Hargreaves AS. Nylon as a denture base material. Dent Pract Dent Rec. 1971; 22:122-128
Matthews E, Smith DC. Nylon as a denture base material. Br Dent J. 1955; 98:231-237
Watt DM. Clinical assessment of nylon as a partial denture base material. Br Dent J. 1955; 98:238-244
Munns D. Nylon as a denture base material. Dent Pract Dent Rec. 1962; 13:142-146
Parvizi A, Lindquist T, Schneider R, Williamson D, Boyer D, Dawson D. Comparison of the dimensional accuracy of injection-molded denture base materials to that of conventional pressure-pack acrylic resin. J Prosthodont. 2004; 13:83-89
Kaplan P. Flexible removable partial dentures: design and clasp concepts. Dent Today. 2008; 27:120-123
MacGregor AR, Miller TPG, Farah JW. Stress analysis of mandibular partial dentures with bounded free-end saddles. J Dent. 1980; 8:27-34
Orr S, Linden GJ, Newman NH. The effect of partial denture connectors on gingival health. J Clin Periodontol. 1992; 19:589-594
Crissey JT. Stomatitis, dermatitis and denture materials. Arch Derm. 1965; 92:45-48
Tsuchiya H, Hoshino Y, Tajima K, Takagi N. Leaching and cytotoxicity of formaldehyde and methylmethacrylate, from acrylic resin denture base materials. J Prosthet Dent. 1994; 71:618-624
Masuki K, Nomura Y, Bhawal UK, Sawajiri M, Hirata I, Nahara Y, Okazaki M. Apoptic and necrotic influence of dental resin polymerization initiators in human gingival fibroblast cultures. Dent Mat J. 2007; 26:861-869
Hashimoto Y, Kawaguchi M, Miyazaki K, Nakamura M. Estrogenic activity of tissue conditioners in vitro. Dent Mat. 2003; 19:341-346
Gawkrodger D J. Investigation of reactions to dental materials. Br J Dermatol. 2005; 153:479-485
Gebhardt M, Geier J. Evaluation of patch test results with denture material series. Contact Derm. 1996; 34:191-195
Fisher AA. Allergic sensitisation of the skin and oral mucosa to acrylic denture materials. J Am Med Assoc. 1954; 156:238-242
Pfeiffer P, Rosenbauer EU. Residual methyl methacrylate monomer, water sorption, and water solubility of hypoallergenic denture base materials. J Prosthet Dent. 2004; 92:72-78
Pfeiffer P, Rolleke C, Sherif L. Flexural strength and moduli of hypoallergenic denture base materials. J Prosthet Dent. 2005; 93:372-377
Mante FK, Mante MO, Petropolous VC. In-vitro hardness of sealed resilient lining materials on immersion in various fluids. J Prosthodont. 2008; 17:384-391
Kiat-Amnuay S, Gettleman L, Mekayarajjananonth T The influence of water storage on durometer hardness of 5 soft denture liners over time. J Prosthodont. 2005; 14:19-24
Wright PS. The success and failure of denture soft-lining materials in clinical use. J Dent. 1984; 12:319-327
Polyzois GL. Adhesion properties of resilient lining materials bonded to light-cured denture. J Prosthet Dent. 1992; 68:854-858
Handa RK, Jagger DC, Vowles RW. Denture cleansers, soft lining materials and water temperature: what is the effect?. Primary Dent Care. 2008; 15:(2)53-58
Chander S, Hill M, Moore D, Morrow L. Tissue conditioning materials as functional impression materials. Eur J Prosthodont Res Dent. 2007; 15:67-71
de Souza RF, de Freitas Oliveira Paranhos H, Lovato da Silva CH Interventions for cleaning dentures in adults. Cochrane Database Systematic Rev. 2009; (4) https://doi.org/10.1002/14651858.CD007395.pub2
Ferracane JL. Hygroscopic and hydrolytic effects in dental polymer networks. Dent Mat. 2006; 22:211-222
Webb BC, Thomas CJ, Harty DW, Willcox MD. Effectiveness of two methods of denture sterilization. J Oral Rehab. 1998; 25:416-423
Chandra J, Mukherjee PK Antifungal resistance of candidal biofilms formed on denture acrylic in vitro. J Dent Res. 2001; 80:903-908
Verran J, Maryan CJ. Retention of Candida albicans on acrylic resin and silicone of different surface topography. J Prosthet Dent. 1997; 77:535-539
Chow CK, Matear DW, Lawrence HP. Efficacy of antifungal agents in tissue conditioners in treating candidiasis. Gerodontology. 1999; 16:110-118
Pavan S, Filho JNA, Dos Santos PH, Nogueira SS, Batista AUD. Effect of disinfection treatments on the hardness of soft denture liner materials. J Prosthodont. 2007; 16:101-106
Kuhar M, Funduk N. Effects of polishing techniques on the surface roughness of acrylic denture base resins. J Prosthet Dent. 2005; 93:76-85
Monsenego P. Presence of microorganisms on the fitting complete denture surface: study in vivo. J Oral Rehab. 2000; 27:708-713
O'Donnell EF, Radford DR Chairside polishing of heat-cured acrylic resin: an SEM and EDA study. Int J Prosthodont. 2003; 16:233-238
Provision of partial and complete dentures constructed from resin is commonplace and a satisfactory outcome requires the consideration of the properties of the resin, the oral tissues and prosthodontic principles. This second of a two-part series examines the advantages and disadvantages of flexible nylon denture base resins, which have found popularity for the provision of partial dentures. Adverse effects of denture base resins are examined and the benefits and shortcomings of softliners are explored. Chairside adjustment and polishing, and denture hygiene are also discussed.
