleft team. The symptoms arise mainly as a result of the abnormal position of levator veli palatine muscle. This muscle is displaced anteriorly which results in increased escape of air from the oropharynx to the nasopharynx, leading to velopharyngeal insufficiency (VPI) and presents as hypernasality. A recent study showed that hypernasal speech was present in 51% of cases of which 22% were severe.4
Hearing loss
Velopharyngeal insufficiency (VPI) may also result in Eustachian tube malfunction which can present as otitis media with conductive hearing loss. This feature is shown to be present in about 45.1% of cases with submucous cleft palate.4
Nasal reflux of meals and liquids
Nasal reflux of meals and liquids is said to be present in 21.6% of cases.4
Management
Conservative approach
This approach is only appropriate if there is no or mild VPI present and involves speech therapy.
Surgical approach
Surgical correction is only indicated in the presence of significant VPI. The aim is to restore the seal between the oropharynx and nasopharynx in order to facilitate normal articulation of speech. Several surgical techniques have been described in the literature, however, they all basically involve rearranging the muscle insertions and repositioning them into their normal place by a procedure known as a palatoplasty.
Case history
A 14-year-old female was referred to the orthodontic department of the John Radcliffe Hospital Oxford by her dentist with regards to her developing Class III malocclusion. The patient had no other complaints. Apart from a severe peanut allergy, she was medically fit and well. As a child she had a strawberry naevus on her upper lip which had resolved spontaneously and without intervention. The patient was a keen musician and actor.
On examination, she had a Class III incisor relationship on a Class III skeletal base with maxillary hypoplasia and increased maxillary/mandibular plane angles. Her oral hygiene was poor. She had a reverse overjet (Figures 1, 2), crowded upper arch and retained LRE and LLE (Figure 3). Her orthodontic treatment commenced with expansion of the upper arch using rapid maxillary expansion (RME) (Figure 4). Fixed appliances were then bonded in upper and lower arches. A few appointments into treatment, her slightly nasal speech continued. The patient admitted she always sounded ‘bunged up’.
Figure 1. Full facial view pre-treatment.Figure 2. Profile view pre-treatment.Figure 3. Occlusion at the start of treatment.Figure 4. Rapid maxillary expansion in situ.
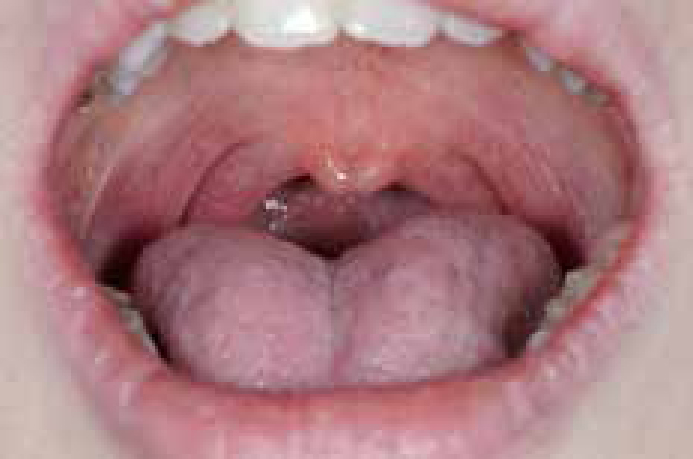
On further examination, it was evident the patient had a bifid uvula (Figures 5, 6). A cleft oral and maxillofacial surgeon's opinion was sought and subsequently the patient was referred to the cleft team for further investigation.
Figure 5. Uvula in the resting position.Figure 6. Bifid uvula with the patient producing the sound of ‘Ah’.
A speech and language opinion found normal palatal elevation on production of the sound ‘Ah’. Formal assessment was carried out using the Great Ormond Street Speech Assessment (GOSSA). Assessment indicated mildly hypernasal resonance with no audible nasal emission. No nasal turbulence or grimace was noted.
Video nasopharyngoscopy was performed to visualize the naso/oropharynx and to determine the presence of a velopharyngeal insufficiency. This showed a very thin strand of palatal tissue with very anteriorly placed levator muscle. A large Passavant's ridge was seen on the posterior pharyngeal wall. The diagnosis of submucous cleft was confirmed. In light of her VPI, a formal sommerlad palatoplasty (Figure 7) was undertaken (radical levator muscle repositioning).
Figure 7. Appearance of the palate post palatoplasy.
The patient made an uneventful recovery (Figures 8, 9) and her fixed appliances were removed 6 months later. Speech and language therapy assessment, using the Great Ormond Street Speech Assessment, identified inaudible nasal emission, excellent articulation and her hypernasality was resolved. The patient felt that her speaking voice had improved post-operatively and that ‘she had learned to speak differently’. She felt that her singing voice was unchanged.
Figure 8. Full facial profile post-treatment.Figure 9. Occlusion post orthodontic treatment.
Discussion
The diagnosis of submucous cleft palate remains a clinical challenge as its signs and symptoms are easily missed or overlooked. Late diagnosis in turn makes the treatment and management of these cases more difficult and the outcome may be less favourable. As demonstrated in this case, if it had not been for her Class III skeletal relationship and crowding, it is likely that this condition would have been missed and the patient would have had to live with persistent hypernasality.
Conclusion
An awareness of the limited signs and symptoms of this condition is all that is needed for these cases to be identified and treated successfully.
A patient that has persistent hypernasality and always sounds ‘bunged up’ should alert the clinician for further investigation or referral. It is the responsibility of all general dental practitioners and all head and neck specialists to look actively for the Calnan triad of signs in their clinical examinations in the presence of hypernasality.