Latimer O. Barnum's Rubber Dam. Dental Cosmos. 1864; VI
Consensus Report of the European Society of Endodontology. Quality guidelines for endodontic treatment. Int Endod J. 2006; 39:921-930
Ahmad I. Rubber dam usage for endodontic treatment: a review. Int Endod J. 2009; 42:963-972
Ireland L. The rubber dam – its advantages and application. Tex Dent J. 1962; 80:6-15
Cochran MA, Miller CH, Sheldrake MA. The efficacy of the rubber dam as a barrier to the spread of microorganisms during dental treatment. J Am Dent Assoc. 1989; 119:141-144
Ather A, Patel B, Ruparel N, Diogenes A, Hargreaves K. Coronavirus Disease 19 (COVID-19): implications for clinical dental care. J Endod. 2020; 46:584-595
Harrel SK. Airborne spread of disease – the implications for dentistry. J Calif Dent Assoc. 2004; 32:901-906
British Dental Association. Returning to work toolkit. 2020. http://www.bda.com
Lin P-Y, Huang S-H, Chang H-J, Chi L-Y. The effect of rubber dam usage on the survival rate of teeth receiving initial root canal treatment: a nationwide population-based study. J Endod. 2014; 40:1733-1737
Wang Y, Li C, Yuan H, Wong CM Rubber dam isolation for restorative treatment in dental patients. Cochrane Database Syst Rev. 2016; 9:(9)
Ammann P, Kolb A, Lussi A, Seemann R. Influence of rubber dam on objective and subjective parameters of stress during dental treatment of children and adolescents – a randomized controlled clinical pilot study. Int J Paediatr Dent. 2013; 23:110-115
Stewardson D, McHugh E. Patients' attitudes to rubber dam. Int Endod J. 2002; 35:812-819
Whitworth J, Seccombe G, Shoker K, Steele J. Use of rubber dam and irrigant selection in UK general dental practice. Int Endod J. 2000; 33:435-441
Hill E, Rubel B. Do dental educators need to improve their approach to teaching rubber dam use?. J Dent Educ. 2008; 72:1177-1181
Bonsor S, Pearson G. A Clinical Guide to Applied Dental Materials.London: Elsevier; 2013
Rubber dam isolation is generally considered to be the optimal method of moisture control in dentistry and is taught at the majority of dental schools worldwide. Unfortunately, undergraduate training does not always translate into use in dental practice, with the majority of clinicians never using a rubber dam, even for endodontic procedures, where its use is regarded as best practice in the United Kingdom (UK) and elsewhere. The COVID-19 pandemic has increased interest in the use of rubber dam as a highly effective infection control barrier. As professional and patient experience of rubber dam isolation is extremely limited, these two papers are designed to support the practical training of clinical teams in the confident, skilful use of rubber dam, to outline its advantages and to help overcome barriers to its routine use. Part one provides an update of the latest equipment and materials for rubber dam isolation and part two provides a practical guide to rubber dam isolation techniques for endodontic and operative/restorative procedures.
CPD/Clinical Relevance: Mastering rubber dam isolation will enhance patient care and be professionally rewarding for clinical teams.
Article
Louis Mackenzie
Timing of the introduction of rubber dam to dentistry is famously precise; the first reported use was by Dr Sanford C Barnum on 15 March 1864.1 Since then, rubber dam teaching has been progressively introduced at the vast majority of dental schools worldwide. In the UK, rubber dam placement is also within the scope of practice of dental therapists and dental nurses who have received appropriate training.
Rubber dam is universally recognized as the optimal method of moisture control, and its use is considered to be best practice in the UK and internationally during endodontic treatment.2 However, the majority of clinicians never use it or use it rarely.3 Explanations for the pervasive professional reluctance to adopt the use of rubber dam are well established:
‘Probably no other technique, instrument or treatment in dentistry has been more universally accepted and advocated, and yet is so universally ignored by practising dentists. Many reasons can be given, but in most cases the fundamental cause is inadequate explanation and training in the dental schools. If any operative technique is not clearly taught and seen to be efficiently executed by the teachers, the new members of the dental profession will not use it willingly.’4
Mitigation of the risk of transmission of SARS-CoV-2 infection has renewed interest in research, advocating the use of rubber dam as an infection control barrier during aerosol and splatter generating procedures,4,5,6,7 and its routine use has been strongly recommended by the British Dental Association for this purpose:
‘Rubber dams are very effective in reducing bioaerosols and so where it is possible, it should be used when carrying out AGPs’
Rubber dam has long been recognized as the optimal infection control barrier during endodontic and restorative procedures, enabling a reduction in microorganisms in the operative field.5,6,7 Optimal rubber dam isolation in combination with high-volume aspiration, high-quality four-handed techniques and effective use of appropriate personal protective equipment, should be capable of reducing the risk of infectious disease transmission in dental surgeries close to zero. Accordingly, this paper has three main aims:
To support the practical training of clinical teams in the confident, skilful use of rubber dam isolation as a reliable method of infection control during dental procedures;
To outline the other advantages of rubber dam isolation and help clinical teams overcome barriers to its routine use;
To provide an update on the latest equipment, materials and clinical techniques for optimizing rubber dam isolation during endodontic and operative/restorative procedures.
Advantages of rubber dam isolation
While rubber dam isolation has gained increased focus during the worldwide COVID-19 pandemic, a wide range of other advantages have been cited, and include those listed in Table 1. Barriers to the routine use of rubber dam are also well documented and are listed, alongside well-recognized counterarguments from experienced users in Table 2.
