Proffit WR, Vig KW Primary failure of eruption: a possible cause of posterior open-bite. Am J Orthod. 1981; 80:173-190
Baccetti T Tooth anomalies associated with failure of eruption of first and second permanent molars. Am J Orthod Dentofac Orthoped. 2000; 118:608-610
Grover PS, Lorton L The incidence of unerupted permanent teeth and related clinical cases. Oral Surg Oral Med Oral Pathol. 1985; 59:420-425
Rhoads SG, Hendricks HM, Frazier-Bowers SA Establishing the diagnostic criteria for eruption disorders based on genetic and clinical data. Am J Orthod Dentofac Orthop. 2013; 144:194-202
Grippaudo C, Cafiero C, D’Apolito I Primary failure of eruption: clinical and genetic findings in the mixed dentition. Angle Ortho.d. 2018; 88:275-282
Sharma G, Kneafsey L, Ashley P, Noar J Failure of eruption of permanent molars: a diagnostic dilemma. Int J Paediatr Dent. 2016; 26:91-99
Frazier-Bowers SA, Simmons D, Wright JT Primary failure of eruption and PTH1R: the importance of a genetic diagnosis for orthodontic treatment planning. Am J Orthodont Dentofac Orthoped. 2010; 137:(160)e1-e7
Hanisch M, Hanisch L, Kleinheinz J, Jung S Primary failure of eruption (PFE): a systematic review. Head Face Med. 2018; 14
Frazier-Bowers SA, Koehler KE, Ackerman JL, Proffit WR Primary failure of eruption: further characterization of a rare eruption disorder. Am J Orthod Dentofacial Orthop. 2007; 131:(578)e1-11
Ahmad S, Bister D, Cobourne MT The clinical features and aetiological basis of primary eruption failure. Eur J Orthod. 2006; 28:535-540
Gorlin RJ, Cohen Jr MM, Hennekam RCOxford: Oxford University Press; 2001
Deffrennes D, Cohen-Lévy J Primary failure of eruption (PFE) and ankylosis of permanent molars: the surgeons experience. J Dentofac Anom Orthod. 2015; 18
Dibiase A, Leggat T Primary failure of eruption in the permanent dentition of siblings. Int J Paediatr Dent. 2000; 10:153-157
Raghoebar G, Boering G, Vissink A, Stegenga B Eruption disturbances of permanent molars: a review. J Oral Pathol Med. 1991; 20:159-166
Lyczek J, Antoszewska J Primary failure of eruption. Etiology, diagnosis and treatment. Dent Med Probl. 2013; 50:349-354
Brady J Familial primary failure of eruption of permanent teeth. Br J Orthod. 1990; 17:109-113
da Costa ED, Peyneau PD, Verner FS Ankylosis of permanent first molar: diagnosis by cone beam computed tomography. Int J Odontostomatol. 2017; 11:319-325
Smith C, Al-Awadhi E, Garvey M An atypical presentation of mechanical failure of eruption of a mandibular permanent molar: diagnosis and treatment case report. Eur Arch Paediatr Dent. 2012; 13:152-156
O’Connell AC, Torske KR Primary failure of tooth eruption. A unique case. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 1999; 87:714-720
Ireland A Familial posterior open bite: a primary failure of eruption. Br J Orthod. 1991; 18:233-237
Frazier-Bowers SA, Long S, Tucker M Primary failure of eruption and other eruption disorders – considerations for management by the orthodontist and oral surgeon. Semin Orthod. 2016; 22:34-44
Kater WM, Kawa D, Schäfer D, Toll D Treatment of posterior open bite using distraction osteogenesis. J Clin Orthod. 2004; 38:501-504
Razdolsky Y, El-Bialy T, Dessner S, Buhler JE Movement of ankylosed permanent teeth with a distraction device. J Clin Ortho.d. 2004; 38:612-620
Susami T, Matsuzaki M, Ogihara Y Segmental alveolar distraction for the correction of unilateral open-bite caused by multiple ankylosed teeth: a case report. J Orthod. 2006; 33:153-159
Siegel SC, O’Connell A Oral rehabilitation of a child with primary failure of tooth eruption. J Prosthod. 1999; 8:201-207
Settembrini L, Gultz J, Kaim J, Scherer W A technique for bleaching nonvital teeth: inside/outside bleaching. J Am Dent Assoc. 1997; 128:1283-1284
Laverty DP, Thomas MBM, Clark P, Addy LD The use of 3D metal printing (direct metal laser sintering) in removable prosthodontics. Dent Update. 2016; 43:826-835
Replacing buried teeth: A Review of primary failure of eruption of permanent teeth and case report Jann Siew Chin Matthew BM Thomas Dental Update 2024 48:4, 707-709.
