Australian Government: National Health and Medical Research Council. A Report of a NHMRC Working Party. 1999. http://www.nhmrc.gov.au
Lynch CD, Wilson NHF. Managing the phase-down of amalgam: part II. Implications for practicing arrangements and lessons from Norway. Br Dent J. 2013; 215:159-162
Opdam N, Bronkhorst E, Roeters J, Loomans B. A retrospective clinical study on the longevity of posterior composite and amalgam restorations. Dent Mater. 2007; 23:2-8
Burke F, Mackenzie L, Sands P. Dental materials – what goes where? Class I and Class II cavities. Dent Update. 2013; 40:260-274
Correa M, Peres M, Peres K, Horta B, Barros A, Demarco F. Amalgam or composite resin? Factors influencing the choice of restorative material. J Dent. 2012; 40:703-710
Raj V, Macedo G, Ritter A. Longevity of posterior composite restorations. J Esthet Rest Dent. 2007; 19:3-5
Opdam N, Bronkhorst E, Loomans B, Huysmans M. 12 Year survival of composite vs amalgam restorations. J Dent Res. 2010; 89:1063-1067
Mjör I, Moorhead J, Dahl J. Reasons for replacement of restorations in permanent teeth in general dental practice. Int Dent J. 2000; 50:361-366
Türkün LS, Aktener BO, Ateş M. Clinical evaluation of different posterior resin composite materials: a 7-year report. Quintessence Int. 2003; 34:418-426
Burgess JO, Walker R, Davidson JM. Posterior resin-based composites: review of the literature. Pediatr Dent. 2002; 24:465-479
Briso AL, Mestrener SR, Delicio G Clinical assessment of postoperative sensitivity in posterior composite restorations. Oper Dent. 2007; 32:(5)421-426
Mjör I. The reasons for replacement and the age of failed restorations in general dental practice. Acta Odontol Scand. 1997; 55:58-63
Kopperud S, Tveit A, Gaarden T, Sandvik L, Espelid I. Longevity of posterior dental restorations and reasons for failure. Eur J Oral Sci. 2012; 120:539-548
Versluis A, Tantbirjoin D, Douglas W. Do dental composites always shrink towards the light?. J Dent Res. 1998; 77:1435-1445
Millar B, Robinson P. Eight year results with direct ceramic restorations (Cerana). Br Dent J. 2006; 21:515-520
Kwon Y, Ferracane J, Lee IB. Effect of layering methods, composite type, and flowable liner on the polymerization shrinkage stress of light cured composites. Dent Mater. 2012; 28:(7)801-809 https://doi.org/10.1016/j.dental.2012.04.028
Rullmann I, Schattenberg A, Marx M, Willershausen B, Ernst CP. Photoelastic determination of polymerization shrinkage stress in low-shrinkage resin composites. Schweiz Monatsschr Zahnmed. 2012; 4:294-299
Burgess J, Cakir D. Comparative properties of low-shrinkage composite resins. Compend Contin Educ Dent. 2010; 2:10-15
Ilie N, Hickel R. Investigations on a methacrylate-based flowable composite based on the technology. Dent Mater. 2011; 4:348-355
Flury S, Hayoz S, Peutzfeldt A, Hüsler J, Lussi A. Depth of cure of resin composites: is the ISO 4049 method suitable for bulk fill materials?. Dent Mater. 2012; 28:521-528
Scientific Compendium SDR™. 2005; 10-13
Lassila LV1, Nagas E, Vallittu PK, Garoushi S. Translucency of flowable bulk-filling composites of various thicknesses. Chin J Dent Res. 2012; 15:31-35
Ivoclar Vivadent AG Research and Development. Tetric EvoCeram Bulk Fill Scientific Documentation 2013; 2.3. 11-15
Weinmann W, Thalacker C, Guggenberger R. Siloranes in dental composites. Dent Mater. 2005; 21:68-74
Van Dijken JWV, Pallesen U. SDR®, Xeno V+, Ceram∙X mono+ Clinical Study, Results at 12 months (Data available from Dentsply DeTrey). 2012;
Frankenberger R, Schulz M, Holl S, Seitner T, Matthias J, Roggendorf MJ.Marburg, Germany: Department of Operative Dentistry and Endodontics, Medical Center for Dentistry, University Medical Center Giessen and Marburg, Campus Marburg, Georg-Voigt-Str. 3, D-35039;
Baracco B, Perdigão J, Cabrera E, Ceballos L. Two-year clinical performance of a low-shrinkage composite in posterior restorations. Oper Dent. 2013; 38:591-600
Manhart J, Chen H, Hamm G, Hickel R. Buonocore Memorial Lecture. Review of the clinical survival of direct and indirect restorations in posterior teeth of the permanent dentition. Oper Dent. 2004; 29:(5)481-508
Thordrup M, Isidor F, Hörsted-Bindslev P. A one-year clinical study of indirect and direct composite and ceramic inlays. Scand J Dent Res. 1994; 102:(3)186-192
Van Dijken JMV, Hörstedt P. Marginal breakdown of 5-year-old direct composite inlays. J Dent. 1996; 24:(6)389-394
Shortall AC, Baylis RL, Baylis MA, Grundy JR. Marginal seal comparisons between resin-bonded Class II porcelain inlays, posterior composite restorations, and direct composite resin inlays. Int J Prosthod. 1989; 2:(3)217-223
Tooth-coloured, resin composite restorations are amongst the most frequently prescribed forms of dental restoration to manage defects in posterior teeth. The attainment of a desirable outcome when placing posterior resin composite restorations requires the clinician to have a good understanding of the benefits (as well as the limitations) posed by this material, together with a sound knowledge of placement technique. Numerous protocols and materials have evolved to assist the dental operator with this type of demanding posterior restoration. With the use of case examples, four techniques available are reported here.
