Watson TF, Flanagan D, Stone DG. High and low torque handpieces: cutting dynamics, enamel cracking and tooth temperature. Br Dent J. 2000; 188:(12)680-686
Kenyon BJ, Van Zyl I, Louie KG. Comparison of cavity preparation quality using an electric motor handpiece and an air turbine dental handpiece. J Am Dent Assoc. 2005; 136:(8)1101-1105
The dental handpiece is a frequently used instrument in the clinician's armamentarium. Dental handpieces were first introduced in the nineteenth century as primitive hand-operated devices. Advances in technology have enabled modern handpieces to evolve into sophisticated, engineered precision instruments. The most common handpieces are operated by compressed air or by electric motors. The current market offers a variety of handpieces to suit specific clinical needs. Care and maintenance of all dental handpieces is essential to ensure maximum efficiency and longevity. This paper offers a brief insight into the history of dental handpieces and illustrates what the current market has to offer, with recommendations on care and maintenance to avoid the common problems encountered by clinicians.
Clinical Relevance: Selection, knowledge and maintenance of the dental handpiece are key for effective clinical practice.
Article
Brief history
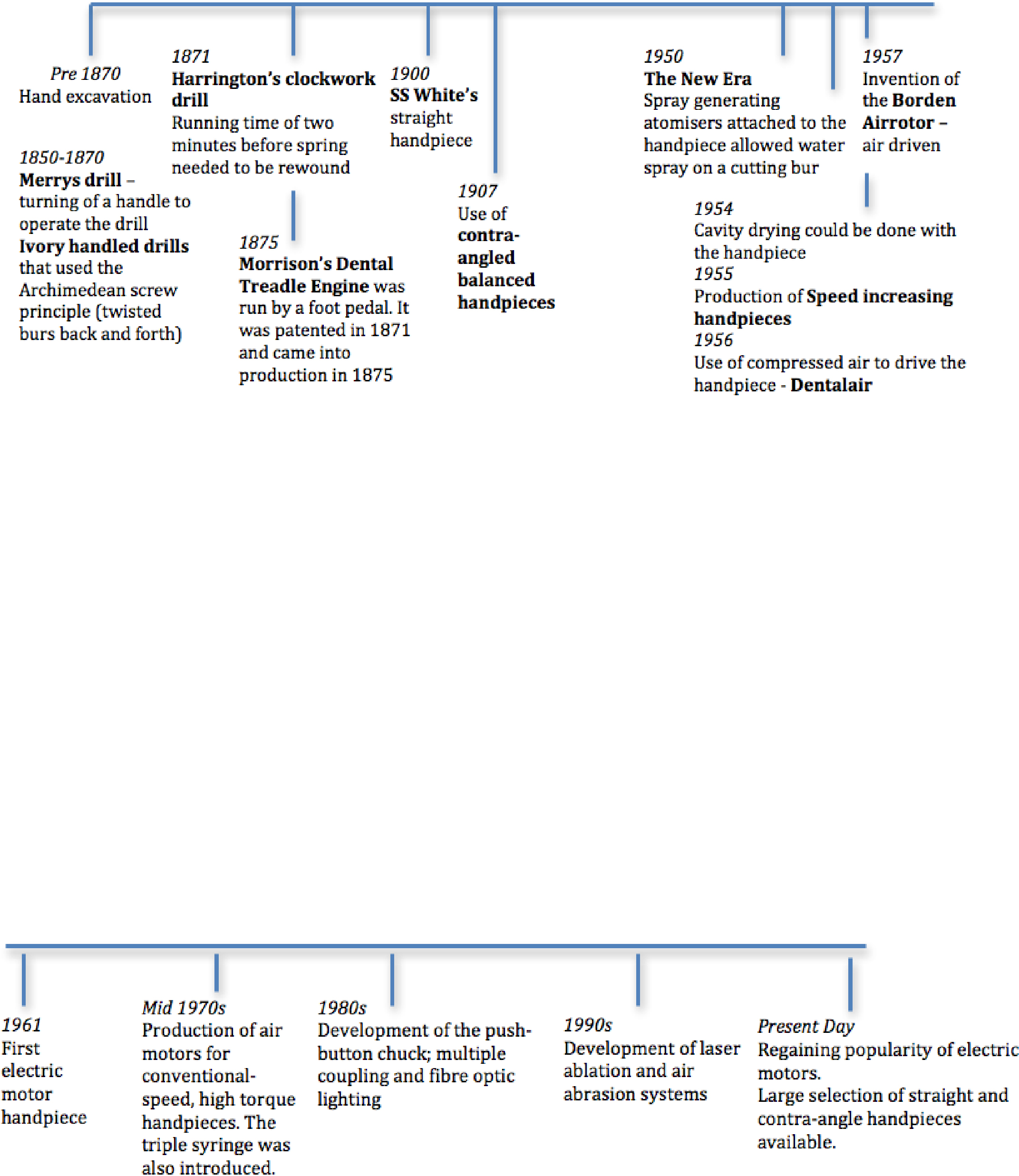
The timeline,1 incorporating Figures 1–3, illustrates the rich history of modernizing technology and ergonomic designs incorporated into the dental handpiece. Over the last 140 years our handpieces have evolved from the historic manual wind-up mechanism to the sophisticated engineered devices we depend upon today.
Figure 1. Full unit from 1935 reproduced with permission from W&H.Figure 2. Handpiece from 1895 reproduced with permission from W&H.Figure 3. Endodontic cursor from 1926 reproduced with permission from W&H.
Harnessing the power of water and electricity, the handpiece delivers impressive torque, powering a controlled cut with which we are able to modify tooth surface. Even in its most simple design it is a core technology in our dental armamentarium. Used for most dental operative procedures from caries excavation to crown and bridge preparations to surgical sectioning of teeth and bone removal, the dental handpiece is a significant investment, with few of us retaining the knowledge and understanding of the intricate mechanisms behind this technology.
When cared for correctly, these potentially delicate instruments can serve us for 30 years – a sizeable proportion of our working career. Admittedly, the majority of clinicians may choose to update their handpieces well in advance of this; nonetheless we may agree that we would appreciate our handpieces to stay reliable and in good working order, maximizing the return on our investment. Handpiece repair costs can be a high recurring expense to all dental practices and, whilst unavoidable due to repeated sterilization, with adequate care we can aim to minimize the adverse effects of prolonged, repeated use.
