Sanz M, Teughels W Innovations in non-surgical periodontal therapy: Consensus Report of the Sixth European Workshop on Periodontology. J Clin Periodontol. 2008; 35:3-7
Page LR, Rams TE. Subgingival root brushing in deep human periodontal pockets. J Int Acad Periodontol. 2013; 15:55-63
Axelsson P, Lindhe J. The significance of maintenance care in the treatment of periodontal disease. J Clin Periodontol. 1981; 8:281-294
Lindhe J, Nyman S. Long-term maintenance of patients treated for advanced periodontal disease. J Clin Periodontol. 1984; 11:504-514
Worthington HV, Clarkson JE, Bryan G, Beirne PV. Routine scale and polish for periodontal health in adults. Cochrane Database Syst Rev. 2013; (11) https://doi.org/10.1002/14651858.CD004625.pub4
Wennstrom JL, Tomasi C. Periodontal infection control: current clinical concepts. Endodont Top. 2006; 13:3-12
British Society of Periodontology Guidelines.: Basic Periodontal Examination (BPE); 2011
Clinical Examination and Record-Keeping Good Practice Guidelines. 2009;
Clinical Guidelines and Integrated Care Pathways for the Oral Health Care of People with Learning Disabilities. 2012;
Manley G, Skelly M, Hamilton G. Dental treatment for people with challenging behaviour: general anaesthesia or sedation?. Br Dent J. 2000; 188:358-360
Periodontology in General Dental Practice in The United Kingdom. A Policy Statement. 2001;
Listgarten MA. The role of dental plaque in gingivitis and periodontitis. J Clin Periodontol. 1998; 15:485-487
Jepsen S, Deschner J, Braun A, Schwarz F, Eberhard J. Calculus removal and the prevention of its formation. Periodontol 2000. 2011; 55:167-188
Wennström JL, Tomasi C, Bertelle A, Dellasega E. Full-mouth ultrasonic debridement versus quadrant scaling and root planing as an initial approach in the treatment of chronic periodontitis. J Clin Periodontol. 2005; 32:851-859
Koshy G, Kawashima Y, Kiji M, Nitta H, Umeda M, Nagasawa T, Ishikawa I. Effects of single-visit full-mouth ultrasonic debridement versus quadrant-wise ultrasonic debridement. J Clin Periodontol. 2005; 32:734-743
Wang D, Koshy G, Nagasawa T, Kawashima Y, Kiji M, Nitta H, Oda S, Ishikawa I. Antibody response after single-visit full-mouth ultrasonic debridement versus quadrant-wise therapy. J Clin Periodontol. 2006; 33:632-638
Smart GJ, Wilson M, Davies EH, Kieser JB. The assessment of ultrasonic root surface debridement by determination of residual endotoxin levels. J Clin Periodontol. 1990; 17:174-178
Jeffcoat MK, McGuire M, Newman MG. Evidence-based periodontal treatment. Highlights from the 1996 World Workshop in Periodontics. J Am Dent Assoc. 1997; 128:713-724
Frydman A, Nowzari H. Down syndrome-associated periodontitis: a critical review of the literature. Compend Contin Educ Dent. 2012; 33:356-361
Sakellari D, Arapostathis KN, Konstantinidis A. Periodontal conditions and subgingival microflora in Down syndrome patients. A case-control study. J Clin Periodontol. 2005; 32:684-690
: Public Health England; 2014
Cheng RH, Leung WK, Corbet EF. Non-surgical periodontal therapy with adjunctive chlorhexidine use in adults with down syndrome: a prospective case series. J Periodontol. 2008; 79:379-385
Saxén L, Aula S. Periodontal bone loss in patients with Down's syndrome: a follow-up study. J Periodontol. 1982; 53:158-162
Frydman A, Nowzari H. Down syndrome-associated periodontitis: a critical review of the literature. Compend Contin Educ Dent. 2012; 33:356-361
Hanookai D, Nowzari H, Contreras A. Herpesvirus and periodontopathogenic bacteria in trisomy 21 periodontitis. J Periodontol. 2000; 71:376-384