CPD/Clinical Relevance: This article explores varying techniques for the restoration of Class II cavities using resin composite.
Article
The prescription of direct plastic restorative materials continues to be the primary choice for most dental practitioners for the management of carious lesions in the posterior dentition. This is largely on account of the conservation of the residual dental hard tissues, the relative economic benefits and the progressive development of direct restorative materials (especially of the adhesive variety).1
Very few would contest the notion of silver amalgam being a popular (and indeed successful) material in conservative dentistry, with a prescription record extending from the 1800s to the present time.2 In recent years however, particularly in light of the Minamata Treaty 20133 (which amongst several other objectives aims to phase down the use of dental amalgam), there has been an international paradigm shift concerning the placement of silver amalgam restorations, with countries such as Norway imposing a complete ban for the prescription of amalgam-based restorations since 2011, primarily on account of environmental concerns3 and a move towards less invasive protocols which begins to address the issues of restorative longevity versus tooth longevity over the lifetime of a patient.
In Australia, a Government report published by a working group for the NHMRC (National Health and Medical Research Council) in March 1999, described a reduction in the provision of dental amalgam restorations by private general dental practitioners from 57.9% in 1983–84 to 28.0% in 1997–98 (when considering the total number of dental restorations placed, inclusive of indirect restorations), thereby representing a reduction by almost 50%.4 The latter trend was suggested to be most likely to be accounted for by an implementation of a more minimally invasive philosophy by dental practitioners, largely rendered possible by advances taking place in the understanding of resin-adhesive dentistry, with a concomitant increase in the number of resin composite restorations doubling over the same time periods stated previously.
In the UK however, the move towards ‘amalgam free’ practice is taking place at a considerably slower pace. Whilst the teaching of posterior restorations has seen a change in the UK dental schools, dental students continue to gain slightly more experience with the placement of silver amalgam restorations and directly bonded resin composite restorations, respectively.5 Indeed, it is estimated that, in the UK, up to three-quarters of the restorations in posterior teeth are of the dental amalgam variety, with the annual expenditure on dental amalgam restorations being likely to exceed £300 million in the short term, with 12 million amalgam restorations being prescribed on the National Health Service in England and Wales by dental practitioners in the primary care sector.5
The popularity of dental amalgam may be accounted for by its beneficial mechanical properties, in particular its compressive strength, together with having a higher tolerance for technique sensitivity, such as moisture tolerance and placement technique, economic benefits, antibacterial activity and a proven record for success.6 However, poor tensile strength, poor aesthetic acceptance, lack of intrinsic adhesive potential and environmental concerns have prompted the search for alternative materials.7
Resin composite is one such material. Directly bonded posterior resin composite restorations have become increasingly popular since the early 1980s, particularly for the conservative and aesthetic management of small to medium sized cavities in posterior teeth.4 Bonded restorations may also provide a means of strengthening and conserving remaining tooth substrate in the long term.8
The durability or longevity of a dental material in the oral environment is often interpreted as a guide to relative success of its efficacy in the oral cavity.9 Cross-sectional retrospective studies (often undertaken in the primary care environment, with less well defined selection criteria and protocols, respectively), based on the survival of posterior amalgam restorations, have reported median survival times of between 6.6 and 14.0 years, versus 3.3 to 4.7 years for directly bonded posterior resin composite restorations.6 The principal causes attributed to the reasons for the higher failure rate of posterior resin composite restorations have been listed in Table 1.
Secondary caries
Bulk restorative fracture
Marginal degradation
Surfaces wear
In contrast, analogous longitudinal clinical studies, with restorations being placed by trained operators, applying consistent protocols and careful selection criteria, reveal comparable, if not slightly more favourable, survival rates for both materials.10
The differences in longevity results between the various forms of study may be accounted for by a number of factors. These include:
Operator skill: Opdam et al 2010,10 have reported comparable annual failure rates of amalgam (1.3%) and resin composite restorations (1.8%) amongst patients with a low predisposition towards dental caries at a 5-year follow-up. Interestingly, at 12 years the annual failure rate for resin composite was lower (1.7%) versus 2.4% for silver amalgam restorations. It was concluded that operator skill was a key determinant for success when placing resin composite restorations.
