Chevalier J. What future for zirconia as a biomaterial?. Biomaterials. 2006; 27:535-543
Piconi C, Maccauro G. Zirconia as a ceramic biomaterial. Biomaterials. 1999; 20:1-25
Denry I, Kelly JR. State of the art of zirconia for dental applications. Dent Materials. 2008; 24:299-307
Deville S, Chevalier J, Gremillard L. Influence of surface finish and residual stresses on the ageing sensitivity of biomedical grade zirconia. Biomaterials. 2006; 27:2186-2192
Kosmac T, Oblak C, Jevnikar P, Funduk N, Marion L. The effect of surface grinding and sandblasting on flexural strength and reliability of Y-TZP zirconia ceramic. Dent Materials. 1999; 15:426-433
Lawson S. Environmental degradation of zirconia ceramics. J Eur Ceram Soc. 1995; 15:485-502
Scott HG. Phase relationships in the Zirconia-Yttria System. J Mat Sci. 1975; 10:1527-1535
Kosmac T, Oblak C, Jevnikar P, Funduk N, Marion L. Strength and reliability of surface treated Y-TZP dental ceramics. J Biomed Mater Res. 2000; 53:304-313
Sorenson J. All-ceramic restorations. Pers Comm. 2009;
Lughi V, Sergo V. Low temperature degradation – aging – of zirconia: a critical review of the relevant aspects in dentistry. Dent Materials. 2010; 26:807-820
Comlekoglu M, Dundar M, Ozcan M, Gungor M, Gokce B, Artunc C. Influence of cervical finish line type on the marginal adaptation of zirconia ceramic crowns. Oper Dent. 2009; 34:586-592
Warpeha J, Walter S, Goodkind RJ. Design and technique variables affecting fracture resistance of metal-ceramic restorations. J Prosthet Dent. 1976; 35:291-298
Kokubo Y, Tsumita M, Sakurai S, Torizuka K, Vult von Steyern P, Fukushima S. The effect of core framework designs on the fracture loads of all-ceramic fixed partial dentures on posterior implants. J Oral Rehabil. 2007; 34:503-507
Liu YH, Feng HL, Bao YW, Qiu Y. Analysis of the fracture processes in all-ceramic crowns by finite element analysis. Chinese J Stomatol. 2008; 43:561-563
Shirakura A, Lee H, Geminiani A, Ercoli C, Feng C. The influence of veneering porcelain thickness of all-ceramic and metal ceramic crowns on failure resistance after cyclic loading. J Prosthet Dent. 2009; 101:119-127
Proos KA, Swain MV, Ironside J, Steven GP. Influence of core thickness on a restored crown of a first premolar using finite element analysis. Int J Pros. 2003; 16:474-480
Studart AR, Filser F, Kocher P, Gauckler LJ. In vitro lifetime of dental ceramics under cyclic loading in water. Biomaterials. 2007; 28:2695-2705
Plengsombut K, Brewer JD, Monaco Jr EA, Davis EL. Effect of two connector designs on the fracture resistance of all-ceramic core materials for fixed dental prostheses. J Prosthet Dent. 2009; 101:166-173
Larsson C, Holm L, Lovgren N, Kokubo Y, Vult von Steyern P. Fracture strength of four-unit Y-TZP FPD cores designed with varying connector diameter. An in-vitro study. J Oral Rehabil. 2007; 34:702-709
Zhang Y, Lawn BR. Fatigue sensitivity of Y-TZP to microscale sharp-contact flaws. J Biomed Mater Res B Appl Biomater. 2005; 72:388-392
Zhang Y, Lawn BR, Rekow ED, Thompson VP. Effect of sandblasting on the long-term performance of dental ceramics. J Biomed Mater Res B Appl Biomater. 2004; 71:381-386
Zhang Y, Pajares A, Lawn BR. Fatigue and damage tolerance of Y-TZP ceramics in layered biomechanical systems. J Biomed Mater Res B Appl Biomater. 2004; 71:166-171
Heffernan MJ, Aquilino SA, Diaz-Arnold AM, Haselton DR, Stanford CM, Vargas MA. Relative translucency of six all-ceramic systems. Part I: Core materials. J Prosthet Dent. 2002; 88:4-9
Aboushelib MN, Kleverlaan CJ, Feilzer AJ. Effect of zirconia type on its bond strength with different veneer ceramics. J Prosth. 2008; 17:401-408
Beuer F, Schweiger J, Eichberger M, Kappert HF, Gernet W, Edelhoff D. High-strength CAD/CAM-fabricated veneering material sintered to zirconia copings – a new fabrication mode for all-ceramic restorations. Dent Materials. 2009; 25:121-128
Aboushelib MN, Kleverlaan CJ, Feilzer AJ. Microtensile bond strength of different components of core veneered all-ceramic restorations. Part 3: double veneer technique. J Prosth. 2008; 17:9-13
Øilo M, Gjerdet NR, Tvinnereim HM. The firing procedure influences properties of a zirconia core ceramic. Dent Materials. 2008; 24:471-475
Aboushelib MN, de Jager N, Kleverlaan CJ, Feilzer AJ. Microtensile bond strength of different components of core veneered all-ceramic restorations. Dent Materials. 2005; 21:984-991
Taskonak B, Yan J, Mecholsky Jr JJ, Sertgöz A, Koçak A. Fractographic analyses of zirconia-based fixed partial dentures. Dent Materials. 2008; 24:1077-1082
Aboushelib MN, Kleverlaan CJ, Feilzer AJ. Microtensile bond strength of different components of core veneered all-ceramic restorations. Part II: Zirconia veneering ceramics. Dent Materials. 2006; 22:857-863
Hussain SKF, McDonald A, Moles DR. In vitro study investigating the mass of tooth structure removed following endodontic and restorative procedures. J Prosthet Dent. 2007; 98:260-269
Aboushelib MN, Matinlinna JP, Salameh Z, Ounsi H. Innovations in bonding to zirconia-based materials: Part I. Dent Materials. 2008; 24:1268-1272
Lindgren J, Smeds J, Sjögren G. Effect of surface treatments and aging in water on bond strength to zirconia. Oper Dent. 2008; 33:675-681
Atsu SS, Kilicarslan MA, Kucukesmen HC, Aka PS. Effect of zirconium-oxide ceramic surface treatments on the bond strength to adhesive resin. J Prosthet Dent. 2006; 95:430-436
de Souza GMD, Silva NRFA, Paulillo LAMS, De Goes MF, Rekow ED, Thompson VP. Bond strength to high-crystalline content zirconia after different surface treatments. J Biomed Mat Res Part B: Appl Biomat. 2010; 93B:318-323
3M ESPE. Handling and Prep Made Easy. LAVA Precision Solutions. 2006;
Duarte S, Phark J, Tada T, Sadan A. Resin-bonded fixed partial dentures with a new modified zirconia surface: a clinical report. J Prosthet Dent. 2009; 102:68-73
Jung RE, Pjetursson BE, Glauser R, Zembic A, Zwahlen M, Lang NP. A systematic review of the 5-year survival and complication rates of implant-supported single crowns. Clin Oral Implants Res. 2008; 19:119-130
Kinsel RP, Lin D. Retrospective analysis of porcelain failures of metal ceramic crowns and fixed partial dentures supported by 729 implants in 152 patients: patient-specific and implant-specific predictors of ceramic failure. J Prosthet Dent. 2009; 101:388-394
Pjetursson BE, Bragger U, Lang NP, Zwahlen M. Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). Clin Oral Implants Res. 2007; 18:97-113