Tanaka MH, Rodrigues TO, Finoti LS The effect of conventional mechanical periodontal treatment on red complex microorganisms and clinical parameters in Down syndrome periodontitis patients: a pilot study. Eur J Clin Microbiol Infect Dis. 2015; 34:601-608
Yoshihara T, Morinushi T, Kiniyo S, Yamasaki Y. Effect of periodic preventive care on the progression of periodontal disease in young adults with Down's syndrome. J Clin Periodontol. 2005; 32:556-560
Newton T, Asimakopoulou K. The management of dental anxiety: time for a sense of proportion?. Br Dent J. 2012; 213:271-274
Young Practitioners Guide To Periodontology. 2012;
Van Winkelhoff AJ, Winkel EG. Antibiotics in periodontitis. Right or wrong?. J Periodontol. 2009; 80:1555-1558
Burke S. Management of aggressive periodontal disease in a patient with Autistic Spectrum Condition (ASC).: BSDH; 2015
Byrd G, Quinonez RB, Offenbacher S Co-ordinated pediatric and periodontal dental care of a child with Down syndrome. Pediatr Dent. 2015; 37:381-385
Al-Tannir MA, Goodman HS. A review of Chlorhexidine and its use in special populations. Spec Care Dentist. 1994; 14:116-122
Stiefel DJ, Truelove EL, Chin MM Chlorhexidine swabbing applications under various conditions of use in preventive oral care for persons with disabilities. Spec Care Dentist. 1995; 15:159-165
Lindhe J, Svanberg G. Influence of trauma from occlusion on progression of experimental periodontitis in the beagle dog. J Clin Periodontol. 1974; 1:3-14
Xu J, Xu B, Song L. [Evaluation of the fiber-reinforced composite periodontal splint on fixing loose teeth with severe periodontitis]. Shanghai Kou Qiang Yi Xue. 2013; 22:81-84
Kumbuloglu O, Saracoglu A, Ozcan M. Pilot study of unidirectional E-glass fibre-reinforced composite resin splints: up to 4.5-year clinical follow-up. J Dent. 2011; 39:871-877
Dougherty N. The dental patient with special needs: a review of indications for treatment under general anaesthesia. Spec Care Dentist. 2009; 29:17-20
Cichon P, Crawford L, Grimm WD. Early-onset periodontitis associated with Down's syndrome – a clinical interventional study. Ann Periodontol. 1998; 3:370-380
Hanookai D, Nowzari H, Contreras A, Morrison JL, Slots J. Herpesviruses and periodontopathic bacteria in Trisomy 21 periodontitis. J Periodontol. 2000; 71:376-384
Moosani A, Sigal MJ, Glogauer M Evaluation of periodontal disease and oral inflammatory load in adults with special needs using oral neutrophil quantification. Spec Care Dentist. 2014; 34:303-312
Periodontal treatment in patients with learning disabilities part 2: professional mechanical intervention Shazia Kaka Chris Dickinson Dental Update 2024 44:3, 707-709.
Authors
ShaziaKaka
BDS, MJDF, RCSEng, MSc M Spec Care Dent
Specialty Registrar (STR) in Sedation and Special Care Dentistry, Oxfordshire Healthcare Foundation Trust, UK (shazia.kaka@kcl.ac.uk)
The first part of this two part series discussed the potential barriers and risk factors that may lead to an increased incidence and severity of periodontal disease amongst patients with learning disabilities. Additionally, preventive strategies and tools that can be used by general dental practitioners, oral health promotion teams as well as specialists within the field to control and prevent disease progression were explored. To prevent periodontal disease progression and attain optimal periodontal health, a combination of prevention and professional mechanical instrumentation is usually required. The second part of the series concentrates on the role of the dental professional in implementing professional mechanical instrumentation to attempt to reduce the burden of disease further in this patient group.