Materials and techniques used.
Cavity size and the criteria for placement.
Patient compliance with oral hygiene advice, the oral environment and its contribution to a patient's susceptibility to caries.10
Polymerization shrinkage is a key factor, accounting for the relative failure of direct posterior resin composite restorations. A majority of the currently available products contain the monomer bisphenol-A glycidyl methacrylate (bis-GMA). The latter is a ‘bulky’ monomer; hence upon polymerization the distance between the monomers decreases significantly, resulting in volumetric shrinkage. Reports from several studies have described volumetric polymerization shrinkage of resin composites to range from between 2 to 3%.13
Clinically, as the material is placed within bounded cavity walls, the process of shrinkage has the tendency to transfer stresses to the cavity walls, which may result in the shearing of the adhesive interface between the restorative material and tooth, or indeed the pulling of opposing walls towards each other. The latter could manifest clinically in the formation of a marginal ‘gap’, tooth structure deformation ‘cuspal contraction’/fracture, post-operative sensitivity (POS), recurrent caries, enamel cracks or marginal staining. As listed in Table 1, the latter are often the primary reasons for observing clinical failures with direct posterior resin composite restorations.
The risk of POS has been reported to be more likely to occur in association with larger, more complex restorations. However, for the majority of patients, POS disappears over a period of time from placement.14 A longevity study by Mjör 1997,15 where 537 posterior composite restorations were placed by general practitioners, reported a median survival time of 6 years. The primary cause of failure was described to be recurrent caries, accounting for 38% of all overall failures. Kopperud et al 201216 have reported a 2.5 times greater risk of failure of resin composite restorations for patients who present with higher caries predisposition. Polymerization shrinkage occurring at the gingival margin is a prime site for the stagnation and ingress of cariogenic bacteria.
A number of factors can influence the magnitude of contraction, some of these are under the control of the dental operator. Resin composites with a high modulus of elasticity are associated with greater stress transference to the tooth structure upon polymerization as the elastic modulus of a composite resin tends to increase with the relative filler content. On the other hand, more highly filled resins are likely to display lesser levels of polymerization shrinkage as a result of their lower relative resin content.
The technique of application is also important. The incremental insertion of resin composites reduces the bulk of material cured at any one point in time, thereby decreasing the effect of the setting reaction. Incremental application also reduces the so-called ‘C-factor’ (which is the ratio of the bonded area of the restoration to that of the unbonded area). A reduction in the C-factor is thought to relieve the stresses developed at the adhesive layer between the tooth and resin material.17
Other attempts to reduce the volume of shrinkage include the application of bases/liners with lower elastic moduli, such as glass ionomer cements (including those of the resin-modified variety), chemically cured resin composite formulations, the use of contemporary low shrinkage, bulk-fill materials and perhaps, less frequently today, the inclusion of beta-quartz inserts such as Cerana, Nordiska, Sweden.18 The prescription of indirect resin composite restorations will also largely negate the effect of polymerization shrinkage, as the bulk of this takes place extra-orally.
Clearly, operator knowledge and skill are paramount towards a successful outcome. The aim of this paper is to describe, on a case by case basis, the differing methods of resin composite application for the restoration of posterior cavities, some of the techniques for which may prove to be more workable for a given operator than another, together with an overview of the pros and cons of each technique described, supported where possible by evidence-based data. The techniques will also highlight advances which have taken place in resin technology and an increased understanding of the properties and behaviour of this material, such as the use of bulk-fill materials, ‘direct-indirect’ placement techniques and the use of indirect resin composite restorations, which may have the potential to improve the longer term outlook of these restorations, together with some of the commonly encountered pitfalls associated with the use of this material in this application. The cases described below were completed as part of the in course assessment requirements for the MSc in Aesthetic Dentistry, King's College London.
The direct placement of a posterior resin composite restoration
The direct placement of resin composite is perhaps the most commonly applied method for the prescription of the latter form of restorative material. It provides a means of delivering conservative, aesthetic, bonded restorations with the merits of lower relative cost (as no laboratory fees or additional materials for indirect restorations are required), offers a single visit procedure and the avoidance of a provisional restoration, which would present the added complication of microleakage.
However, placement protocols may be highly demanding of operator skill for the attainment of a superior aesthetic outcome and morphology (that is conducive towards optimal function), both in terms of occlusal anatomy and the attainment of patent, readily cleansable inter-proximal contact area(s), particularly for more complex cavity designs and functionally demanding cases. Adequate moisture control may also be problematic which, if sub-optimal, may culminate in premature failure of an adhesively retained restoration. Improper resin placement technique may also compound the well-documented concern of polymerization shrinkage, and the associated sequelae as discussed above.