Pjetursson BE, Sailer I, Zwahlen M, Hammerle CH. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part I: Single crowns. Clin Oral Implants Res. 2007; 18:73-85
Sailer I, Feher A, Filser F, Gauckler LJ, Luthy H, Hammerle CH. Five-year clinical results of zirconia frameworks for posterior fixed partial dentures. Int J Prosth. 2007; 20:383-388
Pjetursson BE, Tan WC, Tan K, Bragger U, Zwahlen M, Lang NP. A systematic review of the survival and complication rates of resin-bonded bridges after an observation period of at least 5 years. Clin Oral Implants Res. 2008; 19:131-141
Pjetursson BE, Lang NP. Prosthetic treatment planning on the basis of scientific evidence. J Oral Rehab. 2008; 35:72-79
Sailer I, Pjetursson BE, Zwahlen M, Hammerle CH. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part II: Fixed dental prostheses. Clin Oral Implants Res. 2007; 18:86-96
Kreissl ME, Gerds T, Muche R, Heydecke G, Strub JR. Technical complications of implant-supported fixed partial dentures in partially edentulous cases after an average observation period of 5 years. Clin Oral Implants Res. 2007; 18:720-726
Walton TR. An up to 15-year longitudinal study of 515 metal-ceramic FPDs: Part 1. Outcome. Int J Prosth. 2002; 15:439-445
Aglietta M, Siciliano VI, Zwahlen M, Bragger U, Pjetursson BE, Lang NP A systematic review of the survival and complication rates of implant supported fixed dental prostheses with cantilever extensions after an observation period of at least 5 years. Clin Oral Implants Res. 2009; 20:441-451
Bragger U, Aeschlimann S, Burgin W, Hammerle CH, Lang NP. Biological and technical complications and failures with fixed partial dentures (FPD) on implants and teeth after four to five years of function. Clin Oral Implants Res. 2001; 12:26-34
Ozcan M, Niedermeier W. Clinical study on the reasons for and location of failures of metal-ceramic restorations and survival of repairs. Int J Prosth. 2002; 15:299-302
Tsumita M, Kokubo Y, Vult von Steyern P, Fukushima S. Effect of framework shape on the fracture strength of implant-supported all-ceramic fixed partial dentures in the molar region. J Prosth. 2008; 17:274-285
Gottlow J, Dard M, Kjellson F, Obrecht M, Sennerby L. Evaluation of a new titanium-zirconium dental implant: a biomechanical and histological comparative study in the mini pig. Clin Implant Dent Relat Res. 2010;
Zirconia restorations are now accepted and commonly prescribed in dentistry. However, these materials undergo hydrothermal ageing which can reduce their clinical performance. Appropriate handling is essential to limit the restorations’ susceptibility to low temperature degradation/ageing. Through appropriate clinical prescribing and laboratory manufacture, an aesthetic, strong and long-lasting restoration can be fabricated.
Clinical Relevance: This article will inform the reader about zirconia as a dental material as well as how best to handle a zirconia restoration.
Article
What is zirconia?
In ancient history zircon was known to be a gem. The name zirconium comes from Zargon which translates from Arabic to golden in colour. Zargon is a composite of two Persian words; Zar meaning gold and Gun meaning colour. Zirconium dioxide (ZrO2: zirconia) was first identified by a German chemist in 1789. The compound was used for a long time as part of a rare earth oxide mix to pigment ceramics. In its pure form, it is a white crystalline material and has three crystallographic forms, monoclinic, tetragonal and cubic. Monoclinic is the most naturally occurring form, while ‘cubic zirconia’ is rarely found in nature and is best known as a diamond simulant owing to a structural chemistry similar to cubic carbon and a high index of refraction. This is referred to as zircon by jewellers; however zircon is actually the mineral name for naturally occurring zirconium silicate.
Zirconia ceramic was first introduced to the medical profession in 1969 in the field of orthopaedics as a proposed material for hip replacements.1 Since then it has been described as ‘ceramic steel’2 and is widely used in both dentistry and medicine.3 Owing to its impressive flexural and compressive strengths of 900–1200 MPa and 2000 MPa, respectively,4 zirconia has developed into an efficient core material for all-ceramic restorations.
Many different methods of constructing an all-ceramic restoration have been developed, including sintering, cast glass and glass infusion. Contemporary methods include vacuum-pressing and milling via CAD/CAM methods. CAD/CAM zirconia restorations are now considered by many dentists to be the top of the range restorative treatment for a patient. However, despite the increase in size of the digital workflow, both the dentist and the technician must appreciate how to handle the materials appropriately.
Crystallographic structure
Pure ZrO2 has a monoclinic crystal structure at room temperature which transitions to tetragonal and cubic at increased temperatures. It transforms into a tetragonal phase between 980°C and 1173°C and moves to cubic above 2370°C. A volume expansion of approximately 4.5%5 occurs on cooling from the tetragonal to monoclinic phase. This transformation induces very large stresses and will cause pure ZrO2 to crack upon cooling from high temperatures. Several different oxides can be added to zirconia to stabilize the tetragonal and/or cubic phases; magnesium oxide (MgO), yttrium oxide, (Y2O3), calcium oxide (CaO), and cerium (III) oxide (Ce2O3) allow these phases to remain at room temperature without catastrophic crack propagation.2,4,5 Despite more difficult sintering, zirconia stabilized with yttria has better mechanical properties than other combinations.1,2
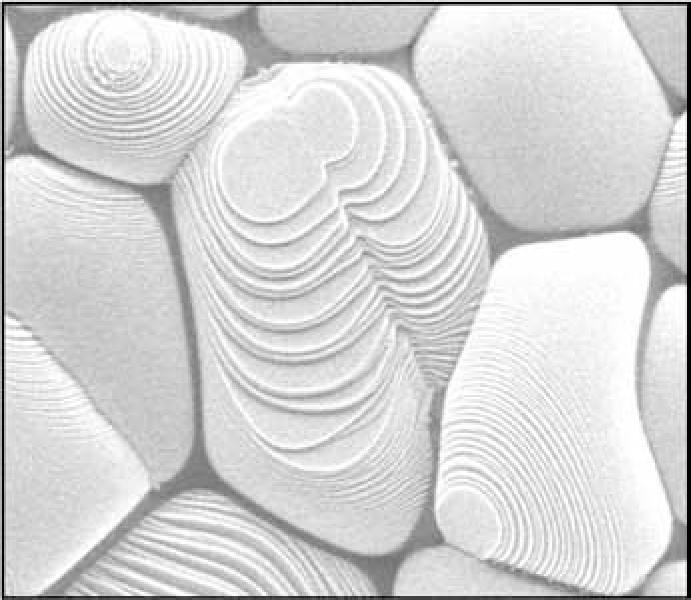
The addition of stabilizing oxides results in a multiphase material known as partially stabilized zirconia (PSZ). A paper in Nature, aptly named ‘Ceramic Steel?’ was the first to record how a phase shift from tetragonal to monoclinic can result in improved mechanical strength and toughness of zirconia.2 If sufficient quantities of the metastable tetragonal phase are present, then an applied stress, magnified by the stress concentration at a crack tip, causes the tetragonal phase to convert to monoclinic. This phase transformation can then put the crack into compression, retarding its growth and enhancing the fracture toughness of the material. This mechanism, known as transformation toughening, significantly extends the reliability and lifetime of products made with stabilized zirconia compared with other ceramics (Figure 1).
