Burke FJT. Amalgam to tooth-coloured materials – implications for clinical practice and dental education: governmental restrictions and amalgam-usage survey results. J Dent. 2004; 32:343-350
Green DJB, Banerjee A. Contemporary adhesive bonding: bridging the gap between research and clinical practice. Dent Update. 2011; 38:439-450
Burke FJT. What's new in dentine bonding? Self-etch adhesives. Dent Update. 2004; 31:580-589
Green DJB, Mackenzie L, Banerjee A. Minimally invasive long-term management of direct restorations: the ‘5 Rs’. Dent Update. 2015; 42:413-420
Burke FJT. Dentine bonding agents – optimizing the use of composite materials. Dent Update. 1991; 18:96-104
Burke FJT. Dentine adhesives: the current status. Dent Update. 1987; 14:201-211
Burke FJT, McCaughey AD. The four generations of dentine bonding. Am J Dent. 1995; 8:88-92
Van Meerbeck B, Yoshihara K, Yoshida Y, Mine A, De Munck J, Van Landuyt KL. State of the art of self-etch adhesives. Dent Mater. 2011; 27:17-28
Combe EC, Burke FJT, Douglas W.Chicago: Kluwer; 1999
Buonocore MG A simple method of increasing the adhesion of acryl filling materials to enamel surfaces. J Dent Res. 1955; 34:849-853
Peumans M, De Munck J, Van Landuyt K, Lambrehts P, Van Meerbeck B. Three year clinical effectiveness of a two step self-etch adhesive in cervical lesions. Eur J Oral Sci. 2005; 113:1-7
Peumans M, De Munck J, Van Landuyt K, Poitevin A, Lambrehts P, Van Meerbeck B. Eight year clinical evaluation of a 2-step self-etch adhesive with and without selective enamel etching. Dent Mater. 2010; 26:1176-1184
Helvey G. Adhesive dentistry: the development of immediate dentin sealing/selective etching bonding technique. Compend Contin Educ Dent. 2011; 32:22-35
Burke FJT, Crisp RJ, Cowan AJ, Raybould L, Redfearn P, Sands P, Thompson O, Rivaghi V. A randomised controlled trial of a Universal bonding agent at three years: Self etch vs Total etch. Paper submitted for Editorial Consideration, EJPRD.
Peumans M, De Munck J, Van Landuyt K, Van Meerbeck B. Thirteen-year randomised controlled clinical trial of a two-step self-etch adhesive in non-carious cervical lesions. Dent Mater. 2015; 31:308-314
Van Landuyt KL, Yoshida Y, Hirata I, Snauwaert J, De Munck J, Okazaki M, Suzuki K, Lambrehts P, Van Meerbeck B. Influence of the chemical structure of functional monomers on their adhesive performance. J Dent Res. 2008; 87:757-761
Fundingsland JW, Aasen SM, Bodger PD The effect of high humidity on adhesion to dentine. J Dent Res. 1992; 72:(Spec Issue)
Nakabayashi N, Masuhara E, Mochida E, Ohmori I. Development of adhesive pit and fissure sealants using MMA resin initiated by a tri-n-butyl borane derivative. J Biomed Mater Res. 1978; 12:149-165
Kim RJ, Woo J-S, Yi Y-A, Hwang J-Y, Seo D-G. Performance of Universal adhesives on bonding to leucite-reinforced ceramic. Biomat Res. 2015; 19:11-16
Kalavacharla VK, Lawson NC, Ramp LC, Burgess JO. Influence of etching protocol and silane treatment with a Universal adhesive on lithium disilicate bond strength. Oper Dent. 2015; 40:372-378
Vogl V, Hiller KA, Buchalla W, Federlin M, Schmalz G. Controlled, prospective, randomized, clinical split mouth evaluation of partial ceramic crowns luted with a new, Universal adhesive system/resin cement: results after 18 Months. Clin Oral Invest. 2016; 20:2481-2492
Muñoz MA, Sezinando A, Luque-Martinez I, Szesz AL, Reis A, Loguercio AD, Bombarda NH, Perdigao J. Influence of a hydrophobic resin coating on the bonding efficacy of three universal adhesives. J Dent. 2014; 42:595-602
Lawson NC, Robles A, Fu C-C, Lin CP, Swalani K, Burgess JO. Two-year clinical trial of a universal adhesive in total-etch and self-etch mode in non-carious cervical lesions. J Dent. 2015; 43:1229-1234
Ferracane JL. Resin-based composite performance: are there some things that we can't predict?. Dent Mater. 2013; 29:51-58
Bayne SC. Correlation of clinical performance with “in vitro tests” of restorative dental materials that use polymer-based matrices. Dent Mater. 2012; 28:52-71
Burke FJT, Hussain A, Nolan L, Fleming GJP. Methods used in dentine bond strength tests: an analysis of 102 investigations on bond strength. Eur J Prosthodont Rest Dent. 2008; 16:158-165