Clinical Relevance: Knowledge of contemporary denture base resin systems will help to achieve optimal outcomes in removable prosthodontics.
Article
Increasingly, dental patients are retaining their teeth, owing in large part to improved oral health awareness. Those patients who are unfortunate enough to lose teeth often enquire about the possibility of replacing missing teeth with fixed prostheses which, as a result of implant therapy, is increasingly possible. However, there remains a demand for ‘simple’ removable dentures by a significant proportion of patients who are completely or partially edentulous. These are most commonly made either entirely of acrylic, or may consist of acrylic saddles on a cobalt chromium framework, in the case of partial dentures. Acrylic has a good track record and fulfils many of the ideal properties of a denture base material but its use is a compromise. A number of its benefits and shortcomings were discussed in part one of this series and others, such as soft-lining acrylics and the potential of acrylics to cause adverse effects, are examined in this second section. However, we begin by exploring the use of flexible nylon denture base resins as an alternative to hard acrylic.
Flexible partial dentures
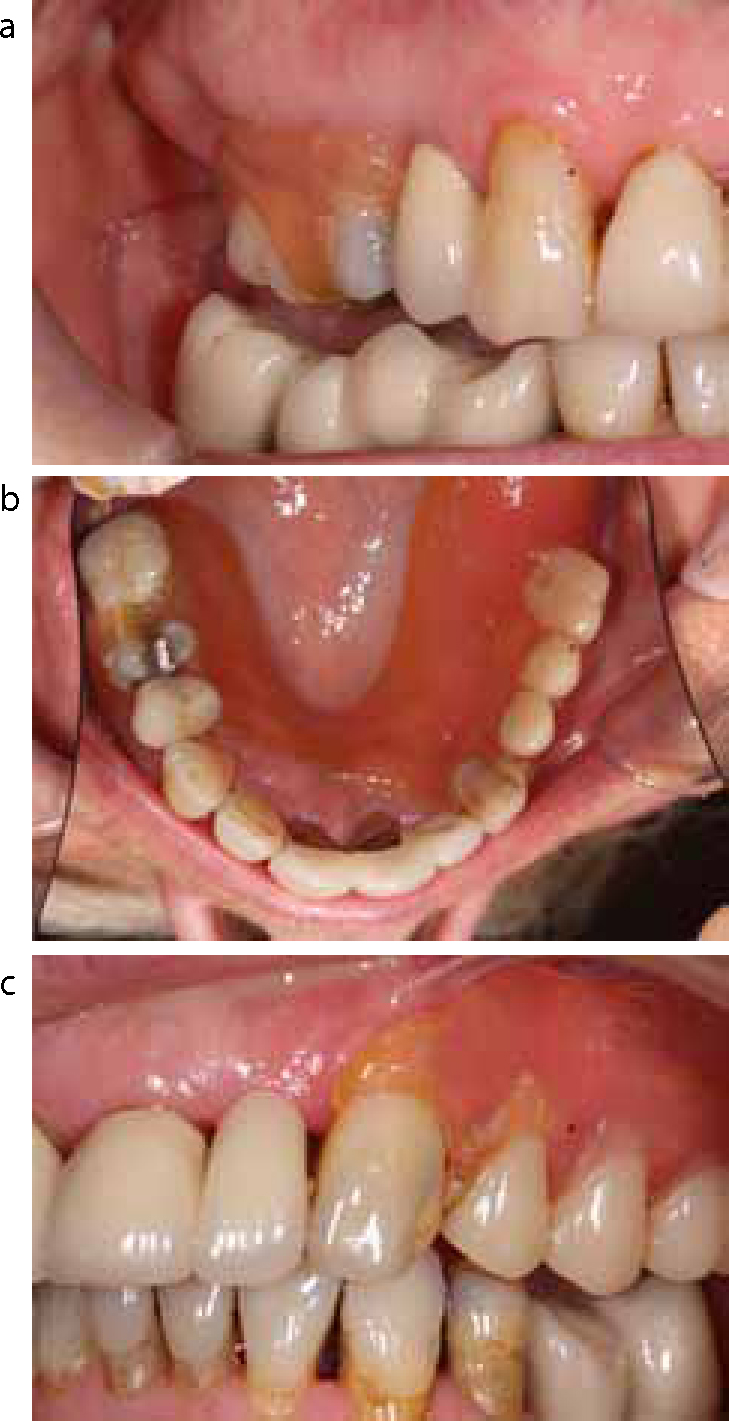
Nylon denture base resins first became available in the 1950s and have recently found some popularity in the UK for the fabrication of partial dentures. Nylon's flexible nature facilitates the manufacture of both the denture base and the tooth clasps form a ‘monoblock’ of the material (Figure 1). Flexible partial dentures appear to be readily accepted by patients owing to their light weight, flexible nature and the provision of clasps that are a similar colour to the gingivae as opposed to metal. However, their use does raise some clinical concerns.
Figure 1. (a) A flexible (Sunflex, Sun Dental Labs) partial denture. (b, c) Typical clasp designs for flexible partial dentures.
Nylon was developed by Wallace Carothers and associates, of the Du Pont Chemical Co, in the 1930s, and is a generic name for certain types of thermoplastic polymers belonging to the class known as polyamides. These polyamides are produced by the condensation reactions between a diamine and a dibasic acid. The manufacturers of modern dental nylon systems, such as Valplast (Valplast International Corporation, Long Island City, NY, USA), Sunflex (Sun Dental Labs LLC, Clearwater, FL, USA) and Lucitone FRS (Dentsply Trubyte, York, PA, USA), recommend their use for the fabrication of partial dentures and small to medium-size complete dentures.
