Altinors N, Caner H, Bavbek M Problems in the management of intracranial meningiomas. J Invest Surg. 2004; 17:283-289
Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, Scheithauer BW, Kleihues P. The 2007 WHO Classifcation of Tumours of the Central Nervous System. Acta Neuropathol. 2007; 114:97-109
Marosi C, Hassler M, Roessler K, Reni M, Sant M, Mazza E, Vecht C. Meningioma. Crit Rev Oncol Hematol. 2008; 67:153-171
Louis DN, Scheithauer BW, Budka H, von Deimling A, Kepes JJ. Meningiomas. Pathology and genetics. Tumours of the nervous system.Lyon: IARC Press; 2000
Rausing A, Ybo W, Stenflo J. Intracranial meningioma – a population study of 10 years. Acta Neurol Scand. 1970; 46:102-110
Longstreth WT, Phillips LE, Drangsholt M, Koepsell TD, Custer BS, Gehrels JA, van Belle G. Dental X-rays and the risk of intracranial meningioma: a population-based case-control study. Cancer. 2004; 100:(5)1026-1134
Hansson CM, Buckley PG, Grigelioniene G, Piotrowski A, Hellstrom AR, Mantripragada K, Jarbo C, Mathiesen T, Dumanski JP. Comprehensive genetic and epigenetic analysis of sporadic meningioma for macro-mutations on 22q and micro-mutations within the NF2 locus. BMC Genomics. 2007; 8
Saloner D, Uzelac A, Hetts S, Martin A, Dillon W. Modern meningioma imaging techniques. J Neurooncol. 2010; 99:(3)333-340
Cook RJ, Sharif I, Escudier M. Meningioma as a cause of chronic orofacial pain: case reports. Br J Oral Maxillofac Surg. 2008; 46:(6)487-489
Aghi MK, Carter BS, Cosgrove GR, Ojemann RG, Amin-Hanjani S, Martuza RL Long-term recurrence rates of atypical meningiomas after gross total resection with or without postoperative adjuvant radiation. Neurosurgery. 2009; 64:56-60
Bindal R, Goodman JM, Kawasaki A, Purvin V, Kuzma B. The natural history of untreated skull base meningiomas. Surg Neurol. 2003; 59:87-92
Intracranial meningioma as a cause of orofacial paraesthesia: a case report Anish Patel Vaidayanathan Murugaraj Mohan Patel Dental Update 2024 41:7, 707-709.
Authors
AnishPatel
BDS(Lond), MJDF RCS(Eng), DipImpDent(Eastman)
Implantologist in General Dental Practice, Senior House Officer, Oral and Maxillofacial Surgery, Oral and Maxillofacial Department, Royal Berkshire Hospital, Reading, RG1 5AN, UK
Meningiomas are the most common benign intracranial tumour and show a rising incidence with age. They present with a wide array of symptoms and, in this paper, we discuss a case report of an intracranial meningioma presenting as paraesthesia of the lower left lip and chin region. Coincidentally, the symptoms manifested soon after a course of routine dental treatment, further complicating the diagnosis of the lesion. This case highlights the importance, to clinicians at all levels, of the wide array of causes of nerve paraesthesia within the orofacial region and how less frequently occurring conditions must be considered at an early stage.
Clinical Relevance: Intracranial lesions should be included in the differential diagnosis of paraesthesia or anaesthesia of a localized area.
Article
Epidemiology
Meningiomas grow slowly from the arachnoid cap cells1 and most commonly occur in the venous sinuses and the skull base,2 around the sixth and seventh decade of life. According to the fourth edition of the World Health Organization (WHO) Classification of Tumours of the Central Nervous System, published in 2007, there are 15 types of meningiomas of which only one variant is malignant.3 They are the most frequently diagnosed intracranial tumour and represent 13–26% of all intracranial tumours.4 In adults, there is a marked female bias with a female:male ratio of 3:2 to 2:1.5
The incidence of meningiomas is increasing over time, particularly in the elderly, and in a large autopsy series it was as high as 1.4%.6 This increase is related to wider indications for cranial imaging, better imaging facilities and ageing populations.