Authors
Jann SiewChin
BDS, MFDS, MPhil, FDS RCPS (Glasg)
Consultant in Restorative Dentistry, Dental Hospital, Cardiff and Vale University Health Board
Primary failure of eruption is a condition that has variable presentation and can be difficult to diagnose. This article provides an overview of the condition and discusses the management of an unusual case of primary failure of eruption of permanent teeth in a 37-year-old adult.
CPD/Clinical Relevance: Where surgical and orthodontic options are unpredictable, restorative management alone may achieve successful functional and aesthetic outcomes for cases involving primary failure of eruption of permanent teeth.
Article
Primary failure of eruption (PFE) is a condition that involves malfunction of the eruptive mechanism, and results in incomplete eruption of the dentition in the absence of any identifiable mechanical obstacle or recognizable disorder.1 PFE is an uncommon condition with a reported prevalence of 0.06% and which affects females more than males at a ratio of 2:1.2,3
Although the aetiology of PFE is poorly understood, there is a growing body of evidence to suggest that it is genetic in origin.2,4 In particular, studies have found a strong link between eruption failure and the mutation of the PTH1R gene.4,5,6 As such, a positive test for the PTH1R gene mutation is considered confirmatory diagnosis of PFE, although it is accepted that a negative test does not necessarily rule out the condition.4,5,7 More recent studies have supported PFE as an inherited condition.4,8 A systematic review found that a familial pattern existed in 84% of cases.8 In addition, Frazier-Bowers et al found that 26% subjects with PFE had a previous family history.9 For subjects who did not have a family history, it has been speculated that spontaneous mutations are likely to have occurred.1,8
Diagnosis
Diagnosis of PFE can be challenging because it has a variable presentation and can be similar to other conditions.9 Establishing the correct diagnosis is essential, as failure to do so, will lead to inappropriate treatment, protracted treatment times and patient dissatisfaction.6 Often, the diagnosis is based on exclusion of other conditions with similar presentations, which are listed below:1,6
Syndromes and systemic disorders
Impaction of teeth
Mechanical failure of eruption (isolated ankylosis)
Syndrome and systemic disorders
Table 1 lists reported syndromes and systemic disorders that are associated with failure of eruption.8,10 Cleidocranial dysplasia and Gardner syndrome are well-known conditions that are associated with failure of eruption of multiple permanent teeth.11 Unlike PFE, failure of eruption of the dentition that is associated with syndromes and systemic disorders is attributed to factors such as altered craniofacial components or hormonal imbalance impacting bone metabolism.12
Albers–Schonberg osteopetrosis
Apert syndrome
Cherubism
Cleidocranial dysplasia
Down's syndrome
Endocrine disorders
GAPO syndrome
Gardner syndrome
Gorlin–Golz syndrome
Hypodontia-dysplasia of nails syndrome
McCune–Albright syndrome
Nance–Horan syndrome
Oculodental syndrome, Rutherford type
Regional odontodysplasia
Osteoglophonic dwarfism
Impaction
Impaction presents with a normal eruptive mechanism, which is not the case for PFE. There is a local mechanical obstacle that prevents tooth eruption. If the obstacle is removed, continuation of eruption is expected to occur provided there is maintenance of the eruption potential.13 Examples of local mechanical obstacles include cysts, gingival tissue fibrosis, odontomas, supernumerary teeth and tumours.12,14
Mechanical failure of eruption
Mechanical failure of eruption (MFE), more commonly known as isolated ankylosis, is perhaps the most difficult condition to differentiate from PFE because it can have a similar clinical presentation.4,9 In order to distinguish between the two conditions, it is important to recognize the features of PFE and MFE.