Generally, the properties of nylon are determined by the number of –CH2 – groups in the diamine chain and the number of carbon atoms in the dibasic acid chain, which together also determine the prefix of the nylon. More details on the classification of nylons studied for dental use can be found elsewhere.1 The manufacturers of contemporary nylon denture base materials have not divulged the type of nylon or additives in their formulations. However, to date, nylons which have been investigated in the literature for denture bases are nylons 66, 610, 11, 12, and combinations of these. Although gaining popularity as a convenient ‘flexible’ partial denture base, there are surprisingly few investigations in the literature of its use as a denture material.
Accuracy and stability of nylon
Nylon was initially studied as a denture base material in the 1950s but not recommended for general use at that time. Early nylon dentures exhibited high processing shrinkage resulting in warpage and high water sorption leading to rapid discoloration, loss of surface finish, swelling and softening.2–4 However, the conditions in which these dentures were processed were far from ideal. In 1971, the investigations of Hargreaves on nylon resulted in guidelines for its optimal application as a denture base material.1 These guidelines are emulated in the processing of modern nylon systems using specialized laboratory equipment. Consequently, on completion of the wax try-in stage, some commercial laboratories send nylon denture work on to another laboratory with the necessary processing equipment and expertise.
The importance of correct processing cannot be underestimated. In 2004, Parvizi et al investigated the dimensional accuracy of Valplast and reported the processing shrinkage to be 2.8 times greater than a conventionally processed acrylic denture.5 However, similar to the early nylon denture base studies, Parvizi used a cold denture mould, which is known to lead to exaggerated polymerization shrinkage, and a moist flask, which would be expected to affect dimensional change as nylon is a hydrophilic material. It is clear that the physical characteristics of nylon denture bases are extremely sensitive to processing techniques and further investigations are required to establish the accuracy and survivability of these ‘flexible’ denture bases in clinical practice (Figure 2).
Figure 2. (a, b, c) A flexible partial denture in service.
Are nylon dentures unbreakable?
Although the modulus of rupture of glass-filled nylon 12 is similar to that of denture base acrylic, nylon's lack of notch sensitivity and its toughness are claimed to render it virtually unbreakable under service conditions. This is perhaps reflected by the life-long ‘no breakage’ guarantee offered by Valplast and a similar 5-year guarantee on Leucitone FRS (Dentsply Trubyte, York, PA, USA) denture bases.
Is flexibility an advantage or a disadvantage?
Advantages of flexible dentures
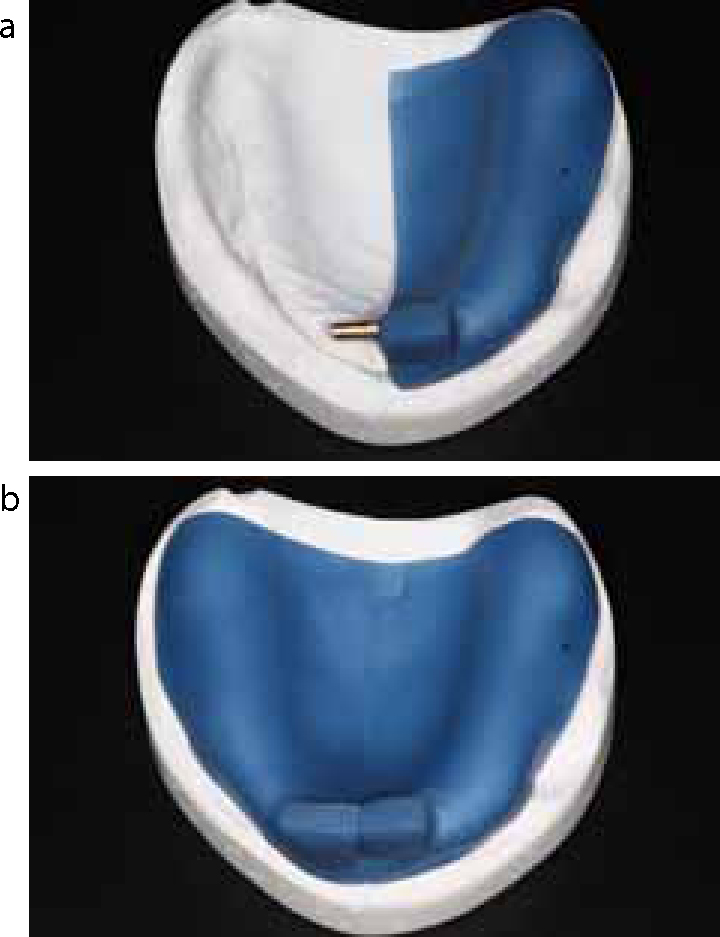
A flexible denture base does offer a number of advantages, for example in the management of patients who suffer from severely limited mouth opening due to conditions such as scleroderma and subsequent to reconstruction following ablative surgery in oncology cases. A flexible denture would be easier to place and remove for such patients, with the main challenge being to obtain a satisfactory master impression, perhaps requiring a 2-part special tray (Figure 3). The design of flexible partial dentures is easy owing to retention being obtained by simply extending the baseplate around undercuts of the abutment teeth immediately adjacent to the saddle(s), and patient acceptance appears to be high. Small sectional designs are possible, although their use should be carefully considered as their size may, in some cases, present a risk to the airway if they become dislodged. A guide to clasp design for flexible partial dentures has been published6 and involves either ¾ or circumferential coverage of the abutment tooth (Figures 1, 2 and 4). The flexibility of nylon facilitates extension of denture bases around bony undercuts and into interproximal spaces, without blocking these areas out on the master cast, both gaining retention and simplifying laboratory procedures. The presence of metal clasps, which can be objectionable to some patients, is avoided and the laboratory procedures are quicker and simpler than the construction of a cobalt chromium framework.