Case 1: Directly bonded resin composite restoration
Case 1 (Figures 1, 2, 3) is an example of a 30-year-old male who presented as a new patient diagnosed with multiple carious lesions, including that affecting the upper left first molar. The patient was prescribed traditional direct conservative composite resin restorations for the management of the aforementioned carious lesions. When employing traditional direct composite resin as a posterior restorative, it is recommended that an incremental layering technique be adopted using increments no larger than 2 mm, with the aim of reducing polymerization shrinkage stress and allowing sufficient light penetration through the material itself.19 Various means of incremental application have been described in the literature, such as the oblique layering concept and the horizontal layering concept.
Figure 1. Case 1: Pre-operative.Figure 2. Case 1: Cavity preparation.Figure 3. Case 1: Completed restoration.
Following administration of local anaesthesia, occlusal stops were marked using articulating paper (GHM 12 Micron Foil Hanel, Coltene Whaledent Inc, Ohio, USA) and the quadrant isolated using a rubber dam (Roeko Non Latex FlexiDam, Coltene Whaledent Inc, Ohio, USA) and dental caries subsequently removed (Figure 2). The latter culminated in the minor involvement of the mesial marginal ridge and contact area of the first molar tooth, thus it was decided to restore this tooth via a tunnel preparation in order to preserve the well-developed marginal ridge. A cellulose acetate strip was applied and subsequently secured with a wooden wedge that was used to seal the breach during restoration.
Increments of a micro hybrid posterior composite, (Filtek P60, A3, 3M ESPE, Loughborough, UK) were readied and maintained in a light-proof container. The cavities were conditioned using a total etch technique (37% phosphoric acid) followed by a dentine bonding agent (Prime & Bond NT, Dentsply, USA) that was air dispersed for 5 seconds (so as to permit solvent evaporation) and cured for 10 seconds (Coltolux LED, Coltene Whaledent Inc, Ohio, USA).
The first increment was adapted to the floor of the cavity and cured for 40 seconds. Subsequent increments were layered on alternating cavity walls and cured for 40 seconds until the cavity reached occlusal level where smaller increments were then used to recreate the cuspal anatomy. Brown fissure tints (Color, Kerr CA, USA) were applied into the central fissures and lightly brushed and dispersed using a micro brush and cured for 20 seconds.
Following rubber dam removal, the restoration was marked in both static and dynamic occlusal positions using articulating paper. A green stone (Dura-Green, Shofu, Japan) in a friction grip was used to adjust the occlusion to conform to the pre-operative occlusal prescription. Marginal refinement and smoothing were achieved using a white stone (Dura-White, Shofu Japan) in a latch grip, followed by dry high lustre polishing, performed after a further 3 days, to permit dark polymerization using a diamond impregnated rotary brush (Astrobrush, Ivoclar Vivadent, Schaan, Liechtenstein). Restorations were post-cured for 40 seconds, following the application of glycerine, so as to permit polymerization of the surface layer, which may be affected by the concept of oxygen inhibition, whereby the presence of ambient oxygen will prohibit complete polymerization of the surface layer and the presence of a medium such as glycerine will serve to block the latter and thereby permit polymerization upon further light curing. Figure 3 provides a view of the definitive restoration.
Case 2: Use of bulk-fill materials
As an attempt to overcome the matter of polymerization shrinkage and the associated sequelae, bulk-fill resins were introduced to the market place. Such materials have shown the potential in vitro to demonstrate reduced polymerization shrinkage stress values,20,21,22 as well as increased depth of cure,23 when compared to their predecessors.
A bulk-fill resin, such as SDR, does not vary substantially from its counterparts in terms of general composition and filler load, but has its effect through a larger monomer with an embedded modulator that mediates polymerization, providing conformational flexibility during cross-link formation and less polymerization stress.24 Increasing the translucency of the material itself also allows for a greater light penetration and subsequent depth of cure.23,25 Alternative photo-initiator systems have also been utilized that initiate a more potent degree and depth of conversion due to an intensive absorption of light and high photo-reactivity.26 Siloranes represent another group of composite resin that have been shown to demonstrate consistently low polymerization shrinkage values below 1%, by adopting a unique ‘ring opening polymerization’ through the use of a new siloxane-oxirane based monomer.27
The use of such a resin is depicted by Case 2 (Figures 4–7) that demonstrates the replacement of a defective mesio-occlusal glass ionomer restoration on an upper left first permanent molar of a female patient in her mid 20s (Figure 4). In this case, the same protocol was followed for pre-operative assessment and bonding as would be for a traditionally layered composite restoration (Case 1). In this instance, the first increment of flowable bulk-fill material (SDR, Dentsply, USA) was placed at the floor of the cavity and proximal box in a layer of 2–3 mm and cured for 20 seconds (Figure 6). The occlusal surface and majority of the proximal surface were then restored using Tetric EvoCeram Bulk Fill IVA (Ivoclar Vivadent, Schaan Liechtenstein) (Figure 7) placed in two increments approximately 3 mm in thickness. Although the manufacturers of these two materials recommend a curing time of 20 seconds at a depth of 4 mm, slightly smaller increments were used in this instance and cured for 30 seconds, with a final cure of 20 seconds from each surface of the restoration. Such methods were adopted to help reduce polymerization shrinkage stress and prevent any uncured resin within the restoration.