Loguericio AD, Muñoz MA, Martinez IL, Hass V, Reis A, Perdigao J. Does active application of Universal adhesives to enamel in self-etch mode improve their performance?. J Dent. 2015; 43:1060-1070
Rosa WL, Piva E, Silva AF. Bond strength of Universal adhesives: a systematic review and meta-analysis. J Dent. 2015; 43:765-776
Muñoz M, Luque-Martinez I, Malaquias P, Hass V, Reis A, Campanha NH, Loguercio AD. In vitro longevity of bonding properties of Universal adhesives to dentin. Oper Dent. 2015; 40:282-292
Chen C, Niu LN, Xie H, Zhang ZY, Zhou LQ, Jiao K, Chen JH, Pashley DH, Tay FR. Bonding of Universal adhesives to dentine – old wine in new bottles?. J Dent. 2015; 43:525-536
Cardenas AM, Siqueira F, Rocha J, Szesz AL, Anwar M, El-Askary F, Reis A, Loguercio A. Influence of conditioning time of Universal adhesives on adhesive properties and enamel-etching pattern. Oper Dent. 2016; 41:481-490
Takamizawa T, Barkmeier WW, Tsujimoto A, Berry TP, Watanabe H, Erickson RL, Latta MA, Miyazaki M. Influence of different etching modes on bond strength and fatigue strength to dentin using Universal adhesive systems. Dent Mater. 2016; 32:e9-e21
Thanaratikul B, Santiwong B, Harnirattisai C. Self-etch or etch- and-rinse mode did not affect the microshear bond strength of a Universal adhesive to primary dentin. Dent Mater J. 2016; 35:174-179
Saikaew P, Chowdhury AFMA, Fukayama M, Kakuda S, Carvalho RM, Sano H. The effect of dentine surface preparation and reduced application time of adhesive on bond strength. J Dent. 2016; 47:63-70
Loguericio AD, de Paula EA, Hass V, Luque-Martinez I, Reis A, Perdigao J. A new universal simplified adhesive: 36-month randomized double-blind clinical trial. J Dent. 2015; 43:1083-1092
Perdigão J, Kose C, MenaSerrano AP, De Paula EA, Tay LY, Resi A, Loguercio AD. A new Universal simplified adhesive: 18-month clinical evaluation. Oper Dent. 2014; 39:113-127
Lawson NC, Robles A, Fu C-C, Lin CP, Sawlani K, Burges JO. Two-year clinical trial of a universal adhesive in total-etch and self-etch mode in non-carious cervical lesions. J Dent. 2015; 43:1229-1234
Brunton PA, Burke FJT, Sharif MO, Creanor S, Hosey MT, Mannocci F, Wilson NHF. Contemporary dental practice in the UK in 2008: aspects of direct restorations, endodontics and bleaching. Br Dent J. 2012; 212:63-67
The ability to bond restorations to dentine successfully is central to minimally invasive restorative dentistry. While dentine-bonding agents have gone through a variety of ‘generations’, it is the purpose of this paper to describe the latest dentine-bonding agents, the Universal Bonding Agents. These materials may be considered ‘Universal’ insofar as they may be considered to be capable of being used for direct and indirect dentistry, as well as being suitable for use in whichever etching modality the clinician considers appropriate, namely self-etch, etch and rinse or selective enamel etch. Laboratory investigations and initial clinical studies hold the promise that Universal Bonding Agents are a forward step in the quest for the ultimate bond to tooth substance.
CPD/Clinical Relevance: New Universal Bonding Agents appear to present a promising advance in bonding to dentine.
Article
Dentine-bonding agents play a strategic role in the sealing and retention (where necessary) of resin composite restorations, which are increasingly placed by dentists worldwide.1 Bonding to dentine is also central to the practice of minimally invasive dentistry, given that bonded restorations do not require macro-mechanical retentive features such as locks and keys, which are a feature of non-adhesive (amalgam) cavity preparations.2
A dentine-bonding agent should perform the following functions:3
Provide a strong, immediate and permanent bond to dentine;
Seal the cavity and minimize leakage;
Resist microbial or enzymatic degradation;
Provide adhesion per se of the restoration in cases where this is necessary;
Prevent post-operative sensitivity;
Reduce the risk of recurrent caries;
Prevent marginal staining;
Be easy to use.