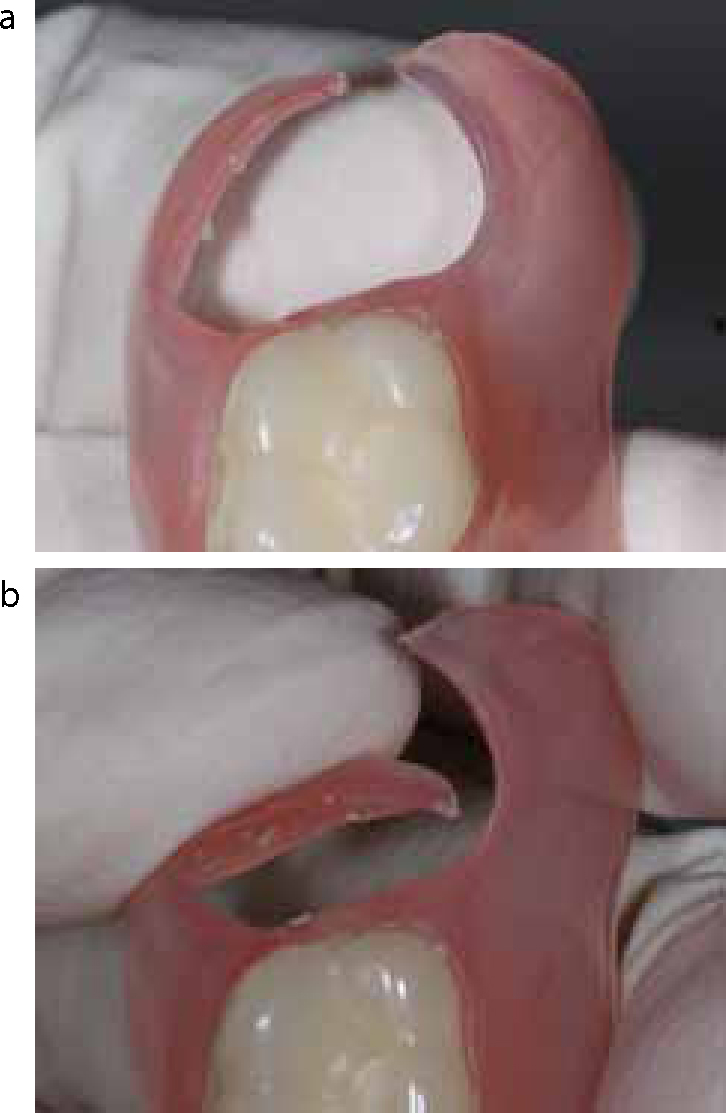
Figure 3. (a, b) A two-part special tray.Figure 4. (a, b) Demonstrating degree of flexibility of flexible denture clasp.
Disadvantages of flexible dentures
Flexible dentures also carry a number of disadvantages, owing both to the distribution of forces within a non-rigid material and design features synonymous with flexible partial dentures. Any possible changes in the shape of a denture base are important to the teeth and the tissues that come into immediate contact with the denture.
If a denture base is rigid, under occlusal loading, the forces are distributed evenly throughout the material. For example, an occlusal force on the working side of a rigid denture results in both a positive force pressing the denture base into the supporting tissues on that side and, on the non-working side, a negative force tending to raise the prosthesis, countered by suction (in the case of a complete denture) or clasps (in the case of a partial denture). Increasing flexibility of the denture base results in a decreasing counter or balancing force, resulting in less even distribution of the forces over all the tissues covered by the denture.
When considering a partially dentate arch with a bounded saddle, it has been shown that, by means of occlusal rests and using a rigid denture material (typically cobalt chromium), the masticatory force is distributed over the abutment teeth and the alveolar ridge through the denture saddle.7 As with acrylic, nylon cannot be used to construct occlusal rests and, therefore, flexible partial dentures are entirely mucosal-borne. This introduces the risk of gingival recession and clinical attachment loss – ‘gum stripping’. Although mucosal-borne acrylic partial dentures are ‘rigid’ enough to obtain some tooth support if they are finished above the survey line of teeth they contact, this is not a possibility with flexible dentures. Additionally, masticatory force on a flexible saddle produces a heavier pressure on the underlying ridge than if the base is inflexible. This is because the distribution of the force transmitted to the underlying mucosa is dependent on the elasticity of the material used as well as the length of the saddle.7 Essentially, the elasticity of flexible denture bases results in the masticatory pressure acting on a limited area of the alveolar ridge, as opposed to distributing forces more evenly, including to teeth and the primary support areas (see part one of this series), increasing the risk of resorption.
When the saddle(s) and connecting plate of a flexible denture bends, the clasps on the teeth must shift, with the result that torquing forces would be expected to act on the abutment teeth. It is not known if the clasps of nylon denture systems are flexible enough to avoid torquing of abutment teeth, which could eventually lead to tooth movement and periodontal complications. Similar problems could arise should a flexible denture not return exactly to its original form after bending, although this problem has not been reported with contemporary nylon systems.
Although denture base nylon is strong and can be used in thin sections, in order to be ‘stiff’ enough for their respective functions, connectors and clasps need to be sufficiently wide. As a result, flexible partial dentures do not facilitate the principle of keeping gingival margins clear. Their clasps and reciprocating arms cover a large surface area, including gingival margins and more tooth tissue than metal clasps, raising concerns regarding plaque control and periodontal inflammation. Avoiding gingival contact by blocking out the dento-gingival region in areas where they are covered by a denture does not appear to offer any periodontal protection.8 Changes to the underlying tissues and to the denture base will consequently also affect the relationship of the occlusal surfaces of the denture teeth to the opposing teeth. This is likely to impact upon masticatory function and, in the longer term, potentially the positional stability of opposing teeth.