Figure 4. Case 2: Pre-operative situation.Figure 5. Case 2: Restoration removal.Figure 6. Case 2: Sectional matrix band placement and SDR lining.Figure 7. Case 2: Completed restoration with Tetric Bulk Fill.
Early results (12–36 months) from the use of Silorane™, SDR™ and Kerr Sonic Fill™ in posterior cavities seem to demonstrate comparable survival rates to traditional composite resin, assuming strict bonding protocols are followed.28,29,30
Case 3: Indirect resin composite restoration
As discussed above, the direct placement of posterior resin composite restorations is highly demanding of operator skill. Furthermore, the attainment of patent inter-proximal contacts and bulk fracture and the consequences of polymerization shrinkage are commonly cited problems with this technique. The placement of resin composite restorations may also take more clinical time as opposed to an analogous silver amalgam restoration owing to the higher level of technique sensitivity. The latter may prove to be challenging for some patients.
The indirect fabrication of resin composite restorations offers the potential to overcome some of the problems described above, as restorations may be fabricated extra-orally without the challenges of the soft tissues, salivary contamination and patient co-operation. Contact area and occlusal anatomy and form, respectively, can be developed on die stones, with the use of an appropriate form of occlusal apparatus if deemed necessary. As polymerization shrinkage takes place extra-orally, the consequences are reduced (other than dimensional changes occurring at the level of the resin lute). Furthermore, there is the potential to extend the level of polymerization beyond light curing, which has been claimed to enhance the mechanical properties of the restoration, as well as offer a more favourable prognosis in situations