Infection control, eg sterile operative field, during aerosol generating procedures
Moisture control (saliva, blood, gingival crevicular fluid)
Increased patient comfort during operative/restorative treatments, eg no debris
Reduction in treatment interruption, eg reduced need for rinsing
Possible increased restoration longevity (compared to cotton wool roll isolation)10
Reduced exposure to mercury during dental amalgam placement and removal
Reduced clinician stress/anxiety, significant reduction in pain perception by patients11
Reduced risk of successful dento-legal clinical negligence claims
Reasons Cited for not Using Rubber Dam
Counterargument/Notes
Concerns over patient acceptance
The overwhelming majority of patients prefer treatment under rubber dam12
Patient resistance
Once used, patients commonly request rubber dam for subsequent treatments12
Time required for application
<90 seconds for most clinical situationsRubber dam may be prepared in advance of patient attendance
Application difficulties
Rubber dam use becomes easy and routine after dedicated training and with experience
Financial considerations
~ £0.60 per case
Latex allergy
Use of non-latex products predominates
Loss of orientation
May be managed with multi-tooth isolation
Psychological reasons
Very occasional claustrophobia/gagging may preclude use for restorative proceduresNB: Use is considered best practice for endodontic procedures and patients should be advised accordingly1
Mucosal, hard tissue or restorative damage from retainers
Plastic retainer alternatives are available (Figure 1)Sharp points on metal retainers may be rounded using suitable rotary instruments (coarse/medium composite shaping discs are recommended)
Occlusal restorative assessment cannot be carried out with rubber dam in place
Careful pre-operative occlusal analysis (supplemented by clinical photography) and accurate restorative shaping mitigate the need for major occlusal adjustments (Figure 1)
Rubber dam and retainers complicate endodontic radiography
Specialized endodontic sensor/film holders optimize radiographic qualitySpecialized plastic universal retainers are partially radio-opaque (Figure 1)Effective use of apex locators may eliminate the need for some radiographic exposures
Lack of proper training
Educational quality, time and dedication to mastering rubber dam techniques all have a significant impact on rubber dam use as do the curricula of individual dental schools13
Technique sensitivity
Operator/team experience improves patient compliance13 and optimizes all future endodontic and restorative procedures
System of remuneration
The majority of UK Health Service dentists never use rubber dam isolation in endodontic treatment13
Sodium hypochlorite is universally recognized as the solution of choice for endodontic irrigation and its use without rubber dam isolation is indefensible. The use of alternative irrigants, eg chlorhexidine, local anaesthetic is not recommended
Clinical case example
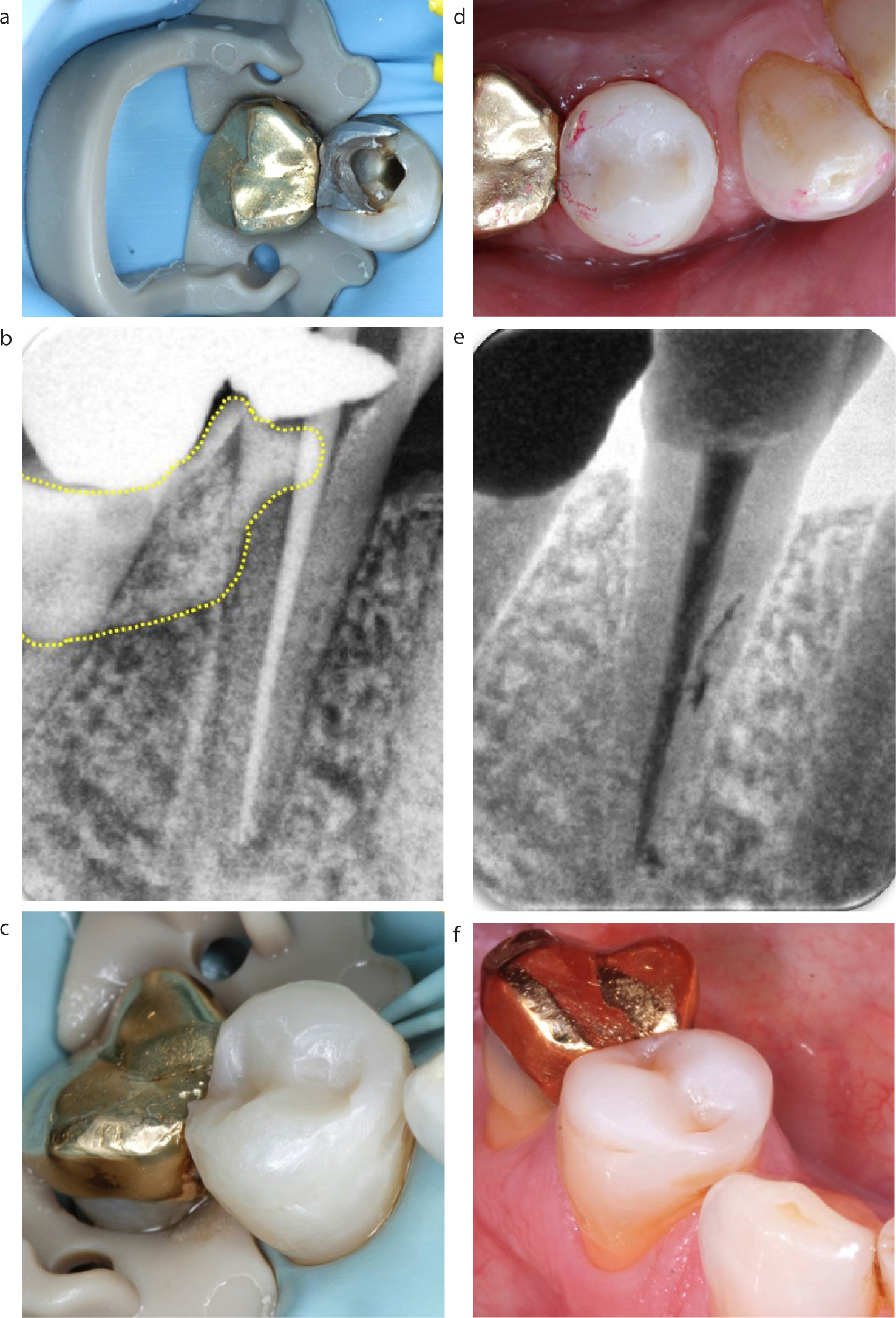
Figures 1 (a–f) illustrate the advantages of rubber dam equipment used during the endodontic and restorative treatment of a mandibular right first permanent premolar, including the following:
The universal plastic SoftClamp™ (Kerr, Bioggio, Switzerland) is suitable for all molar and premolar teeth;
Isolation optimizes safety and infection control (patient/clinical team) and improves visual and operative access;