Adverse effects of denture base resins
Adverse reaction to denture base resins appears to be uncommon, yet residual monomer and additives of denture base acrylic have the potential to cause allergy, irritation, cytotoxicity and unwanted biological effects. Nylon (see above) or other hypoallergenic materials (which will be discussed) appear to offer an alternative, but their use is associated with other clinical concerns. To place the adverse effects of denture base acrylic into perspective, it is worth remembering that poor fit and poor denture hygiene are the main causes of soreness beneath dentures. Additionally, residual monomer, which is the allergen and major irritant present in denture base acrylic, typically constitutes around 0.3% of heat-processed acrylic and most of this is lost within 12 hours of use.9
Effect of biodegradation products
In the oral environment, repeated occlusal loading, food and drink, thermal changes and the water and enzyme constituents of saliva result in a degree of biodegradation of denture base materials. Biodegradation of denture base acrylic results in diffusion of residual monomer and additives out into saliva, which further biodegrades the denture base via enzymatic attack on polymer side-chains. As well as allergy, residual or released monomer has the potential to cause direct toxicity or to produce formaldehyde by reacting with molecular oxygen, which is cytotoxic at much lower concentrations.10 Benzoyl peroxide, used as an initiator in the polymerization of denture base acrylic, and phthalate esters, used as plasticizers, are also released by biodegradation. Both of these additives have the potential to contribute to chemical irritation of the oral mucosa, which could lead to oral ulceration or burning mouth syndrome, and benzoyl peroxide can induce necrosis in gingival cells.11 Phthalates (and other esters of aromatic carboxylic acids used as plasticizers) released from denture base acrylic are noted for their oestrogenic activity12 and are present in particularly large concentrations in some acrylic-based soft lining resins for dentures. Fortunately, in most cases, the biodegradation of heat-cured denture base acrylic is probably of little clinical significance except as a cause of wear and denture fracture, mainly due to repeated occlusal loading.
Allergy to denture base acrylic
Although uncommon, contact stomatitis to denture base acrylic does occasionally occur.13 Acrylic allergy usually relates to residual monomer, however, it has been speculated that additives, such as the initiator benzoyl peroxide, and pigments may sometimes be present in sufficient concentration to cause unfavourable tissue reactions.14 The rarity of allergy to denture acrylic may, in some part, be explained by the conditions present in the oral environment which help to prevent prolonged contact of the oral epithelium with potential allergens: the highly vascularized oral mucosa leads to rapid absorption and has a relatively low density of T cells and Langerhans cells, and the saliva has a diluting and washing effect.
Although hand dermatitis could present amongst dental professionals owing to inappropriate direct handling of monomer liquid, patients present with oral signs and symptoms such as irritation and erythema of the denture-bearing area. These may be non-specific and difficult to distinguish from irritative contact from ill-fitting dentures or candidiasis. Other physical signs of contact stomatitis are lichenoid reactions, angular cheilitis, swollen lips, recurrent aphthous ulceration and oral granulomatosis. However, symptoms are often more prominent than physical signs and can include burning mouth syndrome, loss of taste, numbness or soreness.
A definitive diagnosis is usually reached following patch testing, which involves the adhesion of test substances in the acrylate series to the skin for 48 hours. The skin is then examined to identify to which allergens the patient is sensitive. It may be necessary to use an alternative denture base resin in patients with confirmed allergy to denture base acrylic. However, increased risk of allergy has been associated with inadequately polymerized acrylic and patients known to be allergic to methylmethacrylate (MMA) monomer may tolerate acrylic dentures that have been adequately heat-cured and are free from any autopolymerizing acrylic repairs or reline materials.15
Hypoallergenic denture base resins
On the occasion that a clinician may be presented with a patient with a proven allergy to some component of denture base acrylic, hypoallergenic denture base materials are available, such as MMA-free modified methacrylates, for example Eclipse (Dentsply Trubyte, York, PA, USA). There are also methacrylates available which have significantly lower residual monomer compared to polymethyl methacrylate–based acrylic, such as Polyan (Lewepharm, Gaweinstal, Austria) and Sinomer (Alldent, Veenendaal, Netherlands).16 In addition, alternatives to methacrylates are available. Alternatives to methacrylate include a variety of materials, with a number of manufacturers producing nylon denture base materials (as previously discussed) and the availability of enterephthalate-based (Promysan, Pedrazzini Dental Technologie, Ottobrunn, Germany) and polyurethane-based (Microbase, Degudent, Hanau, Germany) materials. The flexural strength of Polyan (Lewepharm) and Promysan (Pedrazzini Dental Technologie) has been shown to be comparable to heat-cured acrylic, and that of nylon to be superior.17 However, the clinical properties of all the materials presented in Table 1 require further investigation.
There are two types of soft liner currently available; highly plasticized acrylic and silicone rubber. Resilient soft liners placed on the impression surface of a hard acrylic prosthesis can provide a visco-elastic ‘cushion’, and such materials are often incorrectly viewed as a panacea in difficult complete denture cases. Further examination of the properties of these materials highlights their shortcomings and the importance of limiting their use for successful long-term prosthodontic outcomes. The intrinsic properties of soft liners (see below) make them at best semi-permanent and, as such, the decision to incorporate them into a denture design should be a carefully considered one. The only clear-cut indications for their use are for the engagement of undercuts and cushioning underlying sharp and uneven edentulous ridges when selective pressure impression techniques or relief of the impression surface of the denture have been exhausted. Several soft relining materials are presented in Table 2 and include chairside materials, such as Coe-Soft (GC Co, Tokyo, Japan), and others such as Molloplast B (Detax, Ettlingen, Germany), which are placed in the dental laboratory.