CPD/Clinical Relevance: Although research continues into which professional techniques for instrumentation are the most successful amongst patients with periodontal disease, very little data specifically explore the needs of patients with learning disabilities, despite their high unmet needs. This paper aims to report on any available data present to produce suggestions for care.
Article
In the European Workshop of Periodontology 2008, Sanz et al quoted ‘the performance of oral hygiene practices is an inseparable principle that must be observed with any protocol of mechanical debridement.’ 1 This concept cannot be disputed. Page and Rams reported significant improvements in BOP, PPD and periodontal pathogens in chronic periodontitis patients with the sole use of improved oral hygiene.2 Although this study sample was small (11 patients), the changes observed were statistically very significant. Lindhe et al, with much larger study samples, demonstrated suboptimal oral hygiene to result in continued attachment loss whatever professional treatment was provided,3,4 whils a recent systematic review suggested that routine scaling and polishing without oral hygiene instruction (OHI) may provide no benefit at all.5
As good oral hygiene is so crucial to treatment success, some clinicians will refrain from providing professional mechanical debridement until an adequate level of oral hygiene has been demonstrated.6
In patients with learning disabilities, attaining optimal oral hygiene may be challenging for a number of reasons. These may include medical conditions which directly or indirectly affect an individual's ability to perform an adequate standard of oral hygiene, patient barriers such as poor co-operation and resistance to accepting oral hygiene measures, poor education, training and knowledge of the care-givers who provide their care, as well as inadequate dental access and training of dental professionals.
As far as possible, these obstacles should be faced and any necessary adaptations and solutions implemented as discussed in part 1 of this series.
Even so, a reasonable level of oral hygiene may never reliably be maintained or sustained. To withhold professional treatment for these patients on that basis would not be realistic or justified.
Diagnosis and professional mechanical intervention
Although no formal guidelines exist for those with learning disabilities, a clinical evaluation of periodontal health is crucial for the diagnosis of any new patient. The BSPD and FGDP advise a BPE screening examination to determine the level of clinical and radiographic examination subsequently needed for treatment.7,8 Obtaining a reliable BPE is likely to be dependent upon a number of factors, including operator experience and confidence working with this population group, as well as the co-operation of the patient. Co-operation may be defined by the severity of patients' learning disabilities as well as their fears and anxieties towards dental treatment which, compared to the general population, may be more difficult to discuss and resolve.9
It has been suggested that the vast majority of patients with learning disabilities and challenging behaviours can be successfully treated using behavioural management alone or a combination of behavioural management and adjunctive sedation techniques.10 Ultimately, the technique chosen will be largely dependent not only on the patients' co-operation, but their capacity, medical status as well as treatment needs. A sound knowledge of the Mental Capacity Act is necessary to determine the patients' capacity as well as any supportive methods that may help make their decision. In the case where capacity is absent, liaison with patients' supporting network, including family members, close friends and key carers/support workers, is important and decisions should be recorded in writing. For patients lacking family or unpaid carers, a best interest meeting with the presence of an independent mental care advocate (IMCA) may be required. Further details of this process is not within the remit of this article.
Where a BPE can be established using behavioural management and/or sedation techniques, treatment should ideally be provided as per recommended BSPD guidelines.