Figure 1. This SEM picture demonstrates grains of zirconia which have bulged in size as a result of transformation toughening (courtesy of 3M ESPE).
Ageing of zirconia
The ageing of zirconia, known as low temperature degradation (LTD) has been studied extensively.3,5–8 It is exacerbated by water, water vapour and increased temperatures.8 Ageing is associated with surface roughening and microcracking of the material in which phase changes from tetragonal to monoclinic occur. The initiation and progression of ageing are influenced by many factors. Aside from environmental factors, grain size, phase assemblage, density and concentration of stabilizing agent, all play a role.6,8
Larger grain sizes are less stable and more susceptible to ageing. It has been shown that grain size can be controlled by sintering methods; higher sintering temperatures and longer sintering times lead to larger grains.9 Critical grain size increases with increasing concentration of stabilizing agent, resulting in a greater resistance to ageing, ie grains no longer need to be so small to resist ageing. This happens as a result of cubic content increasing at the expense of the metastable tetragonal phase. However, this has resultant detrimental effects on the properties of the ceramic. Most studies concerning ageing have been conducted on yttria stabilized zirconia. However, magnesium oxide stabilized zirconia shows a similar susceptibility to hydrothermal ageing. Calcium oxide and cerium (III) oxide, on the other hand, do undergo phase changes, but at a slower rate than yttria. Should CeO or CaO be of a relatively high concentration, the material becomes significantly resistant to ageing.8
It has been demonstrated that deep scratches can be introduced into the ceramic during machining or polishing. These scratches are areas of monoclinic transformation that grow in height and diameter with time, eventually coalescing6 and theoretically increasing the likelihood of cracking.
Annealing at 900 °C for one hour has been shown to induce reverse transformation.10 This also results in a relaxation of surface stresses and subsequent decrease in strength, but will also act to increase ageing resistance.5 This may be accomplished during the firing of veneering ceramic on to a zirconia coping. Another method shown to combat LTD is coating the zirconia, thus preventing its attack by solvents and protecting the weak surface flaws. It is assumed that veneering ceramic functions in this way.
Despite the perceived need to cover zirconia restorations to prevent ageing, a recent communication described making axial and occlusal surfaces of unveneered zirconia ceramic.11 This option is attractive as it allows for a more conservative tooth preparation on the palatal and lingual aspects of the teeth where the width of the finish line could be reduced from 1.3 mm to 0.8 mm; however, these recommendations have yet to be reported in an in vivo trial.
The literature in this area is extensive and is well covered in a recent review article by Lughi and Sergo.12
Formulations
One of the most commonly used zirconia formulations is stabilized with yttria in the form of 3Y-TZP (3Yttria – tetragonal stabilized zirconia polycrystals). This particular formulation is used in 3M ESPE's LAVA® and Ivoclar Vivadent's E-max ZirCAD®. Zirconia toughened alumina ZTA is another way in which the advantageous properties of zirconia can be used for dental restorations. In-Ceram® (Vita) ZTA uses 12Ce-TZP to toughen its core at a volume of approximately 33%. It is manufactured through soft machining or slip-casting. Unfortunately, however, ZTA shows porosity of between 8 and 11%, which adversely affects the mechanical properties of the ceramic.5 Partially stabilized zirconia (Mg-PSZ) is also currently marketed for dental purposes as Denzir-M® (Dentronic AB). It has generally been unsuccessful owing to large grain sizes, porosity and unfavourable wear characteristics.4 It also requires a high sintering temperature and must be controlled precisely.4
Tooth preparation and clinical considerations
Zirconia may be used to construct copings and frameworks for full coverage single crowns and fixed partial dentures (FPD). A veneering ceramic is then layered and sintered on to this surface. These restorations require similar preparation to conventional porcelain fused to metal crowns (PFM).1 The preparation follows principles which were established for cast restorations in the early-to-mid twentieth century. Despite closely following these principles, preparations for zirconia vary from cast restorations in one important respect, preparation depth.
Porcelain fused to metal restorations can be produced with a palatal chamfer of 0.5 mm thickness which allows adequate strength and a margin constructed in metal. However, zirconia restorations cannot have such conservative preparations and currently must be veneered with porcelain to protect the coping. This results in a relatively constant preparation depth palatally and labially. The minimum labial and palatal preparation depth for an anterior zirconia restoration is 1.3 mm, which is far from conservative.
Marginal configuration
During tooth preparation, a dentist must select the marginal design which results in the best or most predictable outcomes for a patient. This is influenced by the remaining tooth structure, aesthetic requirements and material choice for the restoration. Traditional all-ceramic porcelain jacket crowns required a circumferential shoulder preparation to produce marginal strength and easier manufacture. With cast alloy restorations, there is a greater flexibility and the dentist can afford to be more conservative.
Marginal opening of zirconia crowns has been assessed and it was found that, with cementation, a knife edge preparation resulted in the least amount of marginal opening.13 However, the authors discuss the disadvantages of a knife edge preparation for a milled ceramic and the difficulties it produces in manufacture. For clinical use, the optimal marginal configuration is a shoulder or heavy chamfer. Figure 2 demonstrates that an excellent marginal fit is possible.
Figure 2. Marginal fit (courtesy of 3M ESPE).
CADCAM impressioning
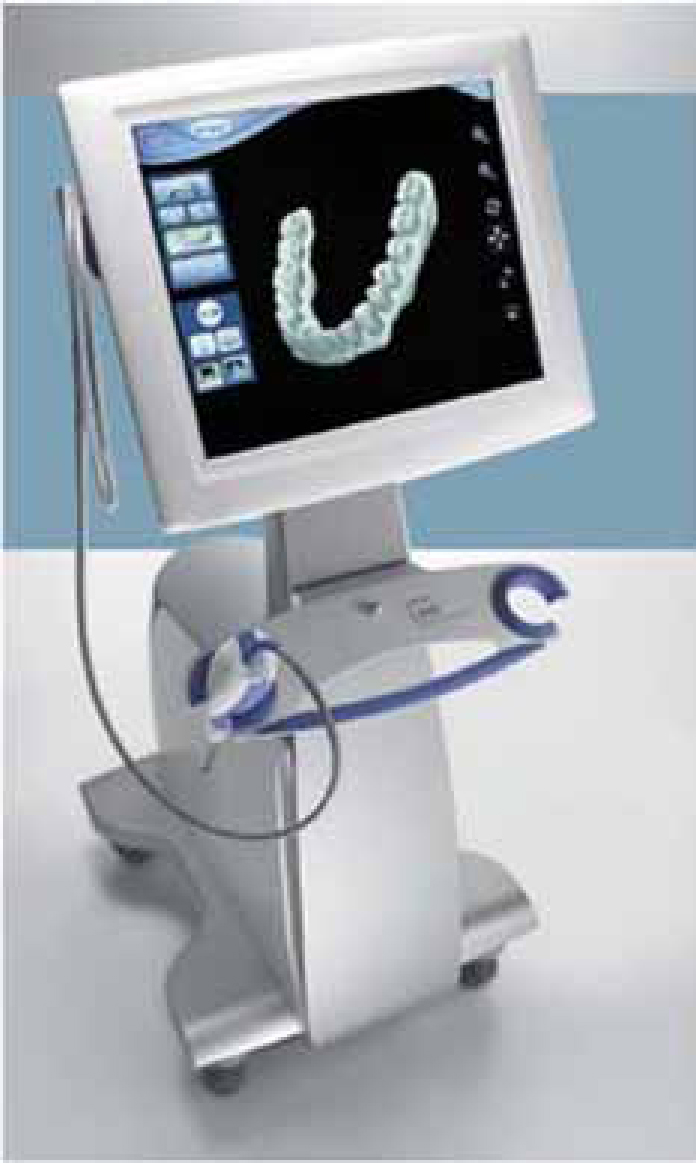
Manufacture of zirconia frameworks is via a CAD/CAM process. The data for the design of the framework therefore must be digitized at some stage in the workflow. This can take place at the chairside using an intra-oral chairside scanner (LAVA COS® 3M ESPE, CEREC Connect® Sirona) (Figure 3). Digitization at this stage is exciting and shows promise for the future but can be costly to set up and has a learning curve which may not easily fit into the busy life of the general dental practitioner.