Aetiology
Many causes and risk factors of developing an intracranial meningioma have been documented. High dose ionizing radiation exposure is the primary identified environmental risk factor for meningiomas, with a risk of six-to ten-fold reported. A variety of old studies had linked the number of full-mouth dental radiographs to an increased risk of developing a meningioma, however, the sample sizes were limited and the results were inconclusive. In a more recent case control study of 200 meningioma patients, the authors reported dental x-rays involving full-mouth series performed 15–40 years ago, when radiation exposure from a full-mouth series was much greater than it is now, were associated with an increased risk of meningioma. The authors did not observe an increased risk with bitewings, lateral cephalometric, and panoramic radiographs.7
Additionally, there is an inherited susceptibility, as suggested by family history and candidate gene studies in DNA repair genes. Mutations in the neurofibromatosis gene (NF2) have been proven to increase the risk for meningioma substantially.8 An aetiological role for hormones (both endogenous and exogenous) has been hypothesized as women are twice as likely as men to develop meningiomas and these tumours harbour hormone receptors.
Imaging
Steady improvements in imaging modalities have enabled a new realm of capabilities in the identification and assessment of meningiomas. The detection and accurate diagnosis of meningiomas has been dramatically improved by the availability of modern cross-sectional imaging methods, in particular magnetic resonance imaging (MRI).
An MRI machine uses a powerful magnetic field to align the magnetization of some atoms in the body, and radio frequency fields to alter the alignment of this magnetization systematically. This causes the nuclei to produce a rotating magnetic field detectable by the scanner and this information is recorded to construct an image of the scanned area of the body.9
MRI is the modality of choice as it provides good contrast between the different soft tissues of the body, and has the ability to assess characteristics such as diffusion and perfusion.9 Within the MRI scan, the meningioma usually presents as a sessile or pedunculated isodense mass, associated with dural surfaces with a characteristic ‘mottling’ structure due to the high vascularization.
Presentation
Symptoms are caused by compression of the central nervous system (CNS), perilesional oedema, and obstruction of cerebrospinal fluid (CSF).10 Visual impairments, headaches, anosmia, mental changes and seizures are all frequently occurring signs and symptoms, however, cranial nerve palsies are more common in clinoidal meningiomas. The examination of the relevant cranial nerves and an outline of potential causes of nerve paraesthesia are discussed later on in this paper.
Management
Surgery is the treatment of choice for symptomatic meningiomas. The latest neurosurgical approaches and the better understanding of the anatomy have allowed a more radical resection. Surgical excision of the tumour and its dural base is the most common primary management as it provides the optimal opportunity for long-term remission. Nevertheless, many tumours cannot be totally resected because they are enveloping vital neural or vascular structures. Conventional radiotherapy has proven beneficial for patients with incompletely resected meningiomas.11 Furthermore, it has been used for high surgical risk patients, where the meningioma is located in eloquent or surgical inaccessible areas and patients of advanced age.
Case study
A fit and healthy 52-year-old woman presented with a history of soreness to the left-hand side of the face and tongue for two years. There was also paraesthesia which presented as tingling of the left lower lip and chin region, confirmed by decreased sensation to the pinprick test in this region.
The patient felt the symptoms started to manifest after routine dental treatment two years previously, however, following thorough intra-oral investigations by her dentist and our team, no obvious pathology was detected clinically or radiographically. The dental treatment only involved local infiltrations and simple periodontal therapy, therefore was unlikely to be the cause of permanent nerve paraesthesia. The localization of the symptoms suggested involvement of the trigeminal nerve, in particular the mandibular branch (V3). No other neurological abnormalities were detected clinically.