It is the intention of this paper to update readers on the new group of Universal Dentine-Bonding Agents, this being a follow-up to a paper published in 2004 giving details of the last major innovation in bonding to dentine, the introduction of the so-called self-adhesive dentine-bonding agents3 and to other Dental Update publications on the subject which readers may wish to read as background or a further update, such as those by Green and Banerjee,2 Green, Mackenzie and Banerjee4 and others.5,6
A brief history of bonding to dentine
In the past, dentine-bonding agents were classified into generations.7 However, this means of identifying different groups of bonding agents fell into disarray because of the failure of authorities on the subject to agree on the type of bonding agent which fitted a given ‘generation’. Until recently, the classification has therefore been simply, glass-ionomer materials, and resin-based dentine-bonding agents, the latter being further classified into etch and rinse materials and self-etch materials, with some workers classifying the self-etch materials according to their pH.8
There are two principal means by which a bond to dentine may be achieved:9
First, glass-ionomer materials (GIC – glass-ionomer cements) which were developed in the 1970s, initially being derived from the Fluoro-Alumino-Silicate glass used in the silicate cement materials which were used until the 1960s, but with the phosphoric acid used in silicate cements being substituted by a polyacrylic acid. GICs were found to have a number of benefits, such as their ability to form a self-adhesive, reliable bond to dentine and the potential to release fluoride initially, but suffered from poor aesthetics and low flexural strength.9
Second, since the ability to bond to enamel was first described by Buonocore in 1955,10 bonding to tooth structure has become an essential part of restorative dentistry and has facilitated the development of resin composite materials, with these materials becoming increasingly used worldwide,1 principally because of patient concerns regarding mercury in dental amalgam and the poor appearance of such amalgam restorations, alongside patient desires to receive aesthetic restorations in both their anterior and posterior teeth. However, dentine is a vital substrate with circa 20% organic and 10% water by weight, and these factors make bonding to dentine more challenging than to enamel. Early resin-based dentine-bonding agents were little more than wetting agents which penetrated the smear layer, until it was realized that the smear layer was not well attached to the underlying dentine. This realization facilitated the development of two distinct types of resin-based dentine-bonding agent:
The etch and rinse (or total etch) materials in which the smear layer was dissolved away by the application of 30–35% phosphoric acid, followed by washing and drying, and the application of the bonding agent. These materials, with a four-stage clinical application protocol, could be considered technique sensitive because of the risk of a failure to carry out any stage optimally,3 hence the development of the self-etch dentine-bonding agents.
In the so-called self-etch bonding systems, the bonding resin is combined with an acid (generally phosphoric acid) in order to reduce the pH to a level which is said to be sufficiently low to carry out the etching step at the same time as the bonding. These materials were therefore significantly simpler to use than the etch and rinse materials and could be presented in only one bottle, thereby facilitating their use. An example of these is G Bond from GC, this being one of the few materials to achieve a maximum score of 5 out of 5 for ease of use since the practice-based research group, the PREP Panel, commenced its ‘handling evaluations’ in 1993.11
Results of research from Leuven12 involving the clinical use of the self-etch adhesive Clearfil SE (Kuraray) in 100 non-retentive Class V cavities (these being considered to be the ultimate test of adhesives as there is no macro-mechanical retention, being reliant only on the bonding agent to retain the restoration) have indicated the need to etch the enamel selectively with phosphoric acid when using a self-etch dentine-bonding agent, because the enamel cavity margins indicated clinical advantages in terms of integrity and lack of staining when they were etched selectively with phosphoric acid. ‘Selective enamel etching’ is therefore a relatively new concept in restorative dentistry, with one of its first uses being in the study by Peumans and colleagues.12 When these workers extended their study to eight years,13 the results continued to indicate fewer small marginal defects on enamel in the selective enamel etch group (65% cf 44% in the non-etch group), while there was more superficial marginal discoloration in the non-etch group, with these differences being only statistically significant for marginal discoloration. In this regard, the so-called self-etch bonding agents were introduced because of dentists' requests for ease of use and speed, with this involving not using phosphoric acid. However, with the benefit of hindsight, it could be considered that clinicians were naïve to expect materials with a pH of up to 2.5 to provide similar marginal integrity or low incidence/absence of marginal discoloration on enamel margins as could be obtained when these were etched using phosphoric acid (pH of 0.5), remembering that pH operates on a logarithmic scale. Hence, in this paper, the authors have termed these so-called self-etch materials in order to indicate their skepticism regarding the ability of these materials to etch the enamel margins adequately, given that it may be considered oxymoronic to use the term self-etch when it appears that etching of enamel with phosphoric acid is indeed necessary if long-lasting good quality restoration margins are to be produced.
Universal Bonding Agents
With a traditional so-called self-etch bonding agent, a principal problem was that they are relatively mild in their acidity, with pH values of between 2 and 2.5. This provides a near ideal treatment of dentine but does not adequately etch enamel. In that regard, a bond to enamel is essential in order to provide marginal seal for the restoration and is the first form of defence against microleakage. For this reason, total etch systems have, up to now, been considered gold standard.14
However, the so-called self-etch dentine-bonding agents had a number of advantages when compared to etch and rinse types, namely:3
No post-conditioning rinsing, hence less operator sensitive;
Less sensitive to the degree of wetness/dryness of the dentine surface;
Single unit dose packaging possible, hence reduced risk of cross infection;
Consistent and stable composition;
Simultaneous demineralization and resin-infiltration meant that it was not possible to over etch the dentine, leading to reduced levels of post-operative sensitivity.