Figure 3. LAVA chairside intra-oral scanner (courtesy of 3M ESPE).
Alternatively, a conventional elastomeric impression can be made and scanned, either in the laboratory or in the dental surgery (3Shape®). Finally, casting the impression in type IV dental stone and scanning of the model is also an appropriate method (LAVA Scan ST®, 3M ESPE). Whichever method is used, once the die is digitized, the technician/dentist can begin design of the framework.
Design of the restoration
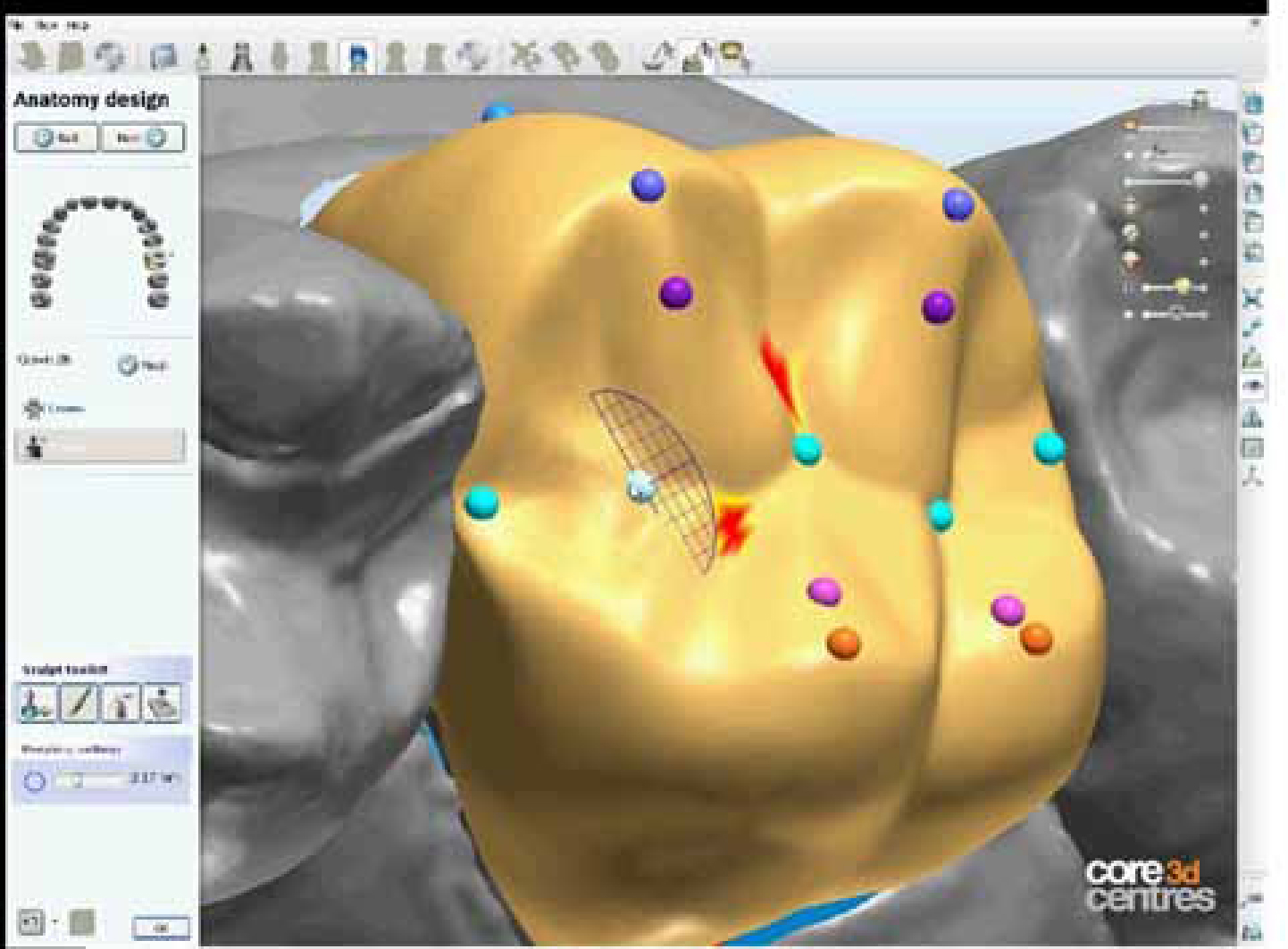
CAD/CAM techniques used in the fabrication of zirconia copings and frameworks allow the technicians complete flexibility. With a ‘virtual wax knife’ the technician can cut-back a digitally generated full contour design, allowing anticipation of the final restoration contour (Figure 4).
Figure 4. Design software is used to design the full contour to a customized shape such that appropriate cut-back can be done to generate the coping design (courtesy of DTS, Glasgow).
Coping design
The design of metal-ceramic copings has been well established for many years.14 Despite a lack of studies, some authors have commented on the need for porcelain fused to metal (PFM) coping design rules to be followed when using zirconia.15 Greater tensile stresses have been shown to exist in ceramic copings which do not adequately support the overlying porcelain16 (Figure 5).
Figure 5. These zirconia copings will clearly not support the overlying porcelain.