As technology develops, the market has many manufacturers, each with a variety of different designs and unique selling points. We are still far from the perfect handpiece: that which is affordable for single use thus eliminating the need for decontamination and maintenance requirements. Currently, most handpieces have many common features and provide qualities approaching an ideal. However, despite this, today's handpieces are efficient enough for a clinician to cut away sound tooth easily, with the potential for over preparation – a compromise made for faster and easier tooth preparation. The ideal qualities of a dental handpiece, adapted from Handpieces and Burs: The Cutting Edge are:2
Safe and effective;
Variable range of speeds;
Maximizes productivity;
Minimizes dental trauma;
Enables gross hard tissue removal;
Enables preparation refinement;
Offers sufficient power and torque;
Easy placement and removal of burs;
Bur retention;
Minimizes patient discomfort;
No maintenance requirements;
Longevity;
Enables or enhances visualization;
Light weight;
Good grip and handle configuration;
Ergonomically designed;
No noise or vibration;
Easy to sterilize/affordable single use;
Cost-effective;
Designs suited specifically to left- and right-handed use.
Manufacturers in the handpiece industry include Bien-Air, Dentsply, KaVo, NSK, and W&H. Together they provide handpieces to suit every need: from a handpiece that is used solely for tooth polishing to one that is used to remove bone. Handpieces may be categorized as those driven by compressed air and those driven by electric motors. The use of electric motor driven handpieces that create high speed and high torque are not new to the market but are increasingly being used over the traditional air turbine handpieces in both Europe and the United States.3 Comparisons documented in the literature by Watson et al4 suggested that, on increasing resistance to the bur, the air turbine will stall, whereas the electric speed-increasing handpiece performed consistently, regardless of the load applied to the bur. There was no significant difference found between the two in terms of heat generation and damage to tooth structure. Kenyon et al5 compared cavity preparations using the electric motor driven handpiece (high-speed high-torque) and the air turbine (high-speed low-torque), finding no significant difference between the performance of the two designs.