PFE primarily affects multiple posterior teeth, where all teeth distal to the most mesially affected tooth are affected by the disorder and this results in a posterior or lateral open bite.1 Anterior and deciduous teeth can also be involved; however, this is much less common.1,13,15,16 The involvement of first permanent molars is considered an essential criteria for the diagnosis of PFE by some authors.4,6 Sharma et al reported that first permanent molars were involved in 100% of affected individuals.6 Similarly, Rhoads et al found that first permanent molars were involved in 93% of affected subjects.4 Overall, Hanisch et al found that the molars were involved in 100% of reported cases, and in 69% of reported cases both the molars and premolars were involved.8 PFE may present in the maxilla or mandible and can be bilateral or unilateral, although bilateral occurrence is more frequent (64%).6,8 For the majority of cases, two or more quadrants are usually affected and a Class III skeletal pattern is common (31%).1,4,8,10 Notably, affected teeth are non-ankylosed initially, and fail to erupt either partially or completely.9 Orthodontic traction of all teeth adjacent to the affected tooth will usually lead to ankylosis.4 PFE is also associated with a higher level of dental anomalies, including curved roots, supernumerary teeth and hypodontia.6,8,10 In 2007, Fraziers-Bowers et al studied subjects affected with PFE and identified three distinguishable forms, subsequently classified into the following groups:9
Type I: All affected teeth display similar lack of eruption potential
Type II: One tooth distal to the most mesially affected tooth has greater eruption, but which is still deemed to be inadequate
Type III: a combination of type I and type II
There are several differences between MFE and PFE. MFE usually involves an individual tooth in a single quadrant.4 In MFE, bilateral occurrence is uncommon and both the maxillary or mandibular arches can be affected.4,6 The aetiology of MFE is usually traumatic, where the periodontal ligament of the affected tooth is damaged, subsequently leading to fusion of cementum to alveolar bone and progressive replacement by bone.12,17 In contrast to PFE, teeth adjacent and distal to the most mesially affected tooth are normal in MFE, and therefore, orthodontic traction of these teeth can be achieved successfully without risk of ankylosis.4,9
To aid differentiation of PFE from MFE, diagnostic criteria developed by Sharma et al are given in Table 2.6
Diagnostic criteria
PFE type I
PFE type II
MFE
Clinical
Permanent molar affected
First molar always
First molar always
First or second molar
Teeth distal to tooth affected
Yes
Yes
No
Primary dentition involved
Possible
Possible
No
Multiple teeth
Possible
Possible
No
Position of tooth
Unerupted or eruption (not fully)
Erupted (not fully) or unerupted
Erupted (not fully) or unerupted
Quadrants involved
Single or multiple
Single or multiple
Single
Posterior or lateral open bite
Yes
Yes
No
Percussion test
N/A
Can be negative for ankylosis
Positive for ankylosis
Radiographic
Eruption pathway
Clear
Clear
Possible bone overlying
Other
Response to treatment
Unsuccessful orthodontic extrusion
Unsuccessful orthodontic extrusion
Successful luxation and subsequent extrusion of the tooth into the line of the arch or extraction of affected tooth and eruption of all teeth distal
Clinical and radiographic assessment
It is evident in the literature that MFE can be treated successfully by extraction and orthodontic alignment, thus early differentiation from PFE is essential.4,18 There is the challenge, however, of detecting the condition early, especially in the developing dentition.9 In the first instance, undertaking a thorough clinical history and examination would help establish a timeline of events, exclude local and systemic factors and determine whether there is a positive family history of PFE. Affected teeth are non-ankylosed and, therefore, will have normal mobility and normal percussive sound if accessible.17 Gathering this information will aid the clinician in determining whether the subject may be affected.