Comparative studies have been conducted between all-ceramic and metal-ceramic crowns on implant abutments to assess geometric requirements. Two different framework designs with two different incisal thicknesses of veneering porcelain were used for each alumina all-ceramic and high noble metal ceramic crown systems with identically-shaped crowns. Thermocycling and unidirectional loading were used to fatigue the specimens. Interestingly, geometry was a significant factor for PFMs but not for all-ceramic crowns.17 Thickness of the ceramic coping, on the other hand, has a significant influence on the resulting stresses in the coping and veneering porcelain of an axially loaded crown by being inversely proportional.18
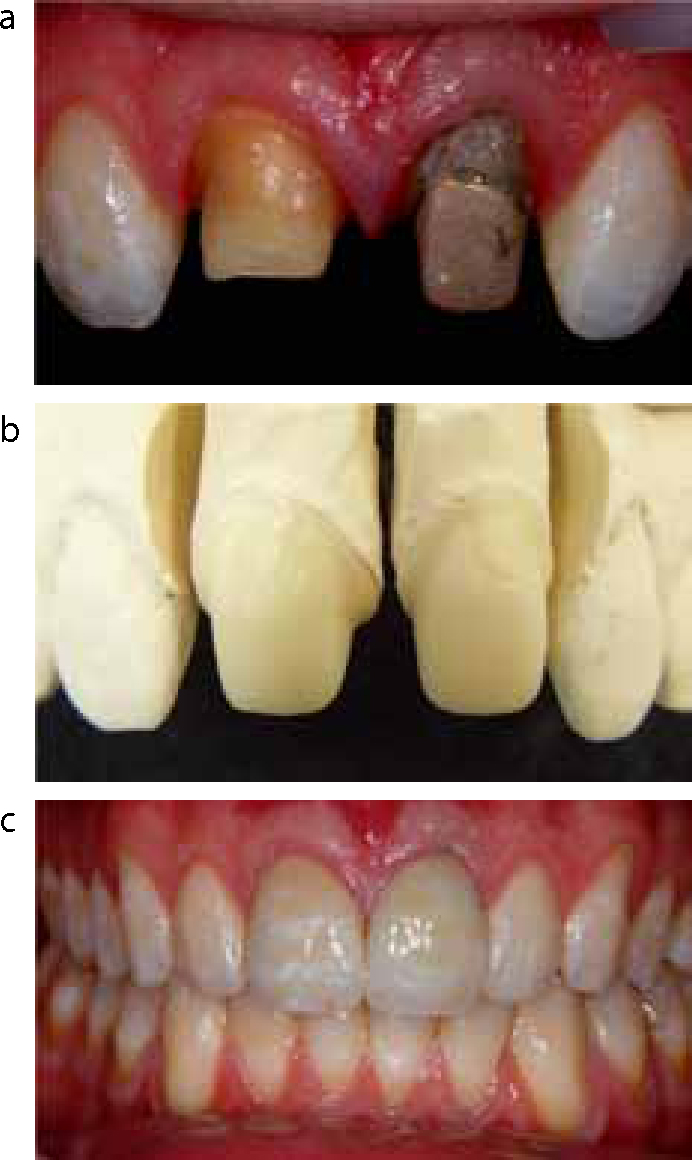
It would seem practical, based on the available evidence, to recommend that basic principles of coping design established for the PFM crown are applied to zirconia copings. Therefore, the veneering ceramic should be adequately supported at all times (Figure 6 a–c).
Figure 6. (a–c) Two central incisors restored with zirconia crowns. Note the different axial heights of the preparations but the identical heights of the copings, providing support for the ceramic. Also note the excellent aesthetic outcome of this case, despite the post and core and discoloured root of UL1. The replication of the hypomineralization and surface characteristics were achieved with the use of a feldspathic veneering ceramic.
Framework design for fixed prostheses
The minimum connector diameters for 3-, 4- and 5-unit fixed partial dentures constructed for different ceramics have been calculated.19 These are summarized in Table 1. This clearly demonstrates the advantages of zirconia over other high strength ceramics. In a study assessing connector design,20 three materials were tested, heat-pressed lithium disilicate glass ceramic, milled lithium disilicate glass and milled yttrium-stabilized tetragonal zirconia polycrystals. Two connector designs, round and sharp with similar diameters, were studied. Higher maximum failure loads were found for the round connector design when compared with the sharp design, with zirconia being highest. The authors also demonstrated that, although connector design can be changed to improve framework fracture toughness, the initial fracture load at which veneering porcelain fractured did not show significant differences between the different designs. However, other authors have questioned this and have recommended a connector diameter of 4 mm inclusive of veneering ceramic.21 A connector diameter of 4 mm is large and would require crown height of some 6 or more millimetres to allow access for plaque control procedures. This is not often found in posterior teeth, thus making the ideal dimensions of a connector difficult to deliver in all clinical situations.
Zirconia
Slip cast glass infused zirconia
Lithium disilicate
3-unit bridge
2.5 mm
4.1 mm
4.9 mm
4-unit bridge
3 mm
4.9 mm
5.9 mm
5-unit bridge
3.5 mm
5.7 mm
6.9 mm
Manufacture of the restoration
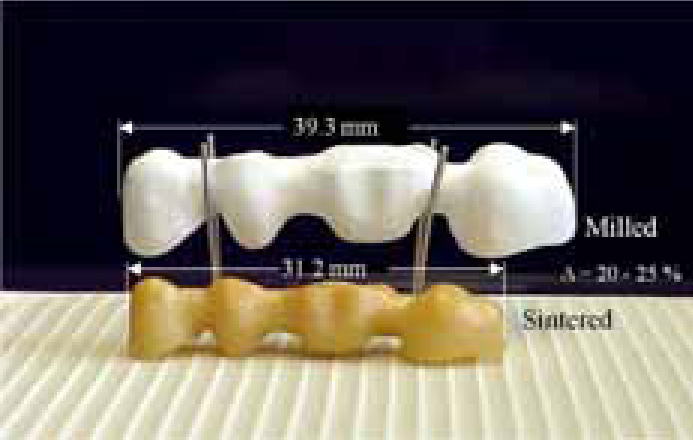
Once the zirconia restoration has been designed, the data must be sent to the milling machine for fabrication. 3Y-TZP dental restorations are constructed in one of two ways: soft machining of pre-sintered blanks in their green state, followed by final sintering at high temperature or hard machining of fully sintered blocks. The first has the disadvantage of approximately 20% shrinkage during the final sintering process, which must be compensated for during milling (Figure 7). However, the latter approach is not only more costly in terms of milling machinery owing to the hardness of the fully sintered block, but the copings contain a far larger monoclinic concentration upon completion. Despite giving the ability to mill to a 1:1 ratio, this method leads to surface microcracking and a decreased resistance to LTD.
Figure 7. Each block of zirconia is accurately measured to determine its exact shrinkage. The milling software then compensates for this when milling in the green state (courtesy of 3M ESPE).
Handling of the restoration
Conflicting evidence has been published on the post-sintering treatment of zirconia ceramic. Manufacturers recommend that minimal grinding, polishing or sandblasting be carried out, despite some systems requiring a degree of grinding to fit the die. Deville et al6 reported that rough polishing can produce a compressive surface stress layer, which is beneficial for ageing resistance. However, Kosmac et al revealed that surface grinding and sandblasting have differing effects on the strength of Y-TZP ceramics.10 While grinding acted to lower the mean strength and Weibull modulus, sandblasting caused strengthening of the ceramic, but at the expense of somewhat lower reliability. By way of further contrast, other studies have shown that sandblasting has detrimental long-term effects.22–24
Following hard machining, a number of surface scratches and transformed areas will be present. These promote residual stresses, leading to greater susceptibility to LTD.6 Smooth polishing, as opposed to rough grinding, was shown in this study to cause a preferential phase transformation around these scratches, which was beneficial.