The partially radio-opaque SoftClamp–still allows diagnostic radiographic information and still facilitates probity checks relating to dam use. (Plastic rubber dam frames also prevent radiographic ‘masking’);
Completing all endodontic and direct restorative stages in one procedure maximizes efficiency for both patient and clinical team;
Adhesion and access for resin composite placement are optimized by moisture control and soft tissue retraction;
Access for shaping, finishing and polishing procedures is more convenient and more comfortable for patients;
Accurate shaping minimizes or eliminates the need for adjustment with rotary instruments once the rubber dam is removed;
Significantly increased long-term success may be expected from endodontic and restorative procedures carried out using rubber dam isolation.7,8
Figure 1. (a) Rubber dam isolation for an endodontic/restorative procedure. (b) Radiolucent SoftClamp™retainer. (c) All adhesive and direct restorative stages completed using rubber dam. (d) Accurate shaping under dam minimizes/eliminates the need for occlusal adjustment. (e) Rubber dam isolation optimizes endodontic and adhesive/restorative outcomes. (f) Restoration at four years post-operatively.
Rubber dam training
Rubber dam training is optimized by using a two-person team approach with an unrestricted time limit to develop confidence and enable mastery of materials, equipment and clinical techniques (Figure 2). Negative reports of insufficient training may be ascribed to:
Poor initial learning experiences (in simulation and clinical settings),14 eg working alone, time limitations, lack of close supervision;
Practice limitations, eg equipment availability, time restrictions, financial limitations;
Negative word of mouth, eg rubber dam use is difficult and clinically unnecessary;
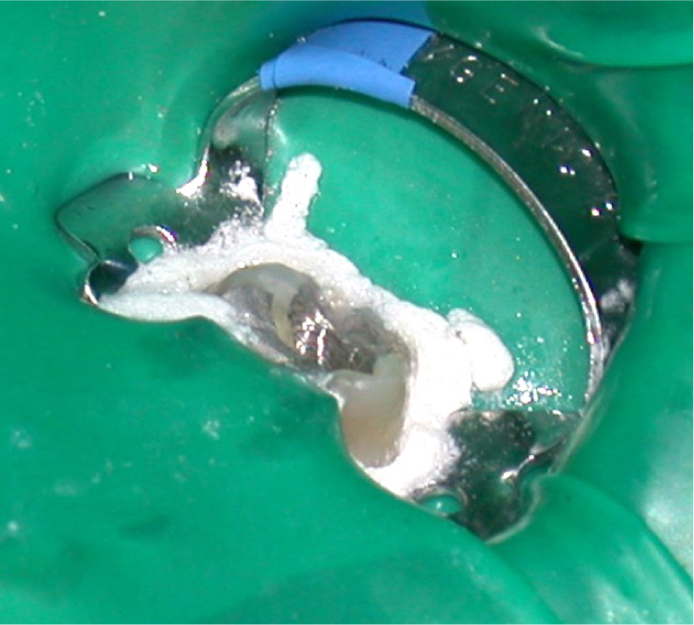
Lack of perseverance following initially discouraging outcomes (Figure 3).
Figure 2. Two-person teamwork is essential for training and mastery of rubber dam isolation techniques.Figure 3. Unsatisfactory simulation (a) and clinical (b) rubber dam isolation outcomes, after training, demonstrate suboptimal knowledge, understanding and clinical technique.
Practical guidelines for rubber dam isolation
The following practical guidelines aim to support both the training of inexperienced clinical teams and the refinement of equipment, materials and clinical techniques for clinicians who routinely employ rubber dam isolation for endodontic and restorative procedures.
Patient preparation
As most patients have never experienced dentistry carried out under a rubber dam, it is important to explain why it is being used and what to expect. The advantages listed in Table 1 may be summarized to help inform patients of the benefits of rubber dam and additional advice may include:
Reassuring patients that rubber dam helps enhance their safety and comfort during dental procedures;
Reminding the patient that they can breathe and swallow normally, that they will get no debris in their mouth, and that a saliva ejector can be placed under the rubber dam, if necessary;
Informing patients that the rubber dam retainer (avoid use of the word clamp) will prevent full closure and reminding them not to bite down firmly;
Asking patients to raise a hand if they have any concerns (usually unnecessary as patients are generally more relaxed once the rubber dam is in place);
Demonstrating the rubber dam to the patient and explaining the isolation process.