Radiographic assessment is essential for determining the presence of PFE.12 At age 8–9 years, an asymmetry in the eruption pattern of first permanent molars may be identified.9 Reviewing the eruption pattern after 6–12 months using an orthopantomograph (OPT), with the patient in occlusion, can help to determine the presence of PFE, as there will be a lack of eruption. Distinguishing between types I and II can only be undertaken at ages 14 or 15 when the eruption progress of the second permanent molar can be evaluated.9 Otherwise, ‘resorption chimneys’ are characteristic of PFE and these appear as large radiolucent fields around embedded tooth germs, and represent enlarged bony crypts due to resorption of the alveolar process around the tooth germs.15 Cone beam CT imaging can provide additional benefit over conventional radiography because it captures a three-dimensional view of the dental structures, and has the potential to detect the periodontal ligament space more accurately and, therefore, identify the presence of ankylosis.17 Despite the advantages of CBCT imaging, this modality does result in a higher dose of radiation and, therefore, its use should only be undertaken after careful consideration.19
Treatment
The age of the patient and degree of severity will often dictate the treatment options possible. Usually, in minor cases where the dentition has fully developed and there are no aesthetic or functional concerns, it may be perfectly reasonable to accept the position of the affected teeth and provide no treatment.6
Otherwise, in affected children, the primary goals are to improve aesthetics, masticatory function, maintain the occlusal vertical dimension and reduce wear of anterior teeth. Importantly, this will help limit the negative psychological impact the disorder can have on patients. A removable prosthesis is usually ideal as it is quick to construct, non-invasive and easily adjustable. Every few months however, the prosthesis may need to be replaced to accommodate for craniofacial development.12 After growth has completed, a fixed prosthesis may be considered.
Orthodontic treatment, as previously discussed, is highly unpredictable as any attempt to extrude the affected or adjacent teeth will result in ankylosis.1 Clinically, ankylosis becomes apparent where there is intrusion of the anchorage teeth, and there is little or no movement of the affected teeth.1,20 Unsuccessful outcomes using orthodontic traction have been reported in a number of publications.6,12,21,22
In order to overcome the issue of ankylosis, surgical techniques that involve repositioning of the teeth and surrounding alveolar bone have been employed. A few published cases have successfully used either osteodistraction or segmental osteotomy with orthodontic traction.9,12,22,23,24,25 Additionally, orthognathic surgery in combination with restorative or orthodontic treatment has been employed with a successful outcome.12 These procedures although promising, do require a high level of expertise due to its complexity and complication risk.
Restorative management of PFE is scarcely documented in the literature.6,12,26 A retrospective study by Sharma et al reported successful outcomes in cases where the occlusion was accepted and managed restoratively, with or without adjunctive treatment, through achieving occlusal contacts and improving function.6 In general, treatment options include provision of direct restorations, onlays or crowns to achieve occlusal contacts in partially erupted cases.12 Adhesive or conventional bridges may be useful for restoring small unit spaces, where teeth have failed to erupt completely. In mild to moderate cases, extraction of the affected teeth, and placement of implants with or without bone grafting, may be considered.9 This treatment option would become more challenging and less predictable as the severity increases. An alternative approach is the use of removable prostheses, which can be successful in cases with significant numbers of unerupted teeth.26
It is evident that there is a limited number of case reports on the restorative management of this condition. Where surgical and orthodontic options are unpredictable, restorative treatment alone may achieve successful functional and aesthetic outcomes. The management of such a case is presented below.