Soft Liner
Manufacturer
Material
Longevity
Eversoft
Dentsply
acrylic
semi-permanent
GC Tissue Conditioner
GC Europe
acrylic
semi-permanent
GC Reline Soft
GC Europe
silicone
semi-permanent
GC Soft Liner
GC Europe
acrylic
3-4 weeks
GC Coe-Soft
GC Europe
acrylic
3-6 months
GC Coe-Comfort
GC Europe
acrylic
1-2 weeks
Luci-Sof Soft Denture Liner
Dentsply, Trubyte
silicone
semi-permanent
Molloplast B
Detax GmbH & Co.
silicone
semi-permanent
Tokuyama Sofreliner Tough
Tokuyama Corp.
silicone
semi-permanent
Visco-Gel
Dentsply, Trubyte
acrylic
short-term
Biodegradation
Of particular importance when considering the use of soft lining materials is their biodegradation, which results in hardening or softening (dependent upon their exact constituents), staining and roughening within several months of service (Figure 5).
Figure 5. A soft liner following several years in service.
Acrylic resin soft lining materials are based on either methyl, ethyl or butylmethacrylate, with high concentrations of phthalates or other esters of aromatic carboxylic acids present as plasticizers to soften the material adequately, for example Coe-Soft (GC Co) contains dibutylphthalate (21%). These plasticizers leach out into the aqueous oral environment, resulting in hardening of acrylic soft liners to the extent that their visco-elastic properties are eventually lost. Further to the deterioration in the properties of soft liners, leaching of their plasticizers can also result in a bitter taste. More concerning are the oestrogenic properties of phthalates, or other esters of aromatic carboxylic acids, which have the potential to induce undesirable biological effects.12 Although leaching from acrylic soft liners may be reduced by the use of a vinyl polymer coating, such as Permaseal (Austenal Inc, Chicago, USA),18 or by incorporating forms of methacrylate which copolymerize but do not leach out,19 silicone soft liners, such as Molloplast B (Detax, Ettlingen, Germany) have become increasingly popular.
Delamination
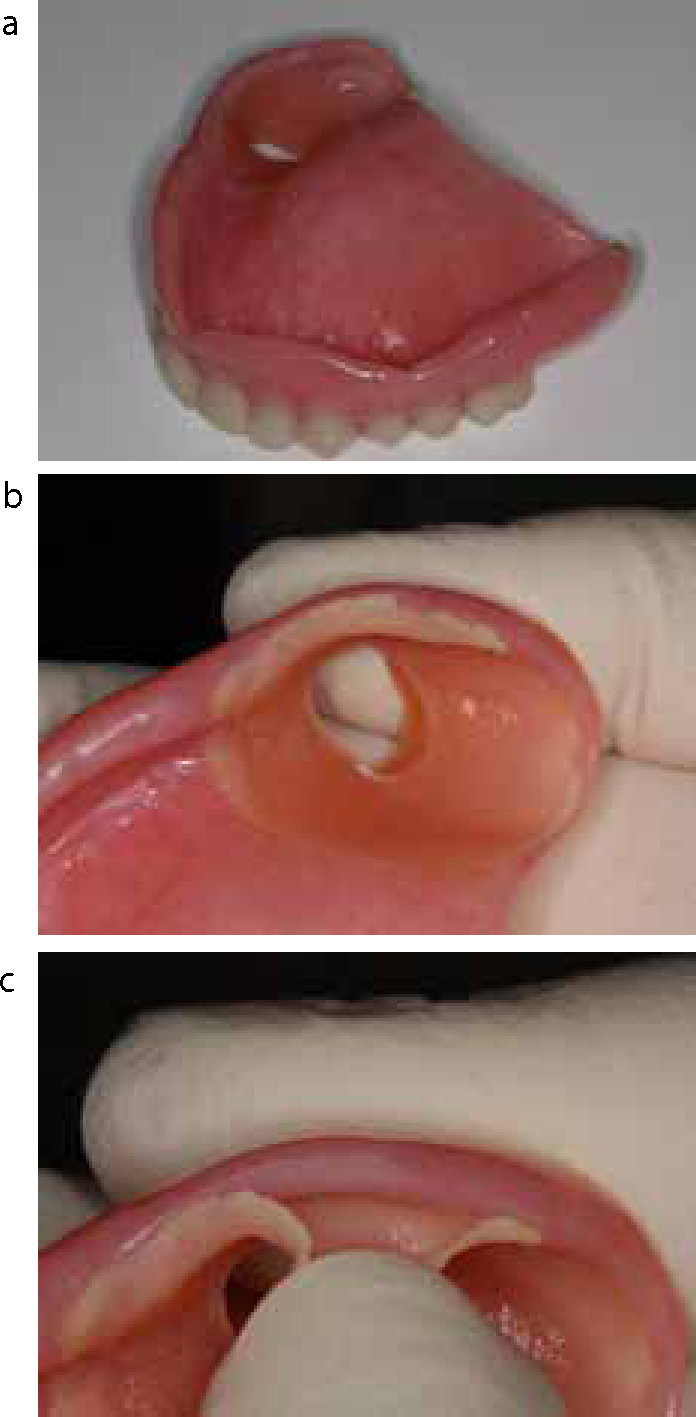
Silicones like Molloplast B retain their resilience better than acrylic resin-based lining materials because softness is an intrinsic property. However, their water uptake is high owing to their filler content and their survivability is commonly compromised by the failure of their adhesion to the heat-cured PMMA denture base during service20 (Figure 6). Their bond to acrylic resin dentures is achieved via an intermediary, such as a silicone polymer in a volatile solvent or the use of alkylsilane bonding agents. Stress occurs at this bond as a result of swelling when the silicone rubber absorbs water from the saliva, eventually resulting in failure of the bond21 which usually begins at the denture border. Staining at this site may be the first clinical observation but bond failure will harbour unwanted micro-organisms, accumulate unwanted debris and ultimately lead to complete delamination. Acrylic-based soft liners are not immune to the problem of delamination, particularly when based on ethyl or butylmethacrylate as opposed to methylmethacrylate. Like resilient silicone liners, acrylic-based soft liners swell due to water sorption producing stress at the bond site, which is subject to increased external loads as plasticizer is lost and the lining material becomes brittle. In addition to areas of partial delamination which can harbour unwanted micro-organisms, the surface of soft lining materials appears to become colonized by yeast and bacteria more readily than conventional denture base acrylic. Soft liners can therefore pre-dispose to candidal infection and it has been suggested that continuous aspiration/inhalation of micro-organisms from the denture plaque can expose medically compromised patients to a greater risk of systemic disease.22
Figure 6. (a) Acrylic denture with a window of soft liner engaging the undercut at a lone standing molar. (b, c) Partial delamination of silicone soft lining material.