where cavity margins rest within dentine. A review of direct and indirect restorations by Manhart et al31 has determined annual failure rates of indirect composite inlays to be 1.9% (1.7% and 1.4% for ceramic and gold indirect restorations, respectively). This review also showed that indirect restorations demonstrated significantly lower annual failure rates than direct restorations fabricated using earlier materials.
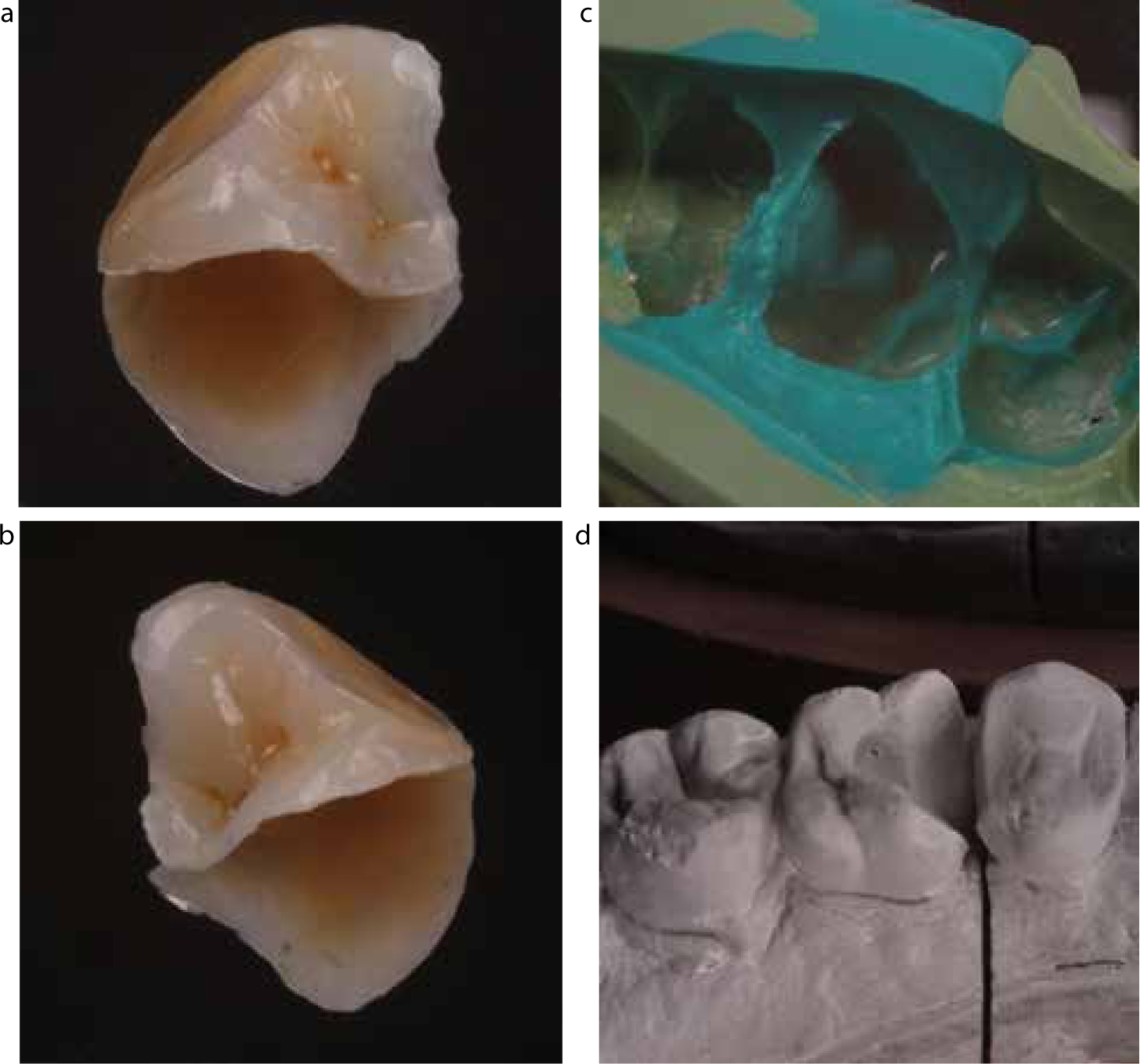
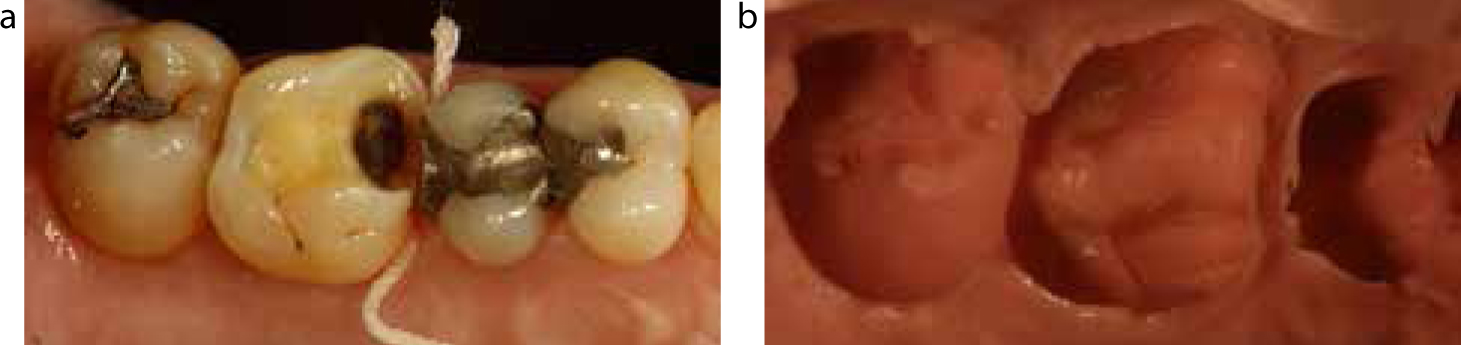
Figures 8–10 demonstrate an example of an indirect resin inlay restoration (Case 3), prescribed to replace a directly bonded resin restoration, presenting with an open contact and a marginal defect (Figure 8).
Figure 8.
(a, b) Case 3: Pre-operative situation.Figure 9.
(a–d) Case 3: To show isolation, bonding protocol and post-operative situation.Figure 10.
(a–d) Case 3: To show master impression, working die and completed lab fabricated composite inlay.
The treatment objectives were to reduce symptoms of food trapping and the potential for secondary caries by establishing a tight inter-proximal contact with a satisfactory peripheral marginal seal. An indirect laboratory made composite inlay (Gradia Indirect, GC Corporation, Tokyo, Japan) was prescribed as the prepared cavity extended beneath the gingival margin and past the embrasures, which would render sealing the floor of the cavity and simultaneously providing an optimal contact point unpredictable. Figure 9 demonstrates delivery of the final restoration that was bonded using a self-adhesive dual cure resin cement (RelyX Unicem, 3M ESPE, UK).
The indirect technique as shown by Case 3 does, however, require the blocking out of hard tissue undercuts. There is also a need to provide a provisional restoration, record impressions, additional visits and laboratory costs (Figure 10).