In summary, the sintered zirconia framework should be lightly ground with a fine diamond (≤30µm grit) prior to application of the veneering ceramic. Intense grinding should be avoided. Sandblasting of the zirconia should be avoided unless a digital veneering system is being used (see Veneering Material section). With respect to the fitting surface of the restoration, no grinding or sandblasting should be carried out unless the sandblasting is a part of tribochemical silicatization to improve bond strengths to resin cements (see Bonding and Cementation section).
Colouring of the framework
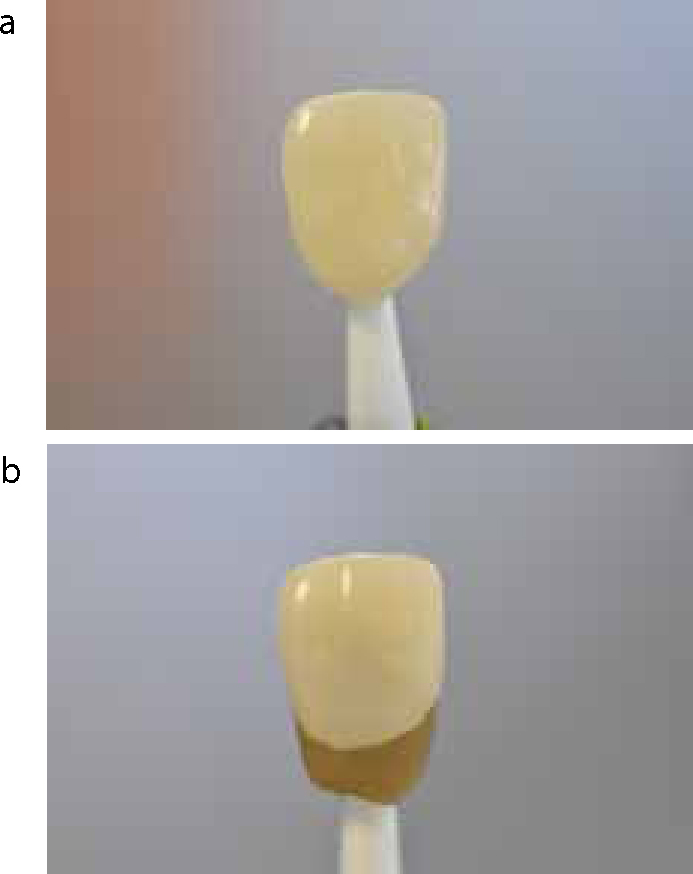
Metal-free all-ceramic restorations have been shown to influence soft tissue colour less than those made of porcelain fused to metal.1 The reason for this and the consequent aesthetic advantage of zirconia over metal is plain to see when examining copings visually (Figure 8). In comparison with other all ceramic systems, zirconia is by far the most opaque.25 Clinically, this opacity allows the relatively thin copings to be used to mask darkened tooth structure or metal cores. Despite this positive aspect of zirconia, a clinician should still be aware of, and communicate shade stumps to, his technician so that shade changes required at the chairside are kept to a minimum (Figure 9). However, should the white opacity of the material impart too high a value to the colour of the restoration, the core's chroma can be altered. Prior to sintering, the porous zirconia is immersed in a colouring liquid which penetrates the coping (Figure 10).
Figure 8. Zirconia copings have an obvious aesthetic advantage.Figure 9. (a, b) Shade stumps can be used by the technician and are an important communication tool.Figure 10. Immersion of the framework to add chroma (courtesy of 3M ESPE).
Following soft machining, copings can be coloured from a choice of eight different solutions of cerium, bismuth and iron (Figure 11). The concentration of the solution, as well as the final sintering temperature, influence the deposition of surface colour. This has no effect on the properties or microstructure of the ceramic.5 However, it was discovered by SEM analysis that surface colourings crystallize during sintering and seem to lead to significantly poorer bond strengths of the veneering ceramic.26
Figure 11. Different colours of the zirconia framework (courtesy of 3M ESPE).
Veneering
Material
A variety of methods is available when choosing how to veneer the coping:
No veneering, ie full contour all zirconia restoration (Figure 12);
Conventional layering with appropriate feldspathic porcelain;
Pressing a glass ceramic on to the coping;
Using CAD/CAM methods to mill the glass ceramic veneer which is then fused to the coping, as in the Digital Veneering System (DVS®) from 3M ESPE.
Figure 12. A full contour zirconia restoration (courtesy of DTS, Glasgow).
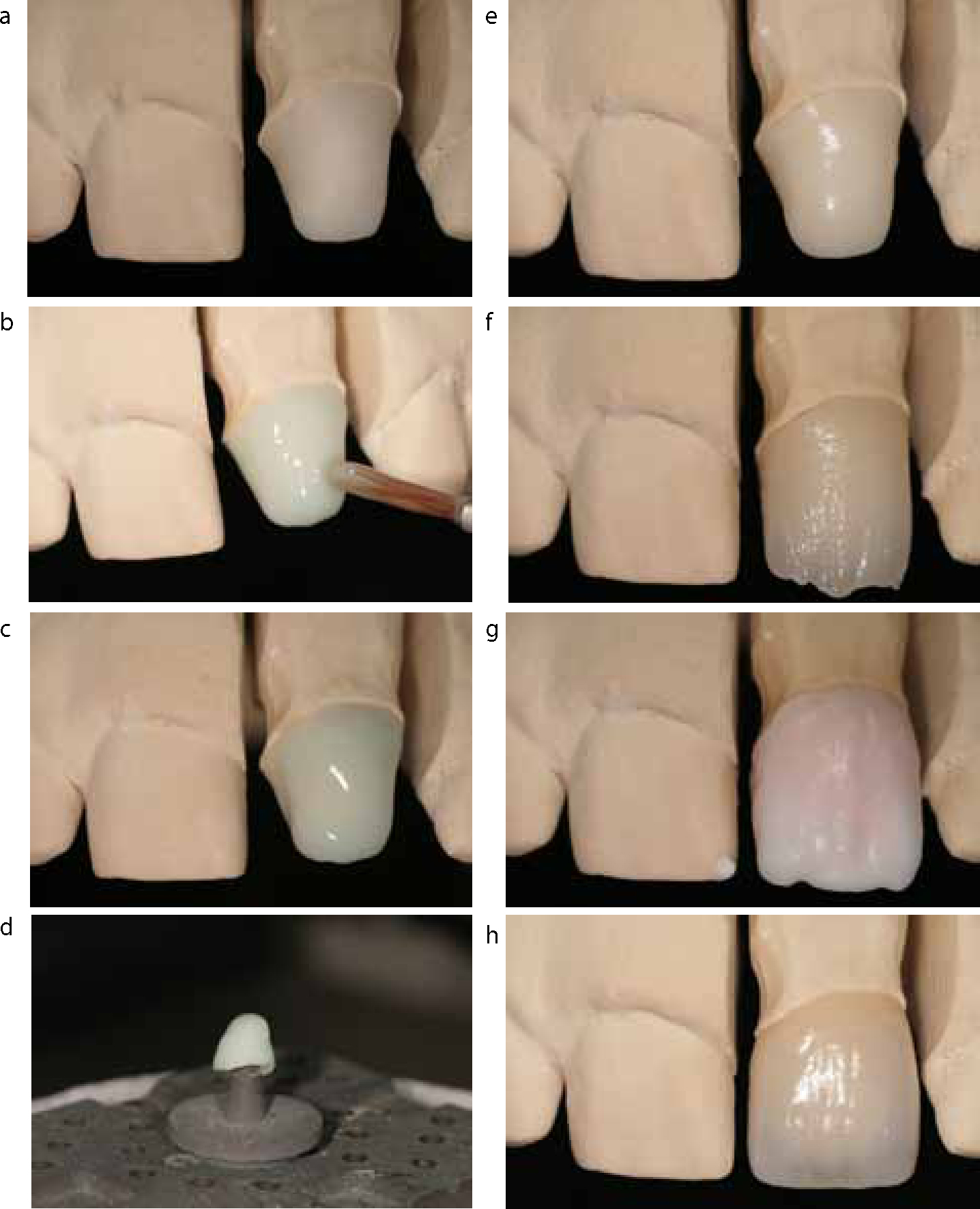
The material conventionally used for veneering zirconia cores is a feldspathic fluorosilicate porcelain which, following the application of a special liner, is incrementally layered and then sintered on to the coping (Figure 13 a–h).