However, among the disadvantages listed in 20043 was: ‘adhesion to enamel requires further long-term evaluation in some systems’. In that regard, it was therefore likely that, as a result of the recently perceived need to etch the enamel margins when using so-called self-etch adhesives, a new group of bonding agents, the Universal Bonding Agents, have been introduced.
A Universal Bonding Agent may be defined as one which:15
Is capable of being used in whichever etching mode that the operator considers appropriate (total etch, self-etch or selective enamel etch): the authors of this paper consider that selective enamel etching is appropriate, as will be demonstrated when the results of recent research are discussed later in this paper;
May be used for direct and indirect dentistry, the latter generally in conjunction with a resin-based luting system from the same manufacturer as the bonding agent, with the luting system incorporating a material-specific initiator.
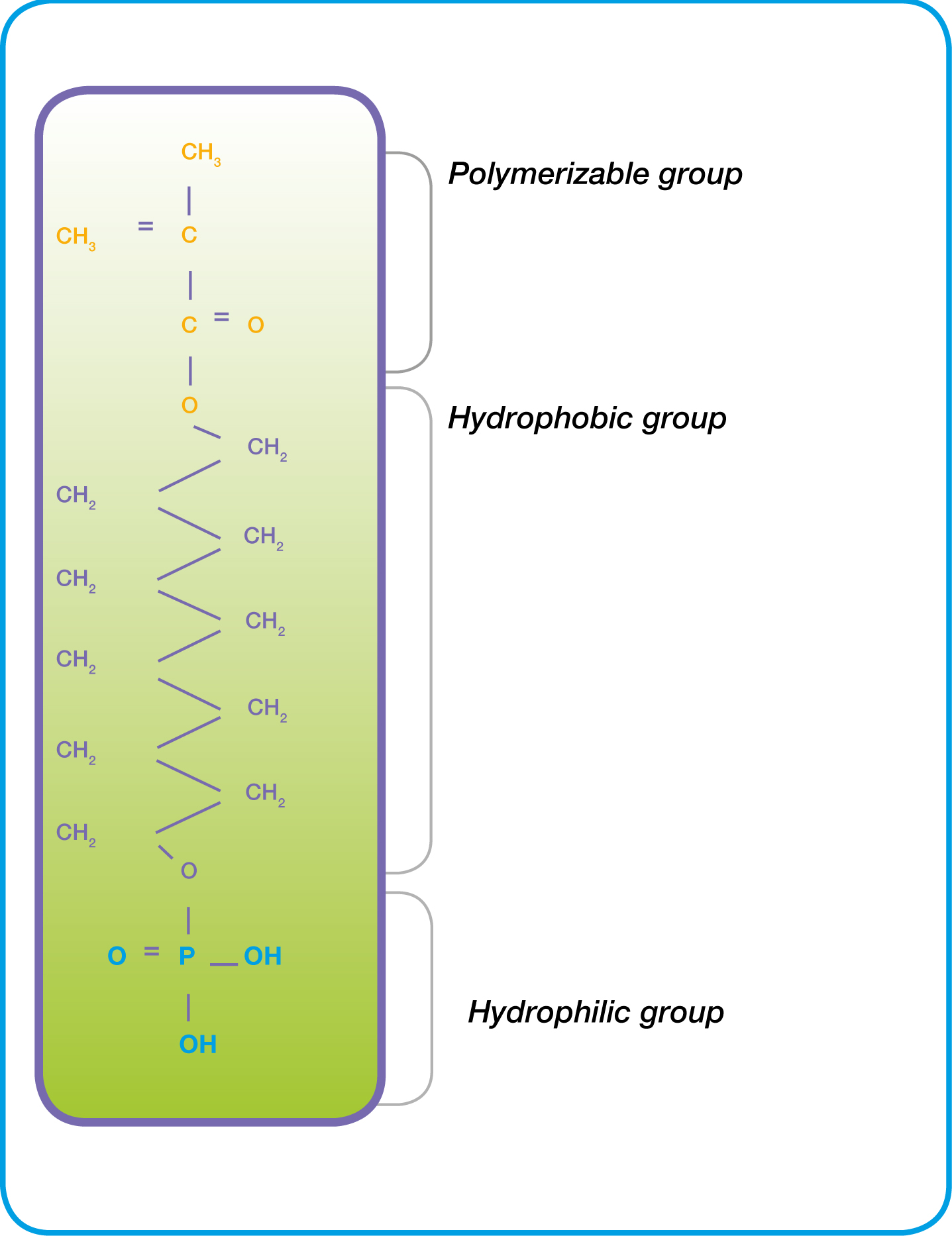
Another factor that the majority of this new group of bonding agents have in common is the resin methacryloyloxydecyl dihydrogen phosphate (10-MDP).16 10-MDP has been shown to provide good clinical survival rates in surveys of Class V restorations, with data using Clearfil SE Bond (Kuraray), which includes this resin, now being available at 13 years.17 10-MDP (Figure 1) was originally developed by Kuraray in the 1980s, this uniquely providing not only a micromechanical bond via a hybrid layer, but also bond ionically to calcium, ie to hydroxyapatite in dentine,18 via the hydrophilic group incorporated in the molecule.