Air-driven handpieces
The advent of Dr John Borden's pioneering air rotor, in 1957, paved the way for faster efficient cutting, minimizing chairside time. The concept of the compressed air-driven handpiece relies on pressurized air flowing through a turbine to engage a friction-retained bur. The head of the handpiece contains the turbine that comprises multiple small components. The major component is the impeller that catches the drive air, causing the turbine to rotate. The bearings sit on either side of the impeller and can be made from stainless steel or the more expensive ceramic option (Figure 4). Owing to the relatively delicate nature of these bearings, it is these parts that are the most susceptible to failure. Any significant resistance met by the bur will stall its movement. As a result, the bur will not rotate concentrically and there may be significant vibration contributing to lack of precision, patient anxiety and operator fatigue.
Figure 4. Cut away diagram of modern air rotor turbine reproduced with permission from W&H.
Stalling of the bur, excessive vibration upon use, loud sounds emanating from the handpiece, lack of concentricity of the bur and the expelling of black matter when the handpiece is lubricated should lead to suspicion of disintegration of the bearing cage.
As technology progresses, handpieces have continued to evolve to lighter, smaller and quieter models, with additions of coolant to minimize thermal trauma to the tooth caused by the increased RPM. The handle of the air turbine contains tubing for the drive air, chip air (air supplied from the dental unit through the handpiece to the cutting surface of the tooth) and water/irrigation spray. Some varieties incorporate illumination, incorporating fibre optics, glass rods or LED bulbs to deliver light directly at the cutting tip of the bur. However, these features are limited to the high-speed handpieces (Figure 5).
Figure 5. Air rotor reproduced with permission from NSK.
Electric handpieces
The advent of the electric motor introduced levels of torque and precision unavailable with air-driven systems. The unique selling point of the electric handpiece is the ability for it to maintain consistent speed and cutting efficiency despite any resistance to cutting – often five times the power of that offered by the air-driven handpiece. The operator has the luxury of adjusting RPMs and torque to decide the exact speed to complete intricate work and, due to the power of the electric motor, the bur maintains efficiency to cut tooth at high resistance and even at a very low speed. The electric motor allows for quicker preparation time whilst producing less noise and vibration than its air-driven counterpart, beneficial to both the patient and the operator. However, the high torque of these instruments results in increased heat generation. To combat this issue, manufacturers have introduced multiple ports in the head of the handpiece to maximize the coolant spray. Attention should be paid to ensure that this is directed on to the tooth surface being cut, to minimize thermal trauma.
Traditional models were bulky and heavy. The handpieces may look and feel similar to slow-speed air-driven handpieces. The relatively slow uptake and poor acceptance of these handpieces has been due to bulkiness and product warning issues related to heat generation. Repairs for electric motors are reputed to be costlier than for air-driven motors. If poorly maintained, the internal bearings and attachments can wear and fail. When the handpiece is used again, power from the electric motor continues to drive the handpiece as normal. The resultant friction generates heat with potential to cause burns in patients. The burns may not be detected until tissue damage has already been done, as the patient may be anaesthetized and the housing insulates the operator from the increase in temperature. The US Food and Drug Administration have issued a public notice regarding burns from electric handpieces in 2008.6 Proper maintenance, flushing and lubrication can help to prevent such occurrences.