Figure 13. (a–h) Conventional layering of a zirconia coping showing application of liner followed by build up with dentine and enamel shades (courtesy of Wayne Fleck, Vision Dental Laboratory).
Other methods can be used:
A fluorosilicate or a lithium disilicate veneer can be pressed over the zirconia. The latter has been shown to have significantly more favourable fracture toughness in comparison with the pressing or layering of any other type of ceramic.27 Pressing the ceramic does not provide the opportunity for the technician to generate individualized aesthetics. However, the ceramic can be pressed and then, using a cut-back technique, subsequently veneered with feldspathic porcelain.28 This double veneer does not alter the bond to the zirconia yet allows for improved aesthetics.
A one piece milled veneer can be constructed using CAD/CAM techniques. The Lava™ Digital Veneering System uses the full contour feature of the design software so that the glass ceramic porcelain and the zirconia coping are both milled to fit together perfectly. The veneer and coping are subsequently bonded to each other using a low-fusing glass ceramic (Lava DVS Fusion Porcelain). The restoration can also be characterized with the system's stains, shades and glaze.
Firing procedure
The veneering process involves a firing procedure at high temperatures at least once and usually between two to five times. Technicians should also be aware of methods used in the handling of veneering ceramic as they can increase or decrease the susceptibility to crack formation, eg multiple firings causing increased numbers of high expansion leucite crystals and an increased tendency to cracks.
In a study assessing the influence of repeated firings on a zirconia core, both the flexural strength and microhardness were reduced after the first firing. However, after subsequent firings they were not significantly different from the values achieved after just one firing and were not detrimental to fracture patterns, dimensions or surface roughness.29 It should be noted that firings should be carried out in a calibrated furnace, according to the manufacturer's recommendations, to limit large grain formation and produce a more homogeneous and smoother surface.
Bond of veneer to zirconia core
The bond between the veneering ceramic and zirconia core is extremely important as it will determine the overall strength of the restoration. The core is significantly stronger than the veneer and therefore can only impart support to the latter if a good bond exists.30 Studies have shown that zirconia crowns have greater stress at the interface between core and porcelain than alumina crowns and fail earlier in loading tests.16 Owing to these stresses, and the large differences in fracture toughness, veneer delamination fractures are likely to occur unless a good bond between the two components is achieved.31
Core liner
Prior to the application of veneering ceramic, some zirconia systems advise the application of a liner material. This is advocated to improve both the bond of the veneer to the core and the aesthetics of the core. Studies of this liner have shown that it can improve the bond strength of some veneering ceramics but can act as a weak point in others. A liner material should only be used with layered veneers, but not in combination with pressed veneers as it will result in weakening of the microtensile bond strength between the two.32 This data, however, is at odds with the recommendations of some manufacturers, demonstrating that application of liner prior to pressing is a controversial issue.
Bonding and cementation of the restoration
Bonding to the fitting surface of a zirconia restoration would be invaluable as it would allow adhesive prosthodontic techniques to be used, potentially conserving tooth structure, ie onlays as opposed to full coverage crowns.33 However, zirconia has a relatively inert surface and lacks silica which is required for bonding to the glass ceramics.
The use of airborne particle abrasion and a resin composite containing 10-methacryloyloxydecyl dihydrogen phosphate (MDP) [Panavia® F 2.0] is currently recommended.34 A similar protocol has been advocated by other authors based on in vitro comparative studies of microtensile bond strength.35 Abrading the surface of the zirconia through sandblasting or tribochemical coating (Rocatec, 3M ESPE) roughens the surface to increase the surface area for bonding. The phosphate ester group of MDP acts as an acidic monomer which chemically bonds to zirconia and other ceramics. This bond occurs with other metal oxides and it is assumed that it bonds to zirconia by the same method.
A form of tribochemical silica coating is available from 3M ESPE (CoJet®). This coats the surface of the ceramic in silica, thus allowing the use of a conventional silanating agent. In one study,36 this method was controlled for and tested with and without MDP/silane. Results showed that the CoJet® system increased significantly the shear bond strength between zirconium-oxide ceramic and a resin luting agent. Application of an MDP-containing bonding/silane mixture led to a further increase in bond strength. Bond strengths to zirconia can reach up to 22.9 +/- 3.1 MPa following ageing, whereas those commonly achieved with noble alloys are over 44 MPa following thermocycling.37
The current recommendations are clear. If there is adequate retention and resistance form of the tooth preparation, self-adhesive resin cement is recommended with light sandblasting of the zirconia fitting surface. If, however, resistance and retention form are poor, achieving the best bond becomes more critical. The zirconia fitting surface must undergo tribochemical silicatization, followed by application of an acidic primer, such as MDP, and finally a silane coupling agent. Resin cement can then be used in conjunction with appropriate bonding to tooth structure.
Reliable and improved bonding of zirconia ceramic would clearly be an advantage, but as yet there are no studies assessing the effects of these surface alterations on the zirconia's resistance to LTD. The clinical implications of this could be significant. Despite shortcomings in the resin bonding capability of zirconia, both manufacturers and clinicians continue to publish cases of resin-retained bridges constructed from a zirconia framework,38 albeit with limited success.39
Failure of zirconia restorations
A previously common cause of technical failure of all-ceramic restorations was bulk fracture. However this is relatively uncommon in zirconia prostheses. Review papers comment consistently that the most common cause of failure in zirconia restorations is veneer chipping or cracking.5,40–43 Veneer chipping has been documented at 13% at only 3 years.44 Many factors have been postulated as the cause of this chipping, such as:
Flaws in the veneering ceramic;
Differences in coefficients of thermal expansion;
Firing shrinkage of ceramic;
Poor wetting of the core by the veneer;
Thickness ratios or framework design.
However, specific veneering ceramics have been designed in order to combat these issues.