Tissue conditioners
On occasion, resilient soft materials can also be helpful used as tissue conditioners in existing complete denture wearers. Visco-Gel (Dentsply Trubyte, York, PA, USA) is a common example of a tissue conditioner, placed chairside to improve fit temporarily and to ‘cushion’ an existing denture in order to relieve inflammation and trauma of the underlying soft tissues prior to the provision of a new prosthesis. Visco-Gel (Dentsply) may also be used to make functional impressions, a description of which can be found elsewhere.23
Denture hygiene
Effectiveness of denture cleansers
Similar to the natural dentition, dentures acquire a pellicle and subsequently plaque and calculus can accumulate. Poor denture hygiene places the underlying tissues at risk of stomatitis, caries and periodontal disease and patients may complain of malodour or poor appearance. Provision of any denture to a patient should naturally be accompanied by advice on how to clean the prosthesis. A recent meta-analysis found that active cleaning is to be recommended over passive cleaning.24 Effective active methods are brushing (with a proprietary non-abrasive paste, for example Dentu-Crème, GlaxoSmithKline, Middlesex, UK), or use of a sonic bath (for example Sonic Denture Cleaner, DentaNurse, Herefordshire, UK) with a cleaning solution. Passively soaking dentures in a cleansing solution such as Steradent (Reckitt Benckiser, Berkshire, UK) or Milton solution (Proctor & Gamble, Cincinnati, Ohio, USA) is unlikely to remove plaque and microbes as effectively.
Adverse effects of denture cleansers
Proprietary denture cleansers for immersion are solutions of chemical agents, such as sodium hypochlorite, alkaline glutaraldehyde, aqueous formaldehyde, or enzymatic solutions. Chemical disinfection has the potential to alter the surface and structure of denture base resins because of polymer solubility or water sorption from immersion solutions.25 However, the effects of these are generally clinically insignificant for acrylic resin dentures in popular commercial solutions. The manufacturers of some flexible (nylon) denture bases suggest their own immersion formulations, such as FDC Flexible Denture Cleaner (Valplast International Corporation, Long Island City, NY, USA) (Figure 7) to reduce the risk of unwanted changes to the properties of the denture.
Figure 7.
Flexible Denture Cleaner (Valplast International Corp).
Microwave disinfection of acrylic dentures has been suggested for cases of candidal infection as it is particularly effective at reducing candida albicans colonization by promoting irreversible changes in cell morphology.26 The technique involves placing the denture in distilled water and subsequently microwaving it at 650W for approximately 6 minutes. This method has not gained popularity not least because of the inherent danger of scalding, but also as a result of dimensional changes brought about within the denture by the repeated use of this method.
Denture stomatitis
The occurrence of chronic atrophic stomatitis beneath the fitting surface of a denture is not uncommon. Its clinical appearance of a well-demarcated area of erythema corresponding to the fitting surface of an upper denture is usually diagnostic, although a gram-stained smear displaying candidal hyphae taken from the lesion could be used to confirm the diagnosis (Figure 8). Angular stomatitis may also be present. The first step in the onset of denture stomatitis is the adhesion of Candida species to the fitting surface of denture base acrylic, either directly or through denture plaque. This unpolished relatively rough surface of the denture facilitates the retention of micro-organisms and may serve as a reservoir: the surface irregularities present can protect micro-organisms from the shear forces produced when brushing the denture and allow them time to become irreversibly attached to the surface.27
Denture stomatitis often resolves following appropriate antifungal treatment, such as wearing the denture with a thin coat of miconazole gel on the impression surface (applied 4 times each day for 7–14 days), and improved denture hygiene. However, for the reasons discussed above, it may be necessary to replace old dentures that have suffered surface deterioration due to biodegradation and could act as a reservoir for Candida species. Persistent Candida infection may indicate poor patient co-operation or an underlying systemic condition, such as iron deficiency or immunosuppression, which are beyond the scope of this article.
Soft lining materials are particularly prone to microbial adhesion because of their relatively highly porous surface texture and the physical/chemical affinity between micro-organisms and the materials.28 Adhesion of fungi promotes the deterioration of soft liners via the release of toxins and metabolic products, and Candida species can become entrapped in surface irregularities, predisposing to re-colonization after cleaning. Attempts to incorporate anti-fungal agents within soft lining materials have been unsuccessful29 owing to their leaching out and dilution by saliva and the countering effect of the nutrient-rich oral environment. Although the need for thorough cleaning of soft liners is clear, this is also problematic as they exhibit problems associated with water absorption, which results in changes in their structure and properties, such as loss of softness, distortion and surface deterioration.30 Some manufacturers of soft lining materials recommend using a sponge, as opposed to a brush, for cleaning which may avoid roughening the surface, but is likely to result in less thorough cleaning.