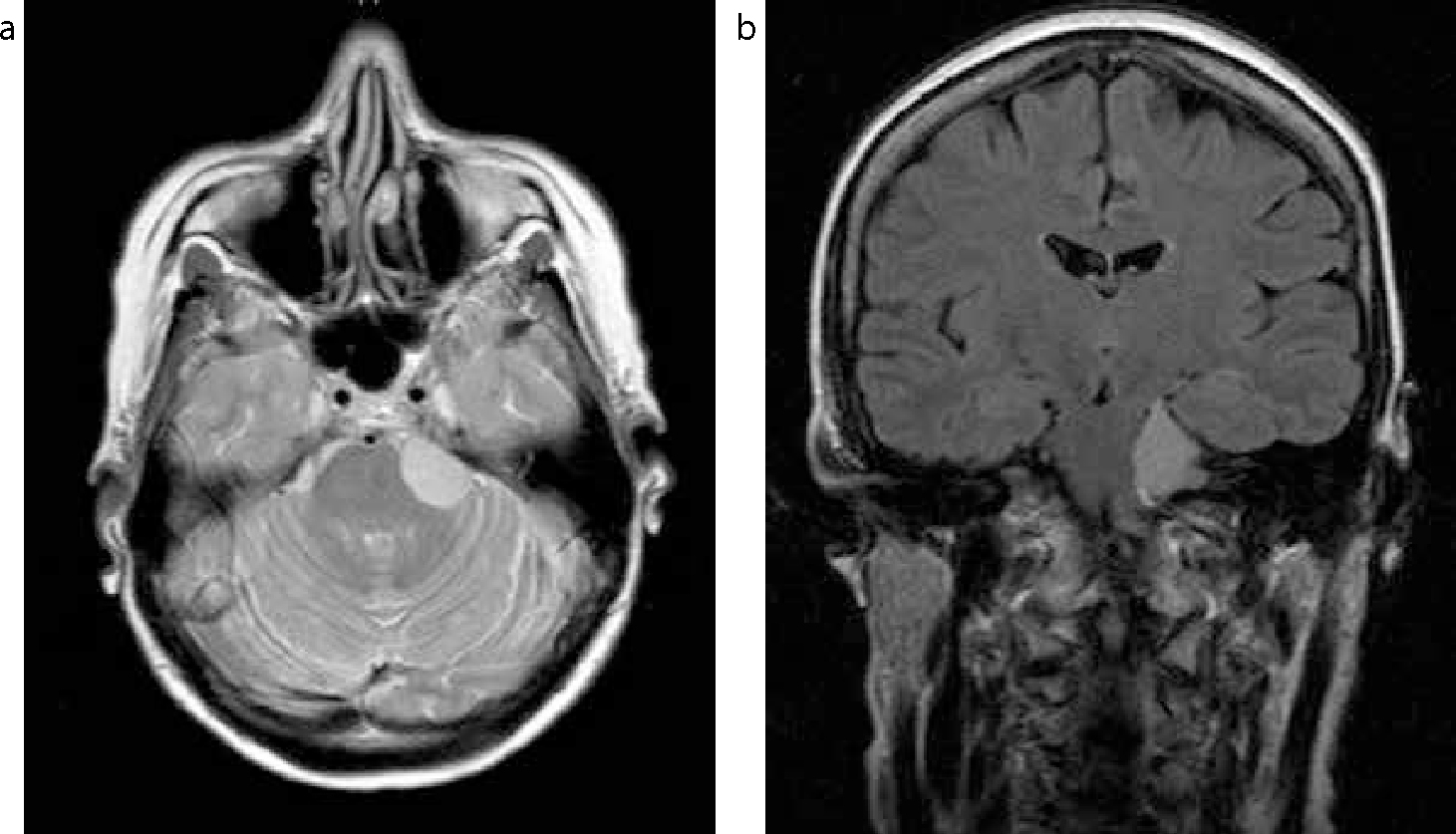
It was at this stage that the authors felt further extra-oral investigations were warranted and an MRI showed a meningioma at the left cerebello-pontine angle, which was referred for neurosurgical assessment (Figure 1). Neurosurgical colleagues discussed at length the treatment options available to the patient, along with the risks and complications attached to each modality. It was advised that surgical intervention to resect this tumour completely had the best long-term prognosis.
Figure 1.
(a, b) Transverse and coronal magnetic resonance images showing the 20 x 22 x 15 mm extra-axial mass lesion at the left cerebello-pontine angle. The lesion is T1 isointense and moderately homogenously T2 hyperintense. The mass does not extend into the internal auditory canal and there is a dural tail within the CP angle cistern. The lesion mildly distorts the adjacent brainstem, but there is no significant compression of the fourth ventricle.