Case report
Background
In 2014, a 37-year-old male was referred to the Restorative department at Cardiff Dental Hospital. He was concerned about difficulty in chewing and the appearance of gaps between his teeth in the upper and lower jaws. He had previously reported several episodes of pain with the LL7; however, it was asymptomatic at the time of presentaion. The patient had enquired about dental implant treatment because he was not keen on dentures and desired a fixed solution. His medical history was unremarkable except for a penicillin allergy. The patient had admitted a history of irregular attendance and was generally quite anxious about dental treatment. A diet history revealed a high intake of sugary foods.
Figure 1. Pre-operative views. (a) Class II division 2 incisor relationship with 50% overbite and discoloured UL1. (b, c) The UR4, UL4 and UL5 are overerupted and there is a lack of interocclusal space. (d) Partially dentate mandibular arch with retained deciduous canines and recurrent caries of the LL7. (e) Maxillary arch view showing carious lesions, retained roots and retained deciduous canines.
Clinical examination revealed that the UL1 was slightly tender to percussion, discoloured and negative to sensibility testing. Oral hygiene was poor and there was generalized bleeding on probing. A Class II division 2 incisor relationship was noted with 50% overbite and overeruption of the UR4, UL4, UL5. Periodontal examination did not demonstrate any pathological pocketing, but localized inflammation, plaque and calculus deposits were evident. There were carious lesions present on several deciduous and permanent teeth.
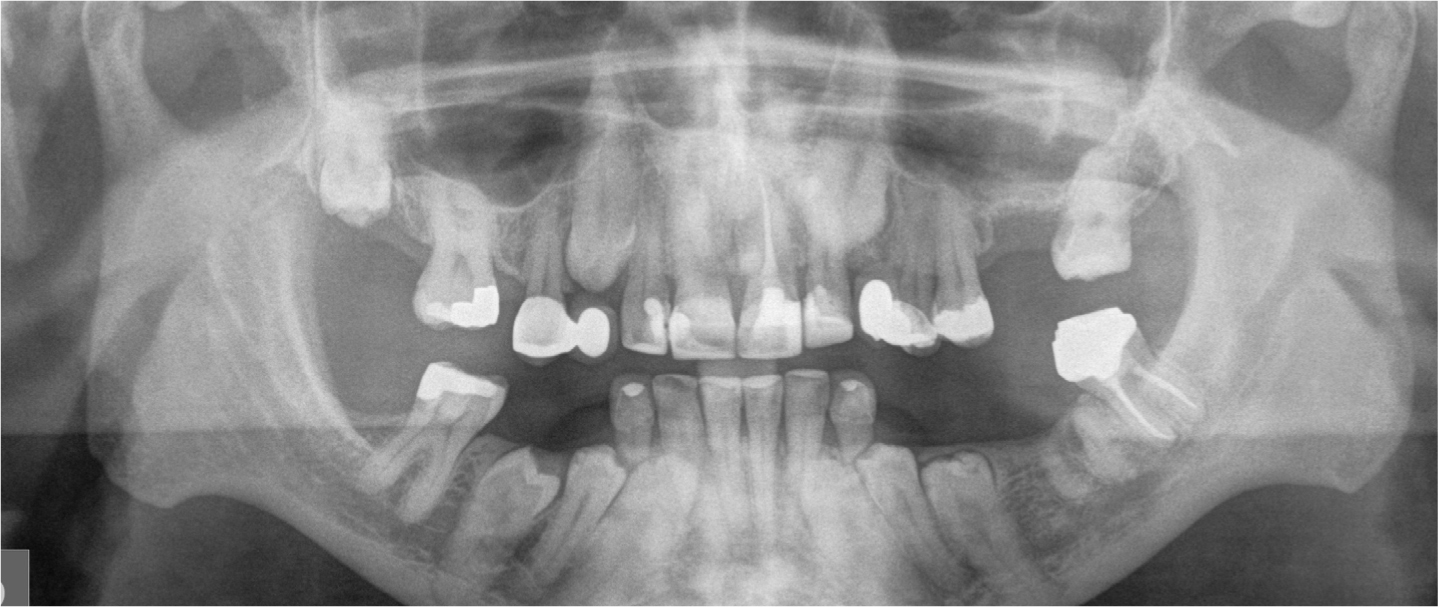
Radiographic examination (Figure 2) revealed the following:
Figure 2. Pre-operative radiographs illustrating primary failure of eruption of permanent teeth. (a) OPT. (b) Peri-apical views of the mandibular anterior teeth.