Operative site preparation
Rubber dam isolation should be planned in advance of the patient's attendance and preparation involves a number of considerations:
Occlusal contacts should be assessed, marked (and ideally photographed) prior to isolation;
Complex cavities may require a temporary foundation restoration to enable retainer placement;
Artificial undercuts may be created by temporary placement of flowable resin composite;
Anaesthetic (confirm that local or topical anaesthesia has been achieved prior to isolation).
Equipment selection
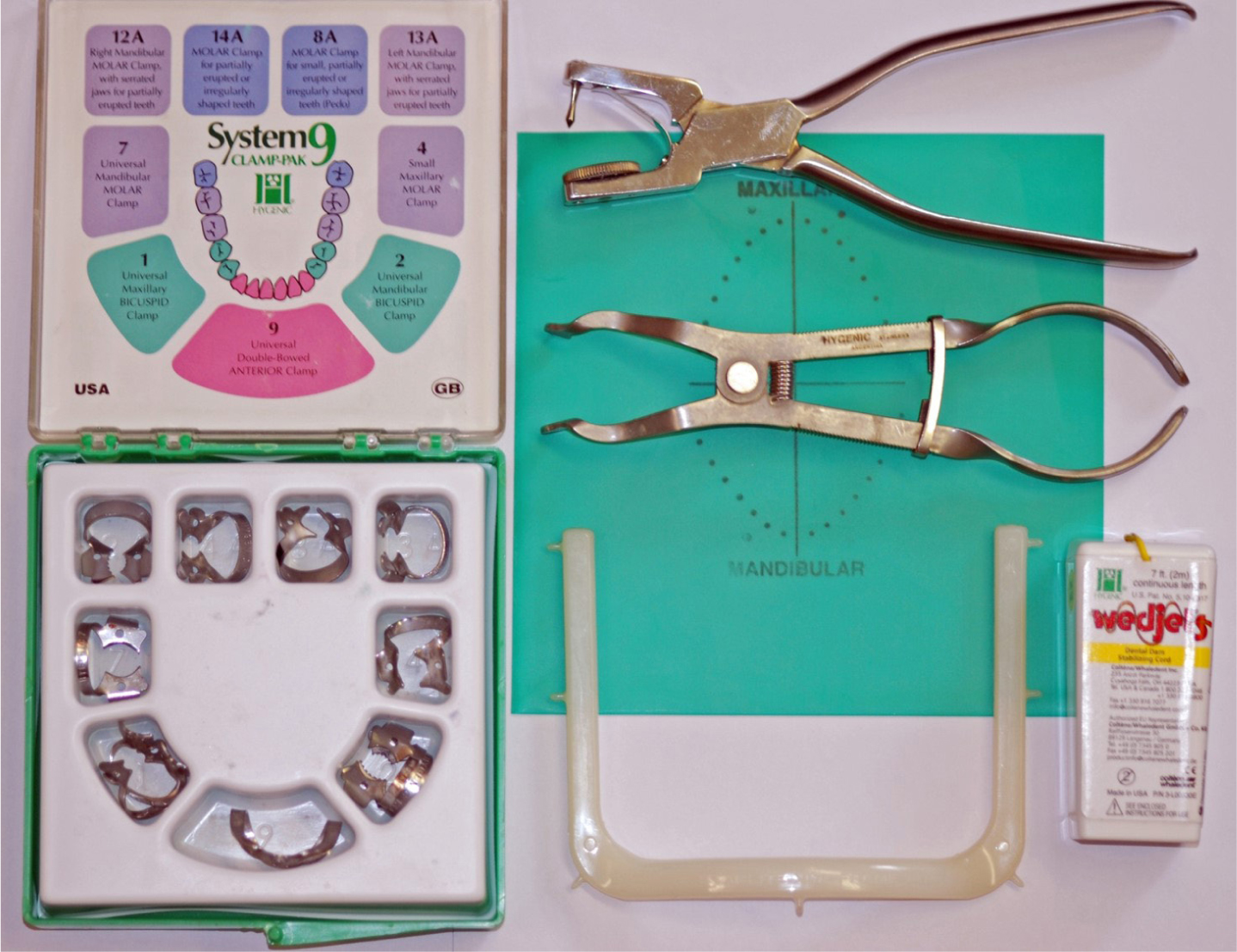
A wide array of rubber dam materials and equipment is available, from a range of different manufacturers. The purchase and mastery of a small selection of high-quality equipment will bring long-lasting rewards at minimal expense (Figure 4).
Figure 4. Basic rubber dam kit. Main components (Hygienic System 9, Coltène-Whaledent) 20 years old.
Rubber dam
A wide variety of rubber dams are available and may be selected based on operator preference using selection criteria described in Table 3.