For patients whose BPE extends to 2, the main aim is to prevent progression to periodontal disease. Individualized preventive programmes must be discussed with patients and/or care-givers, as appropriate, and scaling and prophylaxis carried out to remove soft deposits and plaque retentive factors. For those patients with BPEs of 3 and 4, a 6-point pocket chart with necessary root surface debridement should ideally be carried out. The recording of specific periodontal parameters such as mobility, recession and furcation involvement are useful to assess levels of change, with treatment if possible.11
The removal of the soft plaque biofilm which contains active periodontal pathogens is the main factor in slowing down disease.12 Calculus, which consists of dead, calcified bacteria, is merely a secondary product of infection. Even in its presence, periodontal healing has been reported to occur.13 In comparison to the quadrant by quadrant root planing that was once advised under LA, a one visit full mouth debridement with an ultrasonic scaler has been shown to be just as effective, significantly more time efficient and a more realistic treatment possibility for this group, where co-operation may be for a limited time period only.14,15,16 Debridement aims at a more conservative instrumentation regimen of overlapping strokes and light pressure for a limited time period, in comparison to aggressive root planing of infected cementum which has been shown not to be warranted.17,18 In those patients where the use of an ultrasonic scaler is not possible, gentle hand scaling and toothbrushing of soft plaque deposits is the most important intervention. The removal of larger calculus deposits is mainly beneficial and necessary to aid the patient or carer in removing soft plaque deposits easier and more effectively.
Recalls
The frequency of recall will largely be determined by the patients' current oral hygiene and periodontal status, their host response (determined by both genetic and environmental factors) as well as their co-operation to toothbrushing. Frydman and Nowzari discussed the importance of scaling and root planing as being initiated early for patients with disabilities and with higher frequency, however the actual time interval was not discussed.19 Sakellari et al in a case study of Downs syndrome patients, agreed with the importance of frequent recall however, again, no time frames were given.20 As per Delivering Better Oral Health guidance, any patient with suboptimal oral hygiene should be recalled at least 3 monthly for reinforcement of prevention, to monitor set goals and to repeat debridement. However, intervals of one month have been reported in very high risk cases.21,22 In comparison to other intellectually impaired subjects, those with Down's syndrome are reported to experience the greatest prevalence and severity of periodontal diseases.23 It is suggested that disease behaviour may be due to the presence of particular periodontopathogenic bacteria and viruses and a decreased ability to eradicate normal periodontal pathogens due to immune defects, including reduced neutrophil and monocyte chemotaxis, impaired neutrophil phagocytosis, reduced T-lymphocyte counts and immature T-lymphocytes.24,25,26 Regular recall has not only been shown to suppress the severity and progression of disease but may also help acclimatize the patient to the dental environment, potentially increasing confidence and co-operation.25,27,28 Careful monitoring is essential and any deterioration should be supplemented with a more regular recall frequency.