Case 4: Direct/Indirect technique
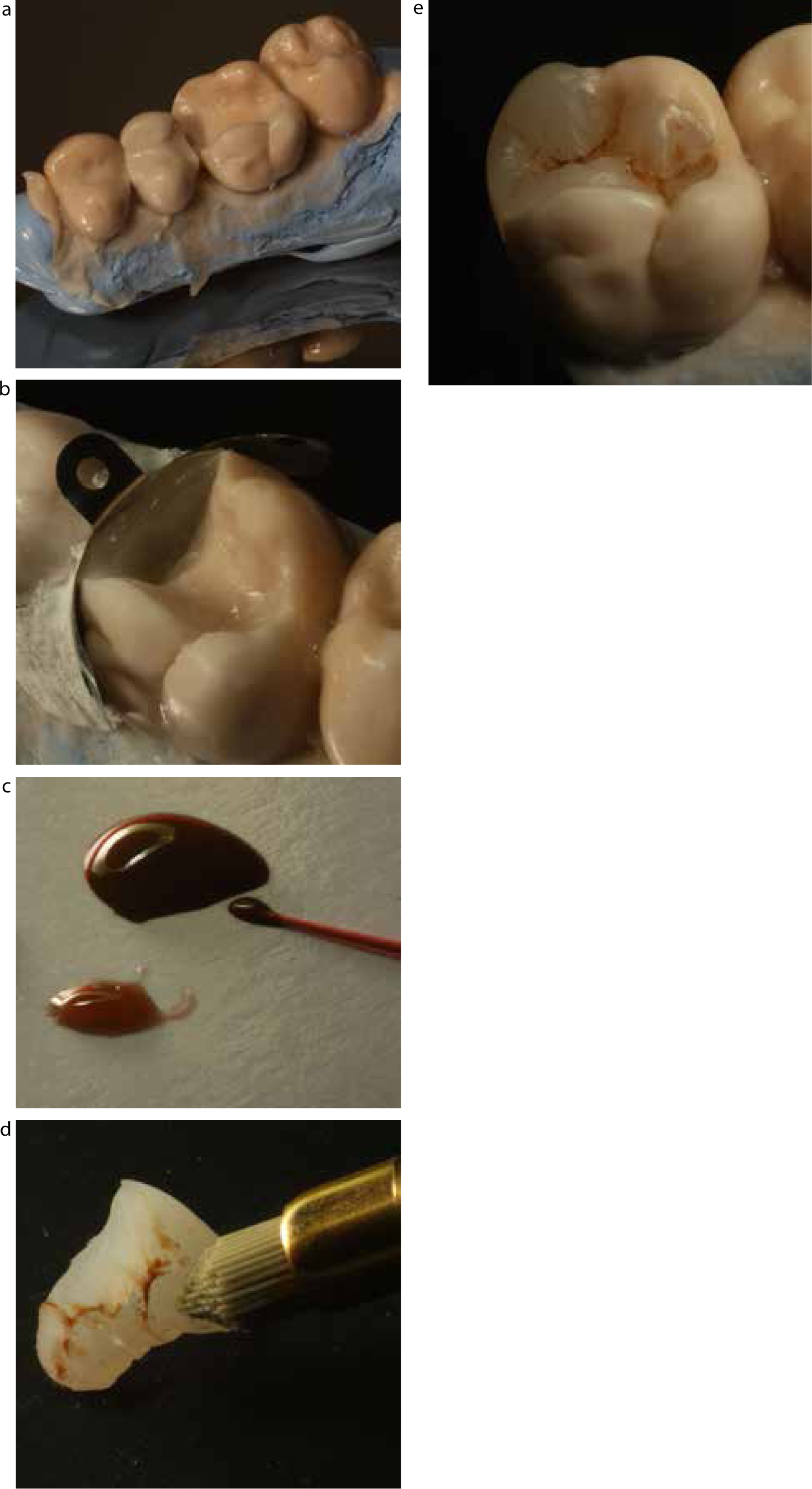
As a means of overcoming the need for some of the above aspects, there is the potential to fabricate the restoration using a direct-indirect approach. This is shown by Figures 11–13, which is an example of the application of a ‘Direct/Indirect technique’ using a silicone die fabricated chairside to provide a tooth-coloured restoration of a large cavity that has less potential for polymerization shrinkage stress compared to a directly placed composite restoration and can be completed in-office.
Figure 11.
(a, b) Case 4: Cavity preparation and sectional impression in alginate.Figure 12.
(a–e) Case 4: Chairside fabrication of semi-direct composite inlay on silicone working die.Figure 13.
(a–c) Case 4: Pre- and post-operative views and demonstration of occlusion.
Thordrup et al32 has reported an 80% survival rate for semi-direct inlays at 10 years that proved to be comparable to indirect composite, direct and indirect ceramic inlays. Van Dijken33 has also reported that the time and expense of Class II indirect composite restoration placement may not be justified as he reported comparable longevity at 11 years of semi-direct Class II composite inlays.