Size
Rubber dams are generally available in two sizes, 13 x 13 cm and 15 x 15 cmLarger sizes afford more coverage and may be easier to use in most operative procedures
Material
Latex (good handling properties/hypersensitivity risk)15Polyolefin (similar properties to latex)15Elastic silicone plastomer (increased flexibility/tear resistance/small dam holes reduce risk of displacement)15
Thickness
Range includes thin (0.15 mm), medium (0.2 mm), heavy (0.25 mm), extra heavy (0.3 mm) and special heavy (0.35 mm)Medium thickness is recommended as thin dam is more fragile and likely to tear and thick dam, although offering enhanced retraction, may be difficult to place through interdental contact areas
Surface
Where a rubber dam has a dull and a shiny side, it should be orientated so that the dull side faces the occlusal surfaces
Flexibility
Flexibility of the dam affects tension on retainers and patient comfort
Colour
Contrasting and light-reflecting colours improve visual accessLight blue dam is recommended for clinical photography backgrounds
Flavoured
Designed to enhance patient acceptance
Specialized design
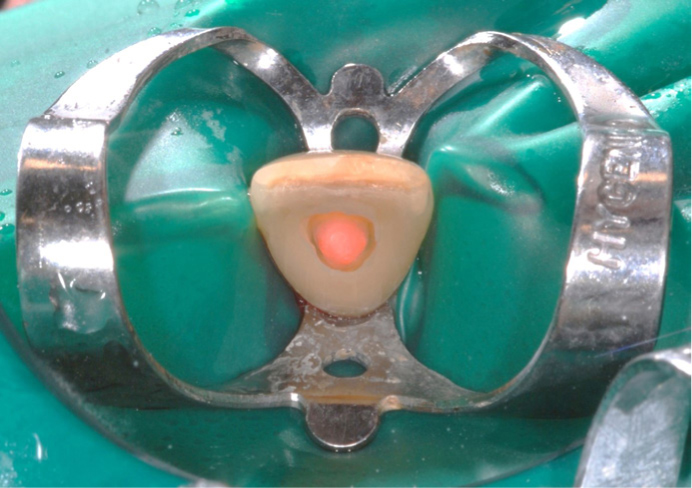
User friendly rubber dam systems may be useful when learning isolation techniques (Figures 5 and 6)
Figure 5. OptiDam™(Kerr, Bioggio, Switzerland) 3-dimensional shaped dam: (a) unique nipple design; (b) contoured anatomical frame; (c) ease of use/rapid application/patient comfort.Figure 6. Drydam® (Directa, Upplands Väsby, Sweden) integral face mask and ear loops. Latex with an absorbent lining (patient comfort and reduced allergy). (Image courtesy of Jansie Van Rensburg).
Retainer selection
While the range of rubber dam retainers is vast, mastery of a limited selection will enable excellent isolation in most clinical situations. General guidelines for retainer selection and placement include:
Purchase only high-quality rubber dam retainers to minimize the risk of fracture;
Retainers should have at least four-point contact to maximize stability and resist rotation;
Metal retainers are generally considered to be the most effective and long-lasting;
The authors recommend winged retainers (confusingly wingless retainers are marked with a W);
For endodontic treatment and for restorative procedures not involving proximal surfaces, the retainer is usually placed on the subject tooth;
For multiple tooth isolation, retainers are placed on a tooth that is distal to the subject tooth, to maximize visual, operative and restorative access;
Rubber dam retainers are orientated with their bow distally to optimize visual and operative access;