The maxillofacial team planned to review this patient following treatment to assess any improvement in the neurosensory deficit.
Discussion
This case is a gentle reminder to include intracranial lesions as a differential diagnosis of paraesthesia or anaesthesia of a localized area, which is not attributable to any intra-oral pathology. Obtaining a detailed history from the patient often excludes most aetiological factors, however, relevant questions can only be asked if the clinician has a profound understanding of potential causes of nerve paraesthesia. Table 1 provides a comprehensive outline to the local and peripheral causes of paraesthesia to the mandibular branch of the trigeminal nerve.
Local
Peripheral
Traumatic
OedemaMandible fracturePoorly fitting denture (in an area of alveolar atrophy)
Inflammatory
Pulpal necrosis and cystsPeriodontal pathologyOsteomyelitisOsteonecrosis – Bisphosphonate-induced Radiotherapy
Post-herpetic neuralgia
Neoplastic (Benign/Malignant)
Odontogenic tumours and cystsNon-odontogenic tumours and cystsNeural origin
Acoustic neuromaIntracranial space occupying lesions – Meningioma Schwannoma Neuroma Granular cell tumour LipomaMetastatic perineural spread of oro-facial neoplasms
Routine dentistry – Local anaesthetic blocksEndodontics – ApicectomiesMedicaments through the apexOral surgery – Surgical extractionsOpen reduction internal fixation of mandible fracturesOrthognathic surgery
Medications – Allupurinol
A basic neurological examination is an essential tool in a clinician's repertoire to ensure that such lesions are not missed and should include assessment of the motor and sensory distributions of the face, reflexes and ophthalmic signs. A simple assessment should be within the capabilities of a general dental practitioner (GDP), not to provide a definitive diagnosis, but to know when to refer to the local maxillofacial department appropriately. Table 2 provides a basic guideline on how to perform a neurological assessment of the trigeminal and facial nerves.
Trigeminal Nerve – CN5
Facial Nerve – CN7
Corneal reflex: patient looks up and away.
Touch cottonwool to other side;
Look for blink in both eyes – ask if can sense it;
Repeat other side (tests V sensory, VII motor).
Corneal reflex already done.
Facial sensation: sterile sharp item on forehead, cheek, jaw.
Repeat with dull object – ask to report sharp or dull;
If abnormal, then temperature (heated/water-cooled tuning fork/instrument), light touch (cotton).
Palpate temporal, masseter muscles as they clench.
Facial expression muscles: Inspect facial droop or asymmetry.
Patient looks up and wrinkles forehead – examine wrinkling loss and feel muscle strength by pushing down on each side;
Patient shuts eyes tightly: compare each side;
Patient grins: compare nasolabial grooves;
Also: frown, show teeth, puff out cheeks.
Test jaw jerk: clinician's finger on tip of jaw.
Grip patellar hammer halfway up shaft and tap clinician's finger lightly;
Usually nothing happens, or just a slight closure;
If increased closure, think upper motor neurone lesion, especially pseudobulbar palsy.
Previously, diagnosis involved interpreting the symptomatology of meningiomas according to their location and performing an extensive neurological examination. However, the availability of modern imaging techniques has facilitated the diagnosis of meningiomas at an earlier stage.12 Once referred to the hospital, we also suggest investigation by MRI should not be delayed whilst chronic idiopathic facial pain is being investigated, but instead carry them out simultaneously. The risks associated with untreated chronic idiopathic facial pain are significantly less serious than an untreated expanding intracranial space occupying lesion.
Although newer technology has achieved remarkable progress in reducing radiography doses, clinicians should be vigilant and aim to reduce radiation doses, and continue to practise according to the ‘‘As Low As Reasonably Achievable’’ (ALARA) principle. In light of this case, and the literature concerning meningiomas, the authors feel it is appropriate and important to question patients about prior radiation exposures to obtain rough approximations of total past exposures.
If diagnosed early, patients have a good prognosis for intracranial meningioma, and it doesn't have to impact significantly on a patient's quality of life. However, as clinicians, it is imperative to understand more about these lesions and if, after an extensive examination, concerns persist, referral for advice from our specialist colleagues should be sought.