No cause for the failure of eruption of the teeth was identified from the clinical history, family history or examination. Genetic and blood testing were not undertaken.
Diagnosis
Based on the clinical and radiographic findings, the following diagnoses were made:
Primary failure of eruption;
Retained deciduous canines;
Apical periodontitis UL1, LL7, UR7, UL6;
Retained roots URC, UL6, LL6;
Generalized plaque-induced gingivitis;
Caries.
Management
Initial management involved prevention and stabilization therapy, which included oral hygiene instruction, scale and polish, diet and fluoride advice. The UR7 and UL6 were extracted and carious lesions were managed. Root canal treatment was undertaken on the UL1 and the LL7. As the UL1 was discoloured, non-vital tooth whitening was subsequently undertaken using the inside/outside technique with 16% carbamide peroxide.27
Following the stabilization phase, the definitive restorative phase was planned. Articulated study casts revealed inadequate interocclusal space for prosthetic rehabilitation of the edentulous areas at the current occlusovertical dimension. It was, therefore, deemed necessary to increase the vertical dimension to achieve adequate space for materials and acceptable aesthetics. Diagnostic casts were articulated on a semi-adjustable articulator using a facebow and an interocclusal record in centric relation. The models were also surveyed to identify undercuts. A diagnostic wax-up of the maxillary and mandibular anterior teeth, and a wax try-in of the mandibular removable prosthesis at the increased vertical dimension was carried out. An aesthetic intra-oral preview of the diagnostic wax-up and wax try-in was undertaken to assess the proposed final occlusal scheme and aesthetics. The patient confirmed that he was happy to proceed with the proposed treatment plan. The following treatment was undertaken:
Extraction of the ULC and URC.
Composite resin build-ups of the UR1, UR2, UL1, UL2, LL1, LL2, LR1 and LR2 (Spectrum, Dentsply, Milford, USA).
Composite crowns of the LRC and LLC, which were firm. Buccal undercuts were incorporated onto the crowns to allow effective clasping and retention of the proposed denture.
Six months after the extractions, porcelain fused to metal resin-retained bridges were provided to restore the spaces using the UR4 and UL4 as abutments. These were cemented using Panavia 21 (Kuraray, Japan).
Milled crown at LL7 with mesial guide plane, mesial and lingual rest seats and buccal undercut incorporated (Figure 3).
Construction of mandibular removable cobalt–chrome partial denture using 3D CAD-CAM direct metal laser sintering (produced by Renishaw plc, UK) (Figure 4).28
Figure 3.
(a–c) Intra-oral views of the LL7 milled crown showing incorporated mesial guide plane, mesial and lingual rest seats and buccal undercut (to aid clasping).Figure 4. Stages for construction of mandibular removable cobalt–chrome partial denture. (a, b) Design of denture using Freeform plus computer software (Geomagic, USA). (c) Final denture constructed by direct metal laser sintering (Renishaw plc),
The final outcome of the treatment is shown in Figure 5.
Figure 5. Post-operative views. (a) Composite build up of the upper anterior teeth at an increased vertical dimension allowed interocclusal space for the mandibular removable prosthesis. (b) Mandibular cobalt–chrome denture engaging the LL7 milled crown. (c) Maxillary canine spaces restored with resin-retained bridges using the upper first premolars as abutments. (d) Patient was happy with the aesthetic result.