Antimicrobials
There is no indication for using systemic antibiotics to manage chronic periodontitis cases.29 However, given the increased incidence of aggressive periodontitis in certain learning disability groups, radiographs and the clinical picture should be thoroughly assessed. A very young patient with advanced, clinically severe, rapidly progressing disease and excessive amounts of bone loss must be thoroughly assessed.
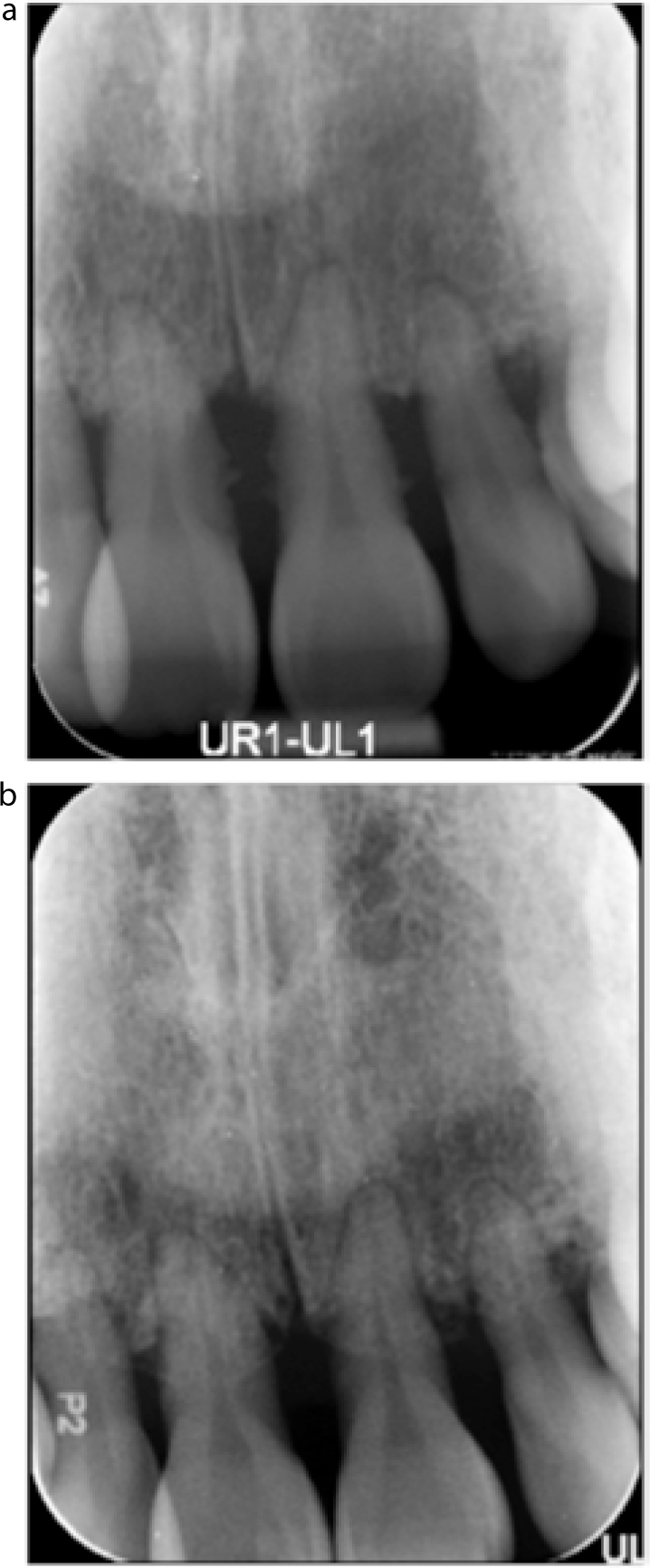
Both localized and generalized cases of aggressive periodontitis have been reported, mostly in patients with Down's syndrome, however, other groups may also be affected (Figure 1).25,27,28,30
Figure 1.
(a, b) Two cases of localized aggressive periodontitis mainly affecting the anterior teeth. Early loss of the central incisors is commonly seen in individuals with Down's syndrome. www.down-syndrome.org/reviews/84
In these cases, systemic antimicrobial therapy alongside full mouth debridement has been advocated (Figures 2 and 3). A combination of Amoxicillin 250 mg TDS with metronidazole 200 mg TDS for 7–10 days is the recommended regimen.30 Although the provision of treatment in these cases may not always be successful or predictable, success stories have been reported.31,32
Figure 2. OPG showing generalized aggressive periodontitis in a young autistic patient.Figure 3.
(a, b) Case of aggressive periodontitis. Pre- and post-treatment periapicals (16 months later) showing some bony healing around the UL1,2 following full mouth disinfection with antibiotic cover. Clinically, there were reductions in pocket depth and mobility following 6 months. (Reproduced by kind permission of S. Burke, StR Special Care Dentistry).
Chemical adjuncts
The regular use of chlorhexidine to help maintain good plaque control in patients with learning disabilities has produced varying results in different studies. Whilst one study reported its use twice daily for up to a year, producing overall plaque indices similar to that of baseline with no improvement, a number of others have suggested a significant benefit in subjects who cannot perform adequate mechanical plaque control.33,34 Additionally, guidelines from the British Society of Disability and Oral Health 2012 suggest chlorhexidine to be effective in reducing plaque bacteria over short periods.9 They suggest the application of chlorhexidine gel (1%) daily, along with 6-monthly professional prophylaxis to be an effective and efficient means of specifically maintaining periodontal health in Down's syndrome individuals. Additionally, chlorhexidine varnish (40%) applied 6-monthly may offer additional benefit. A prospective case series followed up over one year suggested the additional use of a chlorhexidine mouthwash twice daily in conjunction with 1% chlorhexidine gel could produce significant reductions in PPD due to the resolution of highly inflamed gingivae as well as improvements in CAL. These improvements were comparable to that gained in adults with chronic periodontitis who did not have Down's syndrome.