A number of research groups has conducted systematic reviews and meta-analyses looking at the longevity of fixed prosthodontics.40,42, 43,45–50 The results are outlined in Table 2. For restorations involving teeth, the most common complications were biological, such as secondary caries, 21.7%44 and loss of pulp vitality.42 This was similar for both metal-ceramic and all-ceramic fixed partial dentures. The technical complications told a different story, as framework or veneering ceramic fracture was significantly more common in all-ceramic restorations.47 Although ceramic chipping of metal-ceramic fixed partial dentures was more common when supported by implants,51 there are no studies which examine all-ceramic fixed partial dentures on implants, but it would seem reasonable to assume that these would have the highest rate of ceramic chipping. Framework fracture is uncommon in zirconia restorations.
Implant Supported (96.8% (5yr); implant survival at 5 years)
95.2% (5yr); 86.7% (10yr)
68.6%–94.3% (5yr); 88.9% (10yr)
94.5%– 95.4% (5yr); 89.4% (10yr)
91.2%
38.7% (5yr)
Combined Tooth-Implant Supported
95.5% (5yr); 77.8% (10yr)
Not applicable
Not applicable
20.6% (5yr)
The most frequent technical complications for all restorations were fractures of the veneer material, abutment or screw loosening and loss of retention.42 The frequencies of ceramic fractures (framework and veneer) were significantly (P < 0.0001) higher for all-ceramic FPDs compared with metal-ceramic.47 The fractures were mainly seen in the maxilla (75%), predominantly at the labial surface, and were associated with accidents, iatrogenic factors or surgical operations.52 Stress distribution maps of 3-unit FPDs have demonstrated that tensile stresses accumulate adjacent to connectors on their lingual side, thus having direct relevance to the possible site of veneer fracture.53
Other and future uses in dentistry
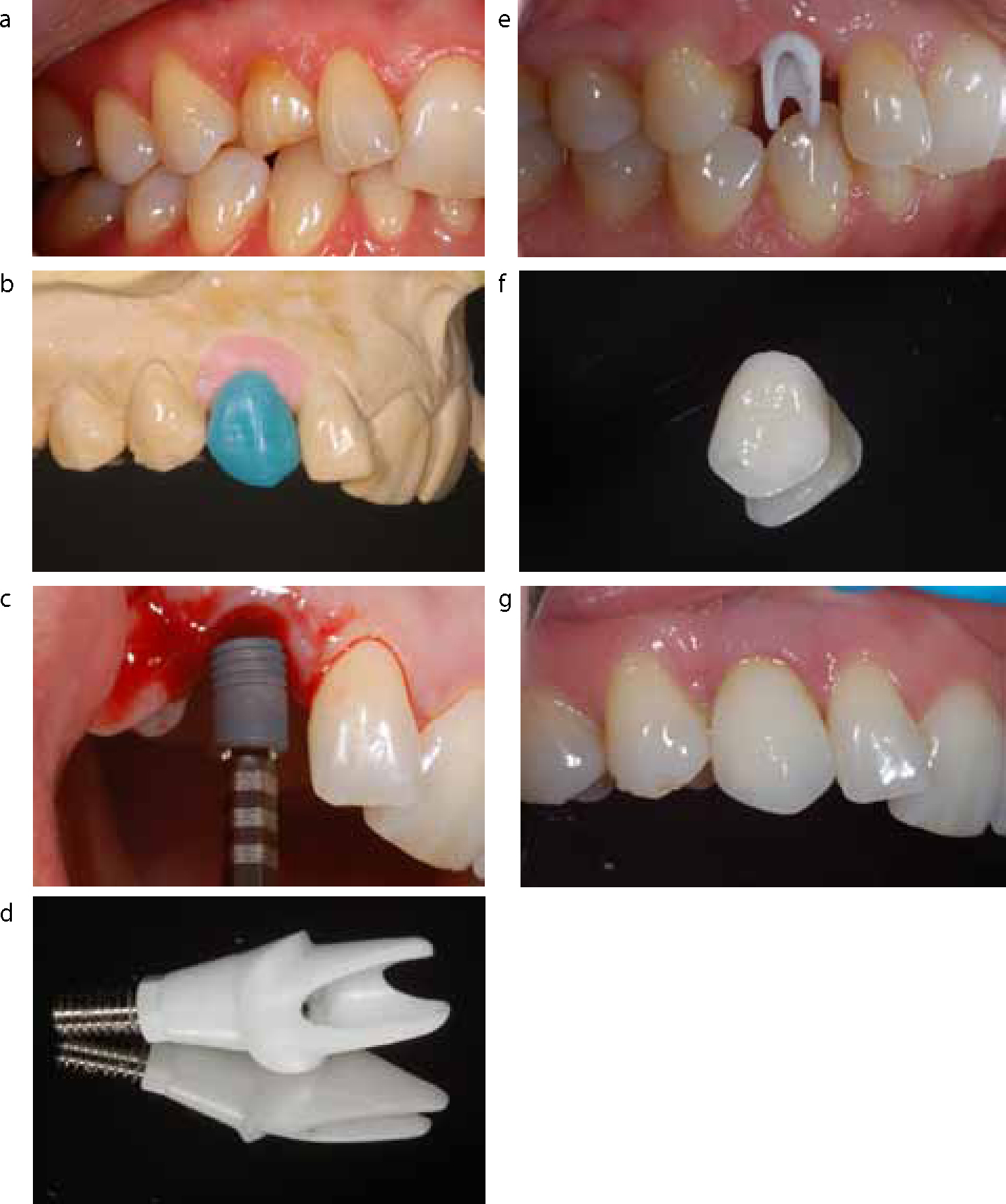
Zirconia is currently being marketed heavily for use with dental implants. It has well researched use as an implant abutment, with obvious aesthetic advantages (Figure 14 a–g). It is also marketed as an integral component of newer implants, such as Straumann's Roxolid™. This alloy of zirconium and titanium takes advantage of excellent biocompatibility to increase bone-to-implant contact compared with pure titanium controls.54 These may be the first steps towards a mainstream all zirconium dental implant. Such white implants are already marketed and clinical reports are available in the literature, however, they are still in their infancy compared with those made of titanium.
Figure 14. (a–g) Unaesthetic deciduous tooth restored with an implant-supported zirconia abutment and cement-retained zirconia crown.
Summary
Zirconia restorations show great promise as the future for all ceramic restorations. They have demonstrated excellent biological, mechanical and aesthetic properties. However, it is evident from clinical studies that some challenges remain. Inferior bond strength to tooth structure in comparison with modern glass ceramics significantly limits their clinical versatility. Veneer chipping is also of concern; this may not catastrophically affect survival rates but is of significance when considering the success of these expensive restorations. Although contemporary research appears to be focused in these areas, it is essential that both clinician and technician treat the material properly so as to achieve best results.
Conclusions
The use of zirconia in dentistry is still in its relative infancy and it should be noted that more long-term clinical data are required to reinforce initial findings.
Sintering of the zirconia framework should be carried out in a calibrated furnace using the manufacturer's recommended temperatures and times to limit large grain formation.
Light grinding and polishing of zirconia copings is recommended as opposed to rough polishing and sandblasting.
Choice and handling of a veneer for the framework are important so as to limit failure of the restoration.
Although bonding to zirconia is not yet comparable with bonding to glass ceramics or noble metals, should bonding be desired, it is advised that the surface undergoes tribochemical silicatization followed by application of an MDP primer and silane. The restoration should be cemented with resin cement for best results.