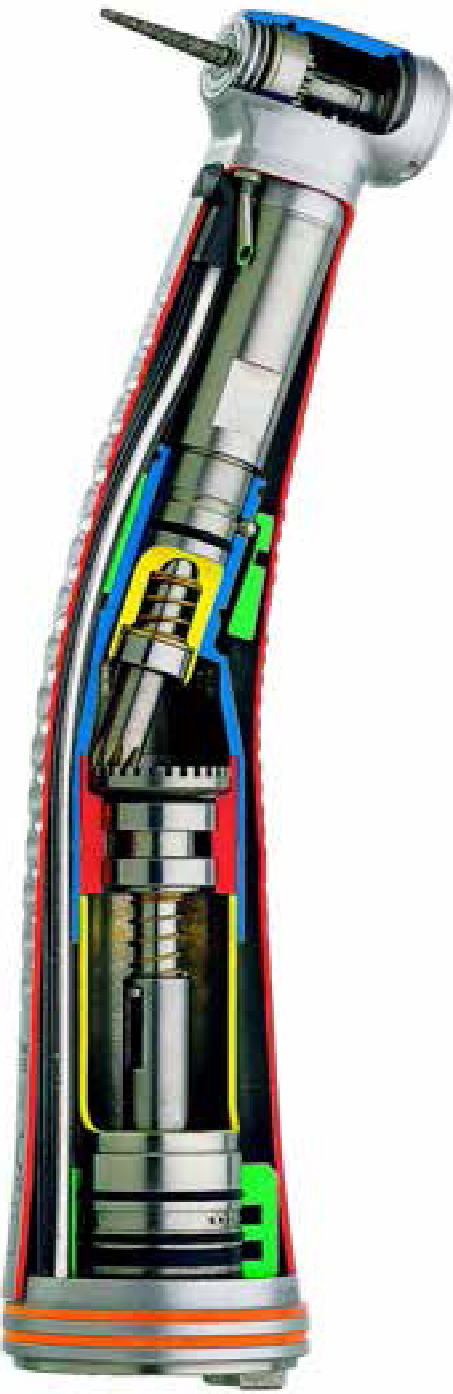
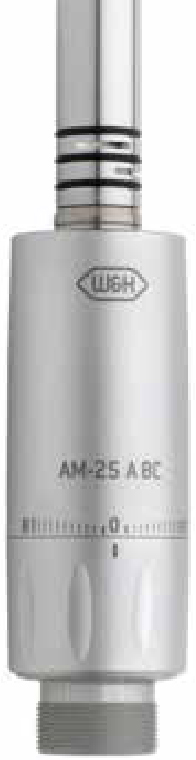
Lighter, smaller, quieter models that are easier to maintain and simple to operate have superseded these models (Figure 6). Modern electric handpieces and motors (Figure 7) have been welcomed into the market. Speed increasing attachments, commonly identified with a red band at the base or labelled as 1:5 or 1:2, are ideal for use for the majority of restorative needs, such as cavity and crown/bridge preparations (Figure 8a), as well as surgical uses such as sectioning teeth (Figure 9).
Figure 6. Cutaway diagram of an electric handpiece reproduced with permission from KaVo.Figure 7. Motor attachment reproduced with permission from W&H.Figure 8. Selection of electric motor attachments reproduced with permission from NSK. (a) Contra-angle for restorative procedures (speed increasing). (b) Straight surgical handpiece (1:1). (c) Contra-angle polishing attachment (1:1). (d) Contra-angle implant handpiece (speed reducing).Figure 9. Surgical handpiece unit reproduced with permission from W&H.
Blue-banded handpieces labelled 1:1 are ideal for chairside adjustments and hygiene, such as polishing. Typically, they transfer the exact speed of the motor to the bur, hence a 1:1 relationship (Figures 8b, c). Colour-coded banding on electric attachments allows for simple, easy identification.
Speed reducing attachments for the electric motor are used extensively for driving rotary Nickel Titanium endodontic files. Features include delicate torque thresholds to control the degree of file twisting, auto-reverse function and constant speed – hence the logical choice for endodontics. Endodontic selections rotate the bur at a slower speed than the motor, often identified with a green band and typically the numbers 8:1, 10:1 or 16:1.
The use of speed-reducing handpieces extends to surgical procedures such as the removal of bone, sectioning of teeth and placement of dental implants. Such attachments may have dual irrigation function to allow for sterility (Figure 8d). The use of an air turbine for surgical procedures is not recommended as it can result in air emboli, and complications such as subcutaneous emphysema, pneumothorax, pneumopericardium and pneumomediastinum have been historically documented.7
Common problems with handpieces
Diligent maintenance is paramount to ensure smooth function. Problems that may occur due to less than ideal care or handling include:
Wearing out of bearings;
Damage to the latch grip causing the bur to rattle in the head;
Blocking of water channels;
Dinting of the head when the handpiece is dropped, causing impeded movement of the turbine;
Shattering of the glass rod in illuminated handpieces.