Preparation began with administration of local anaesthetic and removal of the previous restoration. Minor undercuts were eliminated and internal line angles softened. The inlay preparation was kept to the depth of the previous restoration and was smoothed with a white stone and a rubber polishing point. Non-impregnated retraction cord was used to open the mesial gingival margin of the preparation (Figure 11a) ready for an impression that was made using alginate in a sectional stock tray coated with adhesive (Figure 11b). If this technique were to be employed in a more complicated situation, for example an onlay, it would be sensible to record an opposing impression for accurate articulation. The use of PVS-based materials would also offer a higher level of accuracy as opposed to the use of alginate, which is less dimensionally stable.
The working die was fabricated using a silicone die material (Mach II, Parkell Inc, NY, USA). This was extruded into the impression to replicate the dental hard and soft tissues. A silicone bite registration paste (Blue Mousse, Parkell Inc, NY, USA) was then applied to a plastic base former and to the remaining part of the impression. The base former was then attached to the impression and allowed to set, following which it is simply removed from the impression to form an immediate working die (Figure 12a).
The die was partially sectioned to allow access to the mesial contact point of the preparation. A sectional matrix foil (Palodent, Dentsply, USA) was secured in place with a temporary filling material (Coltosol, Coltene Whaledent Inc, USA) in order to recreate the marginal ridge and interproximal contact point using a stock direct posterior composite resin material (Filtek P60, 3M ESPE, UK) (Figure 12b). The inlay was then built up in cuspal increments and brown tints applied to the central fissures (Color +, Kerr, CA, USA) (Figure 12c). Curing of each increment was carried out for 10 seconds followed by close curing of the restoration off the die for 1 minute over each surface (Coltolux LED, Coltene Whaledent Inc, USA). The die was then fully sectioned to refine the restoration fit margins using a fine abrasive disc (Soflex, 3M ESPE, UK). Final polishing was carried out with a diamond impregnated rotary brush (Astrobrush, Ivoclar Vivadent, Lichtenstein) (Figure 12d, e).
The patient returned on the same day for delivery of the restoration (Figure 13a). A bonding and finishing protocol identical to that of a lab fabricated direct inlay (Case 3) was followed. Occlusal adjustments were made intra-orally as would be similar to a direct restoration (Case 1) (Figure 13b). The final restoration (Figure 13c) was accepted well and a tight interproximal contact was confirmed with floss. Current clinical data for such a technique has shown 84% of semi direct composite inlays having gap free margins at 5 years, demonstrating good marginal integrity.34 This technique may help reduce cervical marginal leakage compared to a direct technique that can make it suitable for high caries risk patients where the cervical margin of the cavity is located within dentine.34
Conclusion
In summary, resin composite may offer the clinician a viable alternative to silver amalgam for the restoration of posterior defects. It is imperative for the operator to understand the benefits offered by the use of this material. Having a sound knowledge of differing placement techniques may assist the clinician with more challenging clinical scenarios. Table 2 provides a summary of the various techniques that may be used when prescribing tooth-coloured resin composite restorations.
Technique
Advantages
Disadvantages
Direct placement
No laboratory fee
Completed in a single visit
No provisional restoration required
Highly conservative
Materials and equipment readily available in a standard dental office set-up
Vast variety of shades and translucencies
Creation of a tight and well contoured interproximal contact can be difficult
Careful bonding and layering protocols are technique sensitive and time consuming
Isolation and moisture control must be maintained throughout whole procedure
Greater polymerization shrinkage stress
Highly aesthetic outcomes require a skilled operator
Direct placement with bulk-fill resins
No laboratory fee
Completed in a single visit
No provisional restoration required
Highly conservative
More time efficient to place
Lower polymerization shrinkage stress
Greater depth of cure
Restricted variety of shades and translucencies
Creation of a tight and well contoured interproximal contact can be difficult
Requires careful bonding protocols
Isolation and moisture control must be maintained throughout whole procedure
May be more expensive than traditional composite and not part of core stock lists
Highly aesthetic outcomes require a skilled operator
Indirect placement
Potential to enhance mechanical properties through extensive 3-dimensional light curing and heat treatment
A pre-cured restoration eliminates problems associated with polymerization shrinkage stress
More precise control of anatomy and occlusion
Isolation only required for final bonding of inlay
Precise marginal fit and adaption
Aesthetics controlled by skilled technician
More predictable marginal stability in dentine
Laboratory fees incurred
Requires two clinical visits
Impressions required
Requires a provisional restoration
Requires removal of undercuts
Semi-direct placement
No laboratory fee
Can be completed on same day
No provisional restoration required
Allows extensive 3-dimensional light curing
A pre-cured restoration eliminates problems associated with polymerization shrinkage stress
Isolation only required for final bonding of inlay
Works with any dental composite system
Additional time must be allocated for inlay fabrication and fitting
Impressions required
Requires removal of undercuts
Requires additional materials and equipment (die material, base former)
Highly aesthetic outcomes require a skilled operator