Molar retainer designs 12A and 13A may be used for most posterior isolation procedures (Figure 7).
When treating premolars, it is recommended to place the retainer on an adjacent molar, as premolar morphology and premolar retainer design may limit stability;
Retainers may be tried in to test their fit. During fit testing, the retainer should be secured with dental floss to allow safe retrieval in the event of retainer fracture (Figure 8).
Versatile plastic SoftClamps™(Kerr, Bioggio, Switzerland) promote user-friendly isolation of broken down, terminal molar teeth and partially erupted teeth and are useful when not using anaesthesia, eg fissure sealants and minimally invasive preventive resin restorations (Figure 9).
Double bow (‘butterfly’) retainers may be used for anterior teeth; they are usually orientated with the concave bow placed palatally, but may be reversed if that improves stability (Figure 10).
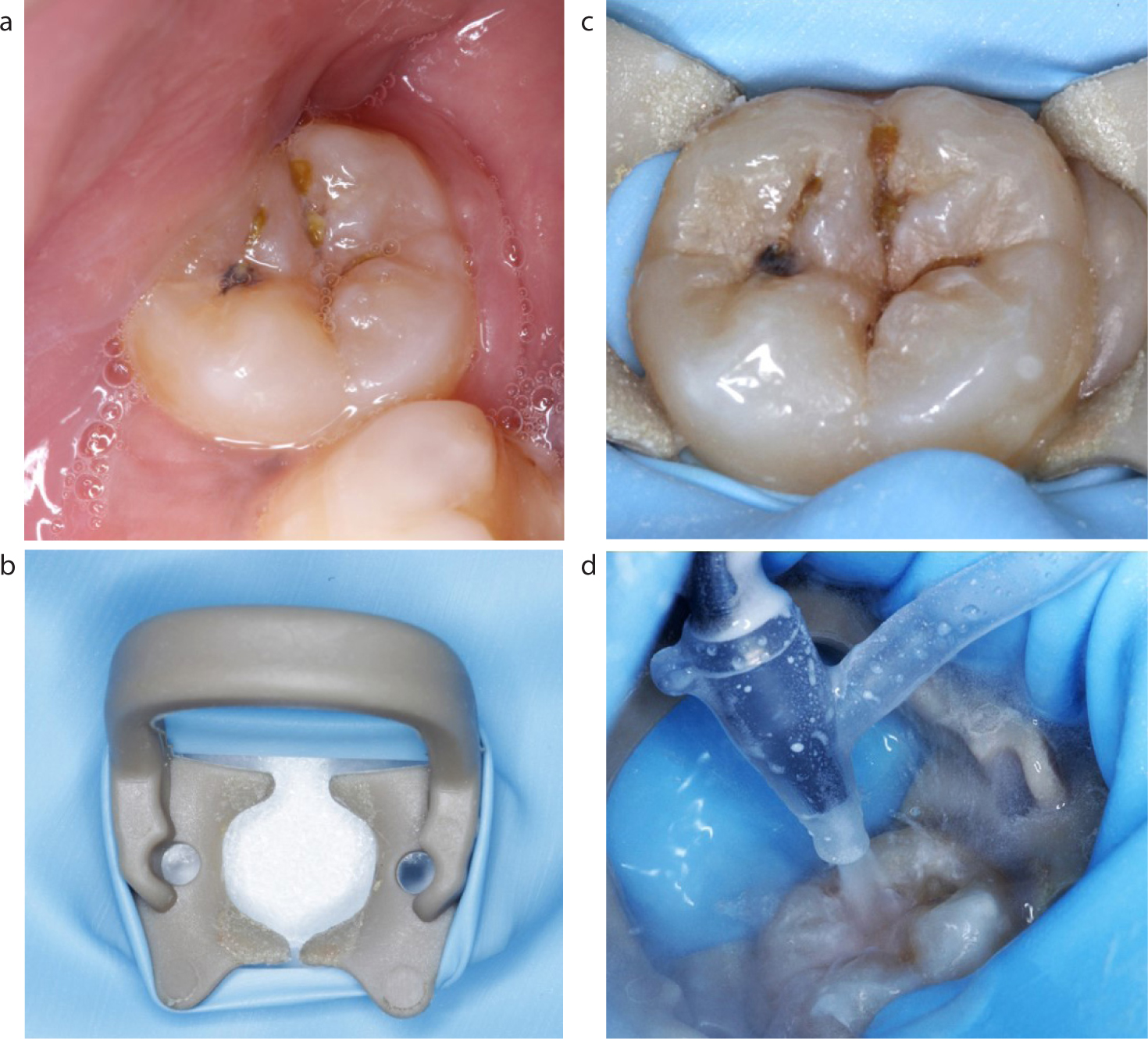
Figure 7. Versatile molar retainers 12A (mandibular right/maxillary left) and 13A (mandibular left/maxillary right) (Hygienic, Coltène-Whaledent).Figure 8. Dental floss placed around a molar retainer for safe retrieval if retainer fracture or displacement occurs during retainer fit test without rubber dam.Figure 9. (a–d) Easy isolation of a partially erupted, malpositioned, third permanent molar enables accurate diagnosis and minimally invasive management of an early Class I carious lesion.Figure 10. Double bow anterior retainers simplify anterior endodontic isolation but may obstruct anterior restorative procedures.
As double bow retainers may obstruct anterior restorative procedures, retainers may be placed distally and/or specialized retainers employed (Figure 11).
Figure 11. Specialized rubber dam retainers for direct (a) and indirect (b) restorative procedures. (Images courtesy of Dipesh Parmar).
Rubber dam punch, forceps and frame
The cutting of holes is usually carried out with a rubber dam punch, often with a rotating metal table that allows different-sized holes to be punched. This is a precision instrument that must be well maintained as clean cuts are required to reduce the risk of tearing when the dam is stretched over teeth/rubber dam retainers. The accurate positioning of rubber dam holes presents challenges for the inexperienced user, which may be overcome by using an inked rubber dam stamp or template or by cutting, rather than punching, a specialized dam (OptiDam™ Kerr, Bioggio, Switzerland) (Figure 5). Tips for the use of rubber dam punches, forceps and frames are as follows:
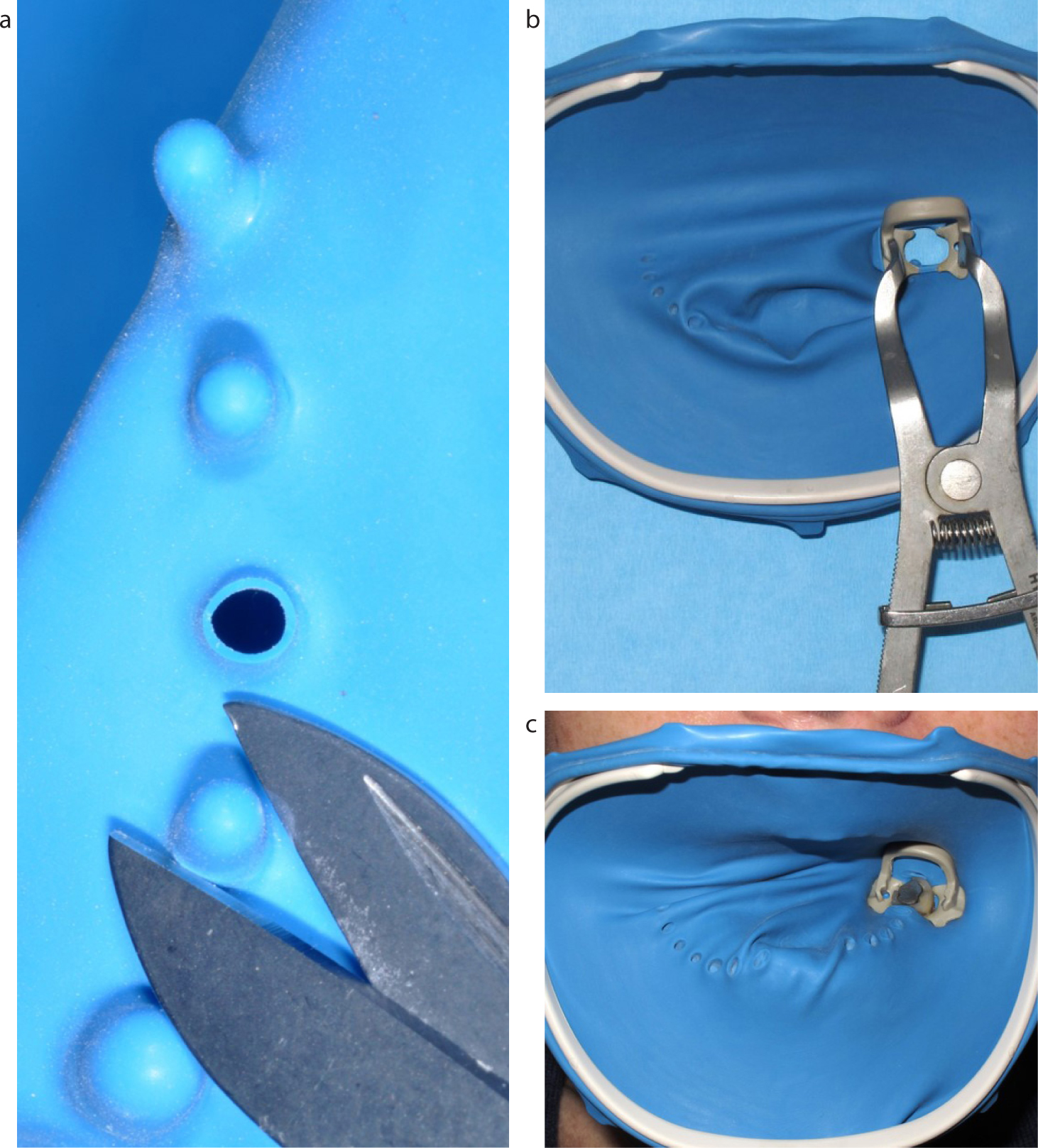