Chairside adjusting and polishing
Denture base acrylic
It is often necessary to adjust dentures in the dental surgery to relieve areas of overextension or excessive pressure, which can cause instability and soreness. For acrylic, this is routinely carried out with tungsten carbide burs with a universal cross-cut blade pattern in a straight handpiece at 10,000–15,000 revolutions/minute. Tungsten carbide trimming burs are available in various diameters and their blades can range from ‘extra coarse’ to ‘super fine’. Unfortunately, whichever tungsten carbide bur is selected, its use will result in the unwanted effect of roughening that area of the denture, even if used in conjunction with a polishing cream.31 Dental laboratories achieve a highly polished outer surface for dentures, typically by polishing with water and fine pumice followed by polishing with an aluminium oxide polishing paste. However, most dental practices do not have a laboratory polishing lathe on site and, therefore, chairside polishing systems are available which are able to produce results approaching that of a laboratory finish. Their use is clinically important because roughened outer surfaces of a denture may cause a patient to complain of discomfort and will encourage the retention of denture plaque and micro-organisms. The fitting surface of dentures is not polished to retain an accurate fit and, although this surface can be colonized with micro-organisms, it is considered that the effect of surface roughness on microbial adhesion is much smaller in the unique environment beneath a denture.32
AcryPoint (Shofu, Kyoto, Japan) is a typical chairside polishing kit for acrylic dentures, consisting of silicone points in three different grits. Polishing should be carried out in a systematic manner gradually eliminating the rough surface layers, beginning with the coarse point and finishing with the fine point. Although multi-step systems may seem laborious, they result in a significantly smoother finish than polishing with a single silicone point,33 and it is not necessary to use a polishing paste. However, use of a polishing paste such as Becht Polishing Cream (Alfred Becht GmbH, Offenberg, Germany) may be useful when using a single or two-step system, for example Kenda-Queen (Kenda, Vaduz, Liechtenstein), where the final polishing point is medium as opposed to fine. It is worth bearing in mind that the greater porosity of autopolymerizing acrylic resin results in reduced polishability and a rougher surface of repaired or chairside relined areas of acrylic dentures.
Soft liners
Soft lining materials (both acrylic and silicone) for hard acrylic dentures require special consideration when adjustments are to be made. It is accepted that their surfaces are inherently rougher than hard acrylic and, therefore, a highly polished surface cannot be achieved. Use of conventional tungsten carbide rotary instruments can cause surface smearing and heat development, which can lead to separation of the soft liner from the denture base. The manufacturers of these materials produce their own instruments for adjusting and ‘polishing’. For example, the chairside silicone soft reliner Sofreliner Tough (Tokuyama, Tokyo, Japan) can be supplied in a kit containing an adjustment point and a finishing point. Similarly, Molloplast Cutters and Molloplast Pre-Polishers are available from Detax for the adjustment of the laboratory-placed soft reliner Molloplast B (Detax, Ettlingen, Germany).
Flexible dentures
Although they are flexible, nylon dentures, such as Sunflex, can cause persistent irritation of the oral mucosa due, for example, to an over-extended impression. As well as roughening the surface, an additional problem with the adjustment of nylon (flexible) dentures is threading of the material. The manufacturers of nylon flexible denture systems produce their own advice and burs for the adjustment of their dentures. Tungsten carbide burs are better avoided for nylon denture bases. Sunflex (Clearwater, FL, USA), for example, produce Sunflex Brown Rubber Points which they recommend to be used at low speed with a light back and forth motion. Any fibres that appear through threading of nylon should be removed with a scalpel blade. If a flexible partial denture clasp is too tight or too loose, the manufacturers of these materials recommend adjustment by a 30 second immersion in hot water and then bending the clasp in the required direction.
Summary
Flexible nylon denture base resins are available which, on the face of it, appear to offer a number of advantages. Used as a material for partial dentures, the base and clasps are fabricated from a monoblock of the material, offering simple design and fabrication. Patient acceptability can be good because of nylon's lightweight nature and clasps which are a similar colour to the gingivae. However, clasp designs possible with current flexible partial denture systems cannot facilitate relief of gingival margins, and a flexible denture base can lead to undesirable distribution of occlusal loads to the underlying tissues. These clinical conditions carry an increased risk of gum-stripping and accelerated resorption of the underlying residual ridge. When adjusting and cleaning flexible partial dentures, the best results are likely to be obtained using the cleaning solutions and adjustment burs provided by the respective manufacturer.
Most dentures continue to be constructed from hard denture base acrylic. Although the material is a compromise, especially when used for partial dentures without an underlying cobalt chromium skeletal framework, it is hard enough to distribute occlusal loading evenly and to facilitate partial denture designs that offer some relief of gingival margins. Biodegradation products of acrylic denture base resins have the potential to produce unwanted biological effects and can be associated with allergy, but the incidence of adverse effects is low. Soft lining materials for hard acrylic are sometimes incorrectly seen as a panacea in difficult complete denture cases, but their use should be limited owing to considerable problems related to their longevity. Soft liners are at best semi-permanent and often exhibit hardening, roughening or peeling within a few months of service. When a soft liner is absolutely indicated then silicone, as opposed to acrylic resin materials, are often preferred as they are not associated with leaching of plasticizers, which have the potential to cause unwanted biological effects. Soft liners provide a rougher surface finish than hard denture acrylic and nylon, which increases their potential to harbour denture plaque and micro-organisms. The use of silicone polishing points can obtain a highly polished acrylic surface for dentures which have been adjusted chairside, and routine removal of denture plaque and micro-organisms is most effectively achieved by mechanical cleaning with a brush or in a sonic cleaner using a cleaning paste or solution, respectively.