Review
At his 3-month review, the patient was satisfied with the overall outcome of the treatment regarding function and aesthetics. A joint assessment with an oral and maxillofacial surgeon was subsequently arranged to establish whether surgical removal of the unerupted teeth and placement of dental implants was a feasible option. To aid assessment, another OPT was taken (Figure 6). Removal of these teeth was deemed to carry a high risk of inferior dental nerve paraesthesia and mandibular fracture. It was also determined that extraction of the teeth would increase the complexity of any future dental implant treatment owing to a lack of vertical bone volume. Also, if the implants were not subsequently placed, the denture bearing tissues would have been adversely compromised. The patient opted not to pursue this option and was satisfied to continue using his denture.
Figure 6. Post-operative radiograph (OPT) used to establish whether surgical removal of the unerupted teeth and placement of dental implants was a feasible option.
At his annual review, the patient remained satisfied with the treatment provided overall. Despite the lower denture being comfortable, he admitted that he had stopped wearing it regularly as he did not currently need it for aesthetics or function. He was quite accepting of the fact that if he lost further teeth in the lower arch, a return to wearing a denture would be the most favourable option. The patient was subsequently discharged back to his general dental practitioner for monitoring and maintenance.
Discussion
This case demonstrates most of the features described in the literature regarding PFE.1,4 Notably:
No mechanical obstacles or systemic disorders were identified;
Incomplete eruption of the dentition;
Multiple teeth affected in more than one quadrant;
Bilateral occurrence;
Maxillary and mandibular involvement.
Interestingly, there were some features that did not entirely match the classic presentation of PFE. Not all teeth distal to the most mesially affected tooth were involved. In this case, the LR6 and LL7 had fully erupted into occlusion. The anterior teeth were affected, which is less common. Also, it was not clear whether there was involvement of the first permanent molars, which in PFE, is almost always the case. Owing to severe coronal breakdown and inability to access previous clinical and radiographic information, it is possible that the UL6 and LL6 were involved; however, this was difficult to ascertain.
As highlighted in this case, there is substantial variability in the presentation of the condition and this may partially explain the inconsistency in diagnostic criteria that exists within the literature.1,4,6 It is promising to observe that there is continuously emerging evidence regarding this condition, and it is hoped that in the future, a consensus on diagnostic criteria can be reached. Nonetheless, an example of a useful flow diagram to aid diagnosis and management of the disorder is given in Figure 7.6
Figure 7. Flow diagram to aid diagnosis and management of failure of eruption of permanent teeth.6
The current evidence base supports the decisions made in this case to adopt a conservative restorative approach. It is clear from the literature that surgical exposure and orthodontic traction of the unerupted teeth would have resulted in ankylosis, as well as intrusion of the anchorage teeth. It is also apparent that in this case, osteodistraction or segmental osteotomy was not feasible due to involvement of multiple mandibular teeth, which were deeply positioned and close to the lower border of the mandible. Otherwise, as previously discussed, the complexity and unpredictability of surgical removal of the unerupted teeth and implant treatment excluded this as a desired option for both the patient and the dental team.
Consideration was otherwise given to the future maintenance and management requirements for the patient. Taking into account his history of poor compliance and dental anxiety, the treatment provided (ie composite build-ups, removable prosthesis, resin-retained bridges) was seen to be a realistic and reasonable option for the patient and his general dental practitioner to maintain. Similarly, given the concern about future loss of teeth, particularly the deciduous mandibular canines, extraction of these teeth and replacement using a removable prosthesis could readily be undertaken by the general dental practitioner.
Conclusion
PFE is an uncommon condition that can pose significant challenges with regard to diagnosis and management. It is difficult to detect at an early age, and can be indistinguishable from other conditions such as MFE. The importance of establishing the correct diagnosis cannot be further emphasized, as orthodontic tooth movement is futile in cases of PFE. Where the disorder becomes more severe, treatment options are increasingly limited, as highlighted in this case. It is hoped that this case report will help to demonstrate the benefits of a restorative-only approach when orthodontic and surgical options are complex and unpredictable.