Figure 1. Chemical formula of 10-MDP (after www.Kuraray Dental/Key Technologies).
The components of some Universal Bonding Agents are presented in Table 1 and the function of their various components may be considered to be as indicated in Table 2.
BisGMA is a proven ‘backbone’ of a majority of today's resin composite materials which facilitates compatibility of hydrophilic substances such as HEMA and hydrophobic resins and imparts high mechanical strength.9
10-MDP makes a bonding agent acidic and is a functional monomer which forms a strong chemical bond to hydroxyapatite surfaces, ie promotes adhesion to tooth substance by formation of insoluble MDP-Ca2+ salts18 and providing high mechanical strength.
Vitrebond copolymer has been a constituent of 3M bonding agents since 1993, it being a methacrylate-modified polyalkenoic acid copolymer. It provides for moisture tolerant performance to dentine as it is resistant to changes in the humidity of the dentine surface.19
HEMA promotes wetting of surfaces and assists in penetration of dentinal tubules.
D3MA is a hydrophobic dimethacylate which enables the reaction of the adhesive with other monomers in the restorative composite or luting material.
4-META, originally described by Nakabayashi et al20 faciliates a bond to hydroxyapatite, but will also bond to metal surfaces.
Urethane dimethacrylate (UDMA) fulfils a similar function to BisGMA.
Camphorquinone is an initiator which is sensitive to blue light at 460 nanometers.
Ethanol, acetone and water are solvents.
Although the similarities between the Universal Bonding Agents in Table 1 and Optibond XTR relate only to their respective clinical applications as opposed to their chemical formulation, it could be argued that Optibond XTR should also be considered as a Universal Bonding Agent, even though it does not contain 10-MDP. It is a 2-component, light-cured, 15% filled, bonding agent, which the manufacturers (Kerr Mfg Co, Orange CA, USA) suggest is indicated for direct and indirect restorative procedures. Its chemistry is derived from previous Kerr bonding agents, using the monomer GPDM, and contains a separate hydrophilic primer, along with a separate hydrophobic adhesive to maximize material compatibility. It contains three solvents, water, ethanol and acetone: as two of these evaporate, the pH reduces from 2.4 to 1.7, which the manufacturers suggest is sufficiently low as not to require selective enamel etching. It also contains camphorquinone and stabilizer.21 In terms of true universality, it is capable of being used for indirect restorations, in conjunction with the appropriate Kerr resin luting material.
So, just how good are these new Universal adhesives?
As with any recently-introduced material, there is a relative paucity of evidence relating to these new materials, although this is building with respect to Scotchbond™ Universal Adhesive (SBU) (3M, St Paul, USA), given that it was the first of this group of Universal materials to be released commercially. Regarding SBU (3M), this is classified as ‘ultra-mild’:22 it also contains a polyalkenoic acid copolymer known as Vitrebond copolymer as well as a silane which may facilitate a bond to ceramic.23 When used for indirect dentistry, the manufacturers advise that further silanating prior to bonding is not required to pre-treat a porcelain restoration. However, stronger bond strengths have still been reported with a separate treatment of silane.24,25 As this is carried out at the chairside (ie outside the mouth) and is a simple task to perform, this may not be considered to be of great consequence. In this regard, when a Universal Bonding Agent was used in conjunction with the luting system from the same manufacturer, performance has been reported, by Vogl and co-workers26 who used a split-mouth randomized study design, to be suitable for the clinical task for which they are intended, with SBU and Rely X™ Ultimate (3M, St Paul, USA) demonstrating consistent results at 18 months and with the authors stating that this combination may be recommended for luting partial ceramic crowns.