Traditionally the rubber dam may be folded and creased or marked to identify the centre and approximate position of the central incisal area (~2.0 cm from the top of the dam to avoid covering the patient's nose);
However, to maximize respiratory infection control, holes may be repositioned to facilitate nose covering4 (Figure 12).6
While it is possible to isolate full arches or quadrants, for maximum moisture and infection control it is recommended to use the minimum number of dam holes;
Although punching smaller dam holes will optimize the seal, usually the largest hole may be selected for convenience;
Once a rubber dam punch becomes worn, extended clinical use may be gained by using second or smaller holes to maintain cutting accuracy;
While templates are available, freehand hole punching is recommended to suit individual tooth positions;
Once the first hole is punched, any further holes are placed approximately 3.0–4.0 mm apart, leaving spaces for missing teeth;
The easiest way to create the holes without ripping the dam is to punch and push the punching tip through the hole;
Make sure that remnants from previous punching are removed from the hole punch wheel prior to use;
Lightweight rubber dam forceps are recommended;
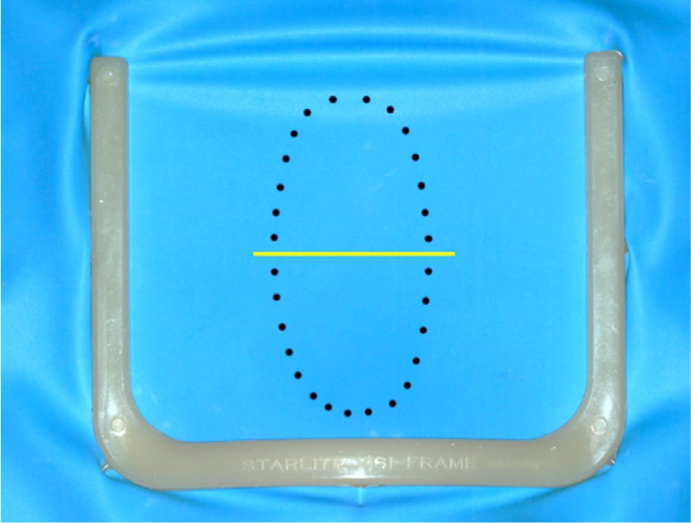
Although the retentive points on metal rubber dam frames are more robust, the authors recommend plastic frames, eg Starlite visi-frame (QED endo, Peterborough, UK) (Figure 12);
Rubber dam frames may be placed on top of, or beneath, the rubber dam or the dam may be folded over the dam frame to create a well, designed to prevent water flowing off the dam edges (Figure 13);
The rubber dam tension should be minimized to allow flexibility during placement and use.
Figure 12. Hole diagram and frame positioning to maximize respiratory isolation.Figure 13. A rubber dam folded over the frame to create a fluid-retentive well.
Accessory equipment
A wide range of accessories are available to optimize rubber dam isolation, and include the equipment listed in Table 4.
Accessory
Function
Example Brand/Manufacturer
Dam stabilizing cord
To prevent dam lifting between contacts
Wedgets® (Latex) (Coltène-Whaledent)
Dental floss ligatures
To optimize dam inversion/cervical seal
eg Oral B Pro-Expert (PTFE)
Rubber dam napkin
To protect patient's skin, eg hypersensitivity
Ora-Shield® (Coltène-Whaledent)
Caulking agent
Optimize dam seal (especially for endodontic procedures)
Figure 14. Caulking agent15 Oraseal™(Optident, Ilkley, Yorkshire). Expanding hectorite clay material prevents saliva leaking into the operative field and blocks passage of chemicals to the mouth, eg endodontic irrigants and phosphoric acid etchant gel.