Splinting
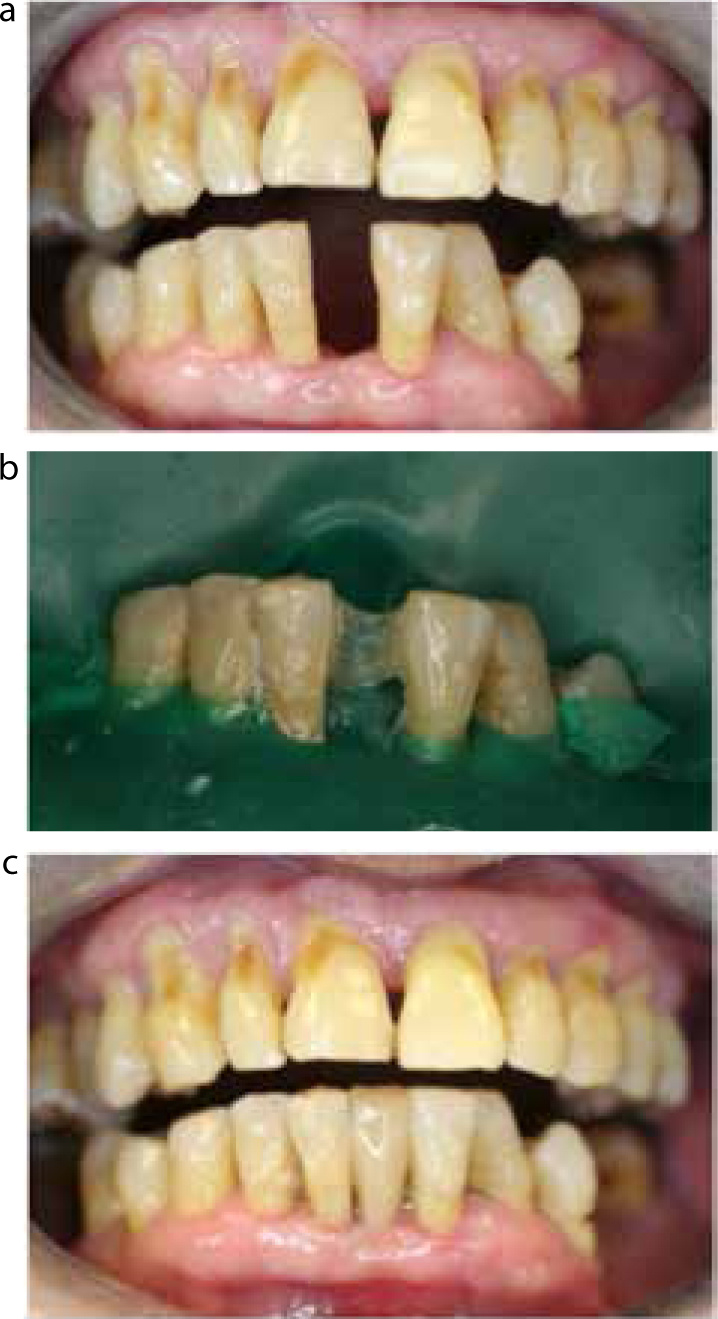
In those patients where advanced periodontal disease has led to significant mobility of the lower anterior teeth but who are otherwise asymptomatic, a periodontal splint should be considered. Fibre-reinforced composite splints are increasingly used in advanced periodontal disease cases to stabilize teeth and prevent further occlusal trauma, thus delaying extractions.35,36 Studies have demonstrated that vital mandibular teeth of grade 3 mobility, with at least one firm canine on both sides, can be splinted together successfully with fibre-reinforced composites for up to 4.5 years, resulting in reductions in PPD and CAL.37,25 If lower incisors have been lost prematurely, a conventional resin-bonded bridge from canine to canine can be used for replacement. Alternatively, a fibre-reinforced composite bridge using either the crown of the natural tooth, a denture tooth or a direct composite build-up technique can be successful (Figure 4).