Scotchbond™ Universal (3M) is the only Universal Bonding Agent to contain both 10-MDP and Vitrebond copolymer (3M). However, in a study by Muñoz et al,27 Scotchbond™ Universal performed suboptimally and one suggested potential mechanism for failure was that the two molecules (10-MDP and Vitrebond Copolymer) could have been competing to bond with calcium and therefore potentially cancelling each other out.27 This evidence is not supported elsewhere in the literature and the performance of SBU has been reported to be comparable with the ‘gold standard’ two-bottle self-etch adhesives in non-carious cervical lesions.28 It is early days, but bonding of restorations with SBU in conjunction with Rely X™ Ultimate (3M) appears to be providing promising results.26
It is considered by the authors that there are a number of useful and relevant clinical and laboratory studies worth mentioning. In this regard, clinical studies may be considered superior, since Ferracane, and Bayne, two of the world's leading dental materials scientists, have independently come to the conclusion that there is little correlation between laboratory studies and clinical performance of materials.29,30 Care therefore must be taken when interpreting laboratory-based studies – there is evidence to be gained from in vitro studies but it should be used with caution. Nevertheless, laboratory studies may be of some value as they may provide an early assessment of the different variables which may affect the performance of a given material, but the studies should be selected with care.31
Laboratory studies
In an extensive laboratory study on Universal Bonding Agents, Loguerico and co-workers,32 using microshear bond strength testing, concluded that selective enamel etching with phosphoric acid might not be crucial for their adhesion to enamel and that ‘the application of such adhesives in self-etch mode may be a practical alternative to enamel etching in specific clinical situations’.
On the other hand, da Rosa and co-workers,33 in a systematic review and meta-analysis, considered that the enamel bond strength of Universal adhesives was improved with prior phosphoric acid etching.
Muñoz and co-workers34 carried out an extensive laboratory assessment which compared the microtensile bond strength of three Universal adhesives: All-Bond™ Universal (Bisco, Schaumburg, USA), G-Bond Plus™ (GC Corporation, Tokyo, Japan) and Scotchbond™ Universal (3M) in etch and rinse and self-etch modes and using Heliobond™ (Ivoclar Vivadent, Liechtenstein) as control. In addition, these workers applied an additional layer of hydrophobic resin over the polymerized adhesive in some groups. Their results indicated that this layer improved the performance of the resins, that SBU (3M) performed similarly in self-etch and etch and rinse modes, with the authors going on to discuss that it could be the presence of 10-MDP as well as Vitrebond™ Copolymer in the Scotchbond™ Universal (3M) which results in this performance, given the improved adhesive performance reported.34
Chen and co-workers35 carried out an extensive laboratory evaluation of five Universal Bonding agents [Prime & Bond Elect® (Dentsply), Scotchbond™ Universal (3M), All-Bond Universal™ (Bisco Inc), Clearfil™ Universal (Kuraray), Futurabond U (VOCO)] using two bonding modes (etch and rinse and self-etch) for microtensile bond strength testing and electron microscopy, having thermocycled 50% of the specimens. When bonded to dentine, the adhesives performed differently in the shear bond testing and the etching mode did not make a difference to the results. The authors praise the increased versatility of the materials which they tested but, by entitling the paper ‘Old wine in new bottles’, they imply that there is nothing new in the adhesive molecules employed, further stating that the manufacturers are using techniques akin to the mixing of cocktails by skilled bartenders! However, when previous bonding resins were classified as etch and rinse or, so-called self-etch, it was not possible to use a self-etch type of bonding agent with an etch and rinse approach, or vice versa. By contrast, it appears, from the results of the research by Chen et al,35 that the Universal approach of etching in whatever mode the clinician identifies as correct, is actually possible with these Universal Bonding Agents. In that regard, the authors express surprise that ‘it is inexplicable why bonds created by Scotchbond™ Universal in the etch and rinse mode were relatively stable’.
Cardenas and colleagues36 used resin-enamel microshear testing to test three Universal adhesives [SBU (3M), All-Bond Universal™ (Bisco Inc), Futurabond U (VOCO, Cuxhaven, Germany)] in self-etch and etch and rinse modes at application times of 20 seconds and 40 seconds, also agitating the resin on the dentine surface by using manual pressure of 35g on a microbrush. The results indicated improved degree of conversion of the resins at 40 seconds when applied in self-etch mode, with the authors adding that the acidity of the Universal Bonding Agents tested did not have sufficient acidity to produce retentive etching patterns on enamel equivalent to those produced by 35% phosphoric acid, with the authors concluding that ‘active and prolonged application of universal adhesives in the self-etch mode may be a viable alternative to increase the enamel etching pattern and resin-enamel bond strength’.
Takamizawa and co-workers37 used fatigue testing to evaluate the dentine-bonding ability of three Universal Bonding Agents in total-etch and self-etch modes. Their results indicated that Prime and Bond Elect® (Dentsply: Milford DE, USA) performed better in total etch mode, whereas SBU (3M) and All-Bond Universal™ (Bisco Inc, Schaumburg, IL, USA) did not show a difference in performance in either etching mode.
Thanaratikul and colleagues38 from Thailand tested the microshear bond strength of three adhesives to primary dentine, concluding that SBU (3M) resulted in similar bond strength whether it was used in self-etch mode or etch and rinse mode.