Matrix systems
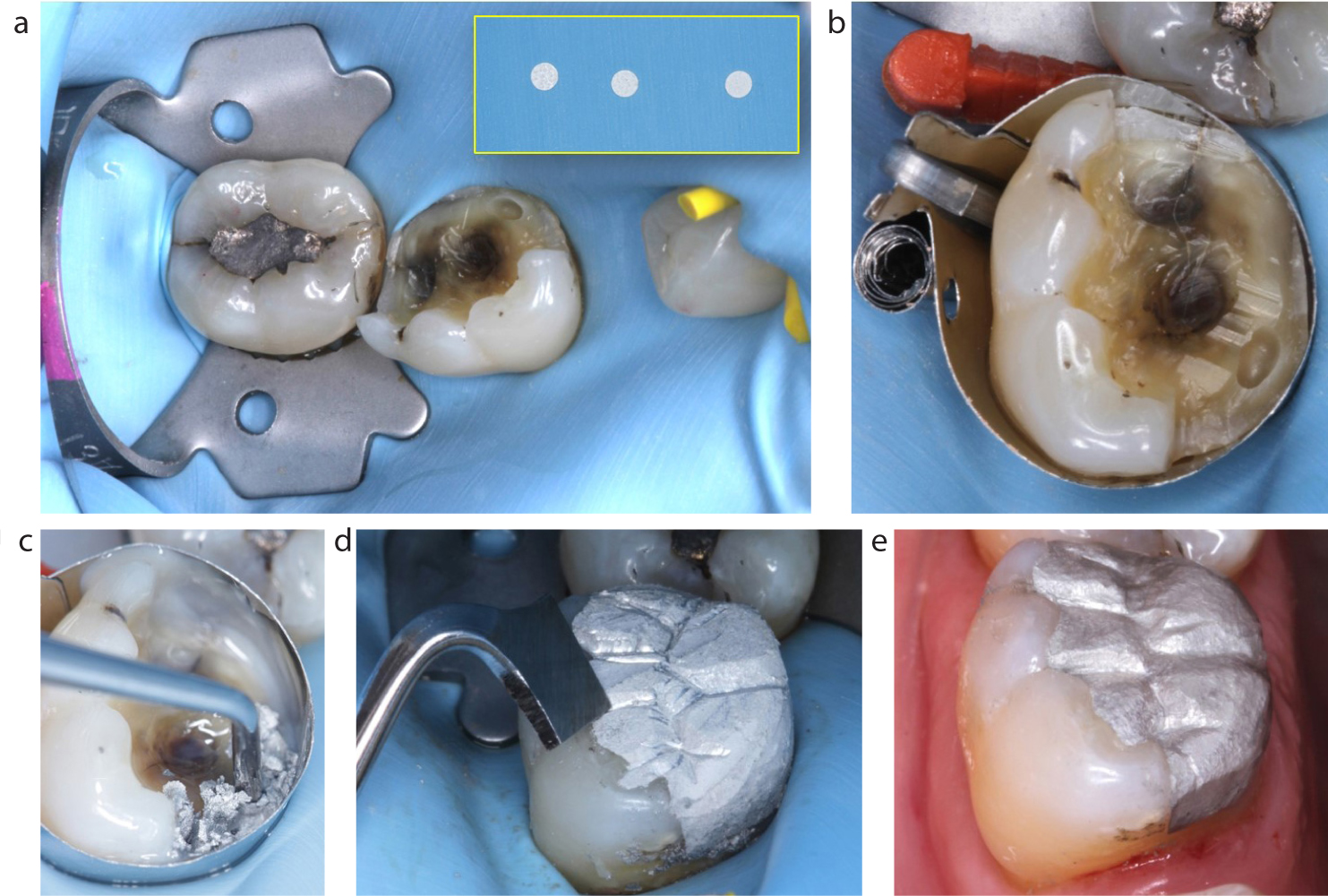
The use of rubber dam isolation optimizes adhesive procedures and, with experience, may be confidently used for the vast majority of restorative treatments. In conjunction with rubber dam isolation, retainer-less, circumferential matrix systems are recommended, eg SuperMat (Kerr, Bioggio, Switzerland) and AutoMatrix® (DentsplySirona, York, Pennsylvania) (Figure 15 a–e).
Figure 15. (a) Rubber dam isolation for a bonded amalgam restoration, dam holes spaced to accommodate a missing tooth. (b) Retainer-less AutoMatrix® system assists isolation and does not interfere with the rubber dam. (c) Rubber dam isolation protects patients from uncomfortable excess amalgam particles during placement (and carving). (d) Anatomical carving is completed with rubber dam in place. (e) Minimal adjustment is necessary after rubber dam removal.
These matrices are easy to use, promote better access and result in better a restorative contacts. They also help to retain the rubber dam and the absence of a retainer reduces the risk of interference. These versatile matrices may also be placed on top of a suitable rubber dam retainer, eg when restoring the last tooth in an arch.
Summary
The use of rubber dam isolation optimizes endodontic and restorative procedures and provides a very high level of infection control. The time taken to master rubber dam materials, equipment and clinical techniques will enhance confidence, improve outcomes and be rewarding for patients and clinicians alike.