Figure 4.
(a–c) Patient with past history of active periodontal disease. The LL1 had exfoliated and was built up using direct composite on a fibre-reinforced composite splint.
Treatment under general anaesthesia
Those patients who can only be treated under general anaesthesia present a significant problem to the treating clinician. Dougherty stated that ‘while some practitioners may feel that it is in the patient's best interests to undertake an examination and preventive treatment under GA as regularly as annually, others may feel it is only appropriate when there is obvious pathology requiring treatment.’38 Carrying out research to answer this question is not feasible and it remains within the dentist's discretion to make a balanced judgement depending on the patient's medical risk, dental risk factors for caries and periodontal disease and the opinion of the patient's supporting network where the patient lacks capacity. A large majority of those requiring GA tend to have more severe learning disabilities. Whilst treatment was not carried out under GA, and was in a cohort of Down's syndrome patients who are significantly more treatment resistant. Cichon et al and Hanookai et al saw no improvement in clinical and microbiological parameters following a single session of scaling and root planing.39,40 In comparison, Moosani et al suggested that even patients with persistently poor oral hygiene and recall intervals in excess of 9 months would still benefit from a single session of scaling and root planing under general anaesthesia. They reported a direct benefit in reducing the oral inflammatory load for an extended period of time with a reduction in the rate of attachment loss.41
The method used relied on attaining oral swabs from the patient's gingivae under GA and at subsequent post GA recall. These swabs underwent laboratory detection of myeloperoxidases, an enzyme released from polymorphonuclear leukocytes which are present in high quantities during inflammatory responses. Using a colorimetric-based reaction, the oral inflammatory load was detected. Challenges of the study included obtaining a reliable sample at recall due to poor patient co-operation and accounting for a colorimetric reaction that was not affected by other salivary peroxidases. Further research on this potentially new method of periodontal diagnosis as well as the conclusions drawn would be very beneficial.
Conclusions
The requirement for dental professionals to assist patients with learning disabilities in the removal of plaque and plaque retentive factors is significant. For the most part, removal of the soft plaque biofilm needs to be focused on at appropriate recall intervals for the patient, ideally by full mouth ultrasonic scaling, or gentle hand scaling/toothbrushing where the ultrasonic is not tolerated. As a large proportion of these patients are likely to require treatment under compromised sedation conditions or time intensive general anaesthetia, more detailed, precise periodontal measurements may not always be appropriate or even necessary. A BPE can assist the clinician in producing an approximate diagnosis of severity and help decide whether additional chemical or antimicrobial adjuncts are required.
Those able to tolerate treatment with behavioural management alone or under good sedation conditions may benefit from more detailed indicators of disease as a monitoring tool for improvement.
Despite the presence of poor oral hygiene in a large majority of these patients, evidence indicates that full mouth debridement can significantly benefit individuals by reducing the oral inflammatory load, although this would need further research. Given the increasing correlation between inflammatory oral and systemic disease, a reduced oral inflammatory load can act as a significant preventive mechanism to systemic disease elsewhere in the body, thus potentially reducing morbidity and, in certain cases, even mortality.
When considering the periodontal treatment of patients with learning disabilities, the three key elements of prevention, risk factor control and professional mechanical intervention must always be considered. As discussed in part 1, prevention and risk factor control requires an individualized, systematic and continuous reinforcement approach that may involve other medical and social professionals as well as the patient's family and carers.
Recall intervals must be made on a patient specific basis with more regular recalls having the potential to reinforce preventive advice and encourage behaviour change, reduce the inflammatory load further, as well as help patient acclimatization.