Finally, Saikaew and co-workers39 evaluated the effects of dentine surface preparation and reduced application times on microtensile bond strength, using three Universal Bonding Agents [SBU (3M), G-Premio Bond™ (GC, Tokyo, Japan) and Clearfil™ Universal (Kuraray)]. The results demonstrated that clinical methods of preparing dentine (ie with a bur) produce lower bond strengths than when the dentine is treated using SiC paper (as in laboratory studies) and that shortened application times (always a temptation for the clinician!) produced a reduced bond strength. The clinical message being, follow the manufacturers' instructions and do not be tempted to cut corners!
A further message which may be applied in the clinic is that there appears to be little difference in bonding performance for many Universal Bonding Agents, but that Scotchbond™ Universal, in particular, has had more testing than other Universal Bonding Agents, whether the dentine is etched or not: therefore, why bother etching the dentine when there is a potential for setting up post-operative sensitivity?
Clinical studies
In a clinical evaluation of 134 restorations at three years, Loguerico and colleagues40 evaluated the restorations, using FDI criteria, bonded using SBU in four etching modalities, concluding that there was no statistical difference among bonding strategies, but adding that there were signs of degradation when the adhesive was applied in self-etch mode.
Perdigão and colleagues41 placed 200 Class V resin composite restorations using SBU (3M), using four different etching modes. Five restorations were lost after 18 months. Regarding marginal adaptation, self-etch (ie no etching) resulted in significantly more restorations with more than 30% of their margins showing marginal discrepancy in comparison with the other groups in which the enamel cavity margins were etched, a clear message supporting the etching of enamel margins when using SBU.
A further clinical evaluation, by Lawson et al42, of SBU (3M) compared the clinical use of this material in self-etch or total-etch modes in 42 Class V cavities. These researchers used Scotchbond™ Multipurpose (3M) as control, recalling 38 restorations at two years. The results indicated 100% retention for the total-etch group and the loss of five restorations in the self-etch group. Marginal discoloration increased over time in all groups, but restorations placed using SBU in self-etch mode exhibited greater marginal staining and the SBU total-etch restorations received the most ‘perfect’ ratings. However, the downside was that the ‘sensitivity to cold’ score in the total-etch group was marginally higher than the others. Nevertheless, in light of the findings of Lawson et al,42 and the increased sensitivity in the total etch group, the present authors consider that selective enamel etching is worthy of consideration.
The laboratory work of Loguerico and co-workers32 and Muñoz and co-workers,34 described above, could be considered to be in agreement with unpublished clinical research by Burke and colleagues,15 who used a split mouth design study to assess SBU (3M) in self-etch mode (ie no etching with phosphoric acid) against total-etch mode (all surfaces in the cavity etched with phosphoric acid), with the results, when 45 restorations were evaluated at three years, indicating no difference in the quality of the margins.15 There is, therefore, a body of opinion which indicates that selective etching of the enamel when using SBU might not be essential, but it is the authors' view that it makes sense, if the clinician wishes to achieve unstained, perfect margins over a period of time, to etch the enamel selectively. Does that statement apply to all Universal Bonding Agents? It is the authors' view that, in view of the similarities between many of the Universal Bonding Agents, and the fact that their pH values tend to lie between 2 and 3 that, until the need to etch the enamel selectively is proven by a voluminous body of opinion not to be necessary, it is prudent to suggest that this is carried out if the clinician wishes to achieve stain-free margins over a period of time.
Finally, with regard to the clinical use of Universal Bonding Agents, it is worth adding that, while isolation with rubber dam is optimal (although not universally used43) and moisture control (by whatever means) is essential, it may be considered that a further advantage is the reduced number of steps, and concomitant reduced technique sensitivity, of these new adhesive systems.
If bonding is as good as this, what are the clinical applications?