Maintenance
Compliance to the manufacturer's directions for cleaning and lubrication of handpieces may contribute to an increase in bearing life.8 General care, such as the air pressure produced by the compressor, should not be ignored. Each handpiece has an optimum PSI range that should be acknowledged. Inadequate air pressure will provide insufficient power and excess air pressure is likely to damage the handpiece and reduce longevity.
The manufacturer's instructions should be followed as routine when the handpiece is used, preferably using the products the manufacturer provides for cleaning the handpiece. The following steps have been adapted from Kavo and W&H maintenance instructions:
Run the handpiece with the bur in place and the water on, to purge the instrument (AVOID running the instrument without a bur in place);
Remove bur or rotary instrument from the handpiece;
Turn off water spray feed on dental unit, disconnect the handpiece from the coupling by 3–5 mm, hold firmly and operate drive air for 2 seconds. This is to blow water out of the spray channel, as calcium deposits in the water may lead to blockages. An alternative would be to use the air supply of the 3/1 syringe;
Remove the handpiece from the drive source;
Place the handpiece in the washer-disinfector and run the cycle in accordance with the HTM-01-05 guidelines. Do NOT place the handpiece in an ultrasonic bath or immerse in water or cleaning solutions;
Lubricate the head and handle separately with a handheld spray or machine as per the manufacturer's guidelines. Use a tissue to clean off any excess lubricant. If done with a handheld spray, check to see if oil leaves the head of the handpiece ensuring it has passed through the whole mechanism;
Package the handpiece and sterilize it in the autoclave in accordance with the HTM-01-05 guidelines – do not exceed the manufacturer's recommended temperature;
Allow handpieces to dry fully before use to avoid corrosion to the internal products;
Run the handpiece before use to clear excess lubricant – do not lubricate prior to use;
Avoid contact with corrosive chemicals such as harsh detergents and bleach.
In addition to the above, ensuring that handpieces are serviced in accordance to their usage will maximize longevity in addition to avoiding large repair bills. It should be noted that some repair merchants might use generic cartridges and spare second-hand parts to keep costs down.
Despite the many advances in technology today, it is unfortunate that we are still reliant on destructive ways to try and save teeth – shattering and fracturing our way through enamel and dentine. Technology such as the Er:YAG and Er, Cr:YSGG lasers that use chemo-mechanical means for removing tooth tissue are around today. They allow increased patient comfort, fast tooth removal and even allow tooth preparation without the use of anaesthesia – but currently remain very expensive. Air abrasion systems are less versatile than laser systems and have a long way to go in terms of being able to do anything more than remove a superficial layer of enamel.
New developments
Over the years, handpiece engineering and design has overcome many of the barriers we have faced in the past. The manufacturers are striving towards quieter handpieces, smaller head sizes to maximize vision and accessibility, stronger bur retention to reduce the amount of vibration and improved illumination. For example, Kavo's latest innovation – the Kavo MASTER torque M9000L – has a technology that allows stopping of the turbine within one second. This function increases safety and decreases the time taken to wait for the stopping of burs.
W&H have introduced LED technology that allows the same quality of light regardless of the voltage input and the high colour-rendering index allows daylight quality light to be emitted from the handpiece.
Conclusion
Dental handpieces have been and will continue to be an essential part of the clinician's armamentarium. Advancements in electric handpiece technology have paved the way for easy-to-use, lighter, smaller, quieter models without sacrificing high torque or precision cutting ability.
Dental handpieces are central to the running of the dental practice and maintaining them to the highest standard of care allows them to be preserved far beyond the manufacturer's warranty. Knowledge of your handpieces and appropriate care will help to ensure your handpieces stay efficient, maximizing longevity and minimizing overheads of maintenance and repair.