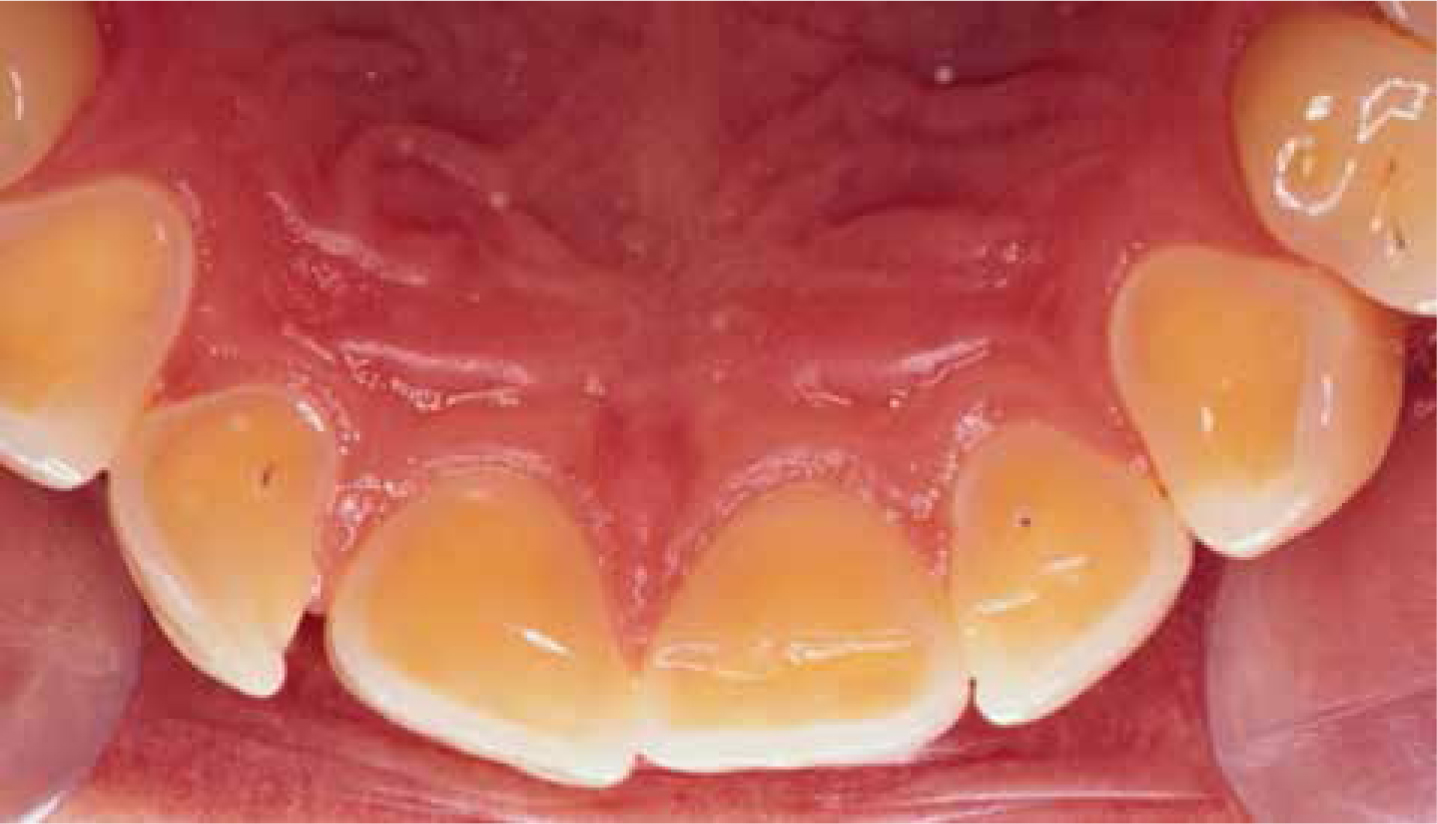
Figures 2 to 9 present a variety of the clinical applications for today's Universal Bonding Agents.
Figure 2. Dentine exposed on the palatal surfaces of a 40-year-old patient who had previously suffered from bulimia.Figure 3. Filtek™ Supreme XTE restorations bonded to the palatal dentine surfaces of UL123, UR123 of the patient in Figure 2, using Scotchbond Universal (3M).Figure 4. Labial view of patient in Figures 2 and 3, showing the incisal edges also restored, although the bonding to the incisal edges will be a mixture of enamel and dentine bonding.Figure 5. Dentinal sensitivity led this 24-year-old patient to seek treatment: there were no aesthetic concerns.Figure 6. Worn dentine surfaces on the palatal of UL12, UR12 of the patient in Figure 5, restored using a dentine-bonding agent and resin composite.Figure 7. Dentine-bonding agents are required to seal the margins of resin composite restorations: application of adhesive.Figure 8. Dentine-bonding agents are required to seal the margins of resin composite restorations: adhesive application completed.Figure 9. Completed resin composite restorations in the teeth in Figure 8.
Conclusions
In summary, Universal Bonding Agents hold promise and:
Can be used in total etch, self-etch, selective enamel etch modes, depending on the clinician's choice, although the need to etch the enamel has not been demonstrated in many of the studies quoted in this review. In view of the potential to cause post-operative sensitivity as a result of (over) etching dentine, it is the authors' view that this is not necessary or desirable and that selective enamel etching is the etching method of choice.
Are compatible with direct and indirect procedures.
Can be used with self and dual cure luting materials, usually from the same manufacturer as the bonding agent as this will contain a separate activator.
Are suitable primers for silica and zirconia.
Can bond to different substrates.
However, as with any new material or technique, long-term clinical evaluations are needed to demonstrate the value of these Universal Bonding Agents adequately.
Disclaimer
The authors have no financial interest in any of the products mentioned in this article.