Burke FJT. Amalgam to tooth-coloured materials – implications for clinical practice and dental education: governmental restrictions and amalgam-usage survey results. J Dent. 2004; 32:343-350 https://doi.org/10.1016/j.jdent.2004.02.003
Green DJ, Banerjee A. Contemporary adhesive bonding: bridging the gap between research and clinical practice. Dent Update. 2011; 38:439-450 https://doi.org/10.12968/denu.2011.38.7.439
Green D, Mackenzie L, Banerjee A. Minimally invasive long-term management of direct restorations: the ‘5 Rs’. Dent Update. 2015; 42:413-426 https://doi.org/10.12968/denu.2015.42.5.413
Burke FJT, McCaughey AD. The four generations of dentin bonding. Am J Dent. 1995; 8:88-92
Buonocore MG. A simple method of increasing the adhesion of acrylic filling materials to enamel surfaces. J Dent Res. 1955; 34:849-853 https://doi.org/10.1177/00220345550340060801
Burke FJT. Attitudes to posterior composite filling materials: a survey of 80 patients. Dent Update. 1989; 16:114-120
Helvey GA. Adhesive dentistry: the development of immediate dentin sealing/selective etching bonding technique. Compend Contin Educ Dent. 2011; 32:22-35
Peumans M, De Munck J, Van Landuyt KL A 13-year clinical evaluation of two three-step etch-and-rinse adhesives in non-carious class-V lesions. Clin Oral Investig. 2012; 16:129-1
De Munck J, Van Landuyt K, Peumans M A critical review of the durability of adhesion to tooth tissue: methods and results. J Dent Res. 2005; 84:118-32 https://doi.org/10.1177/154405910508400204
Nakabayashi N, Kojima K, Masuhara E. The promotion of adhesion by the infiltration of monomers into tooth substrates. J Biomed Mater Res. 1982; 16:265-273 https://doi.org/10.1002/jbm.820160307
Burke FJT, Liebler M, Eliades G, Randall RC. Ease of use vs clinical effectivenss of restorative materials. Quintessence Int. 2010; 32:239-242
Peumans M, Munck J, Van Landuyt K Three-year clinical effectiveness of a two-step self-etch adhesive in cervical lesions. Eur J Oral Sci. 2005; 113:512-518 https://doi.org/10.1111/j.1600-0722.2005.00256.x
Peumans M, De Munck J, Van Landuyt K, Van Meerbeek B. Thirteen-year randomized controlled clinical trial of a two-step self-etch adhesive in non-carious cervical lesions. Dent Mater. 2015; 31:308-314 https://doi.org/10.1016/j.dental.2015.01.005
Burke FJT, Crisp RJ, Cowan AJ A randomised controlled trial of a universal bonding agent at three years: self etch vs total etch. Eur J Prosthodont Restor Dent. 2017; 25:220-227 https://doi.org/10.1922/EJPRD_01692Burke08
de Paris Matos T, Perdigão J, de Paula E Five-year clinical evaluation of a universal adhesive: a randomized double-blind trial. Dent Mater. 2020; 36:1474-1485 https://doi.org/10.1016/j.dental.2020.08.007
Nagarkar S, Theis-Mahon N, Perdigão J. Universal dental adhesives: current status, laboratory testing, and clinical performance. J Biomed Mater Res B Appl Biomater. 2019; 107:2121-2131 https://doi.org/10.1002/jbm.b.34305
Perdigão J, Araujo E, Ramos RQ Adhesive dentistry: current concepts and clinical considerations. J Esthet Restor Dent. 2021; 33:51-68 https://doi.org/10.1111/jerd.12692
Van Meerbeek B, Yoshihara K, Van Landuyt K From Buonocore's pioneering acid-etch technique to self-adhering restoratives. A status perspective of rapidly advancing dental adhesive technology. J Adhes Dent. 2020; 22:7-34 https://doi.org/10.3290/j.jad.a43994
Yoshihara K, Yoshida Y, Nagaoka N Adhesive interfacial interaction affected by different carbon-chain monomers. Dent Mater. 2013; 29:888-897 https://doi.org/10.1016/j.dental.2013.05.006
Feitosa VP, Sauro S, Ogliari FA Impact of hydrophilicity and length of spacer chains on the bonding of functional monomers. Dent Mater. 2014; 30:e317-323 https://doi.org/10.1016/j.dental.2014.06.006
Miyazaki M, Tsubota K, Takamizawa T Factors affecting the in vitro performance of dentin-bonding systems. Jpn Dent Sci Rev. 2012; 48:53-60
Loguercio AD, Muñoz MA, Luque-Martinez I Does active application of universal adhesives to enamel in self-etch mode improve their performance?. J Dent. 2015; 43:1060-1070 https://doi.org/10.1016/j.jdent.2015.04.005
Rosa WL, Piva E, Silva AF. Bond strength of universal adhesives: a systematic review and meta-analysis. J Dent. 2015; 43:765-776 https://doi.org/10.1016/j.jdent.2015.04.003
Muñoz MA, Luque-Martinez I, Malaquias P In vitro longevity of bonding properties of universal adhesives to dentin. Oper Dent. 2015; 40:282-292 https://doi.org/10.2341/14-055-L
Cardenas AM, Siqueira F, Rocha J Influence of conditioning time of universal adhesives on adhesive properties and enamel-etching pattern. Oper Dent. 2016; 41:481-490 https://doi.org/10.2341/15-213-L
Takamizawa T, Barkmeier WW, Tsujimoto A Influence of different etching modes on bond strength and fatigue strength to dentin using universal adhesive systems. Dent Mater. 2016; 32:e9-21 https://doi.org/10.1016/j.dental.2015.11.005
Thanaratikul B, Santiwong B, Harnirattisai C. Self-etch or etch-and-rinse mode did not affect the microshear bond strength of a universal adhesive to primary dentin. Dent Mater J. 2016; 35:174-179 https://doi.org/10.4012/dmj.2015-109
Saikaew P, Chowdhury AF, Fukuyama M The effect of dentine surface preparation and reduced application time of adhesive on bonding strength. J Dent. 2016; 47:63-70 https://doi.org/10.1016/j.jdent.2016.02.001
Cuevas-Suárez CE, da Rosa WLO, Lund RG Bonding performance of universal adhesives: an updated systematic review and meta-analysis. J Adhes Dent. 2019; 21:7-26 https://doi.org/10.3290/j.jad.a41975
Perdigão J, Lambrechts P, Van Meerbeek B The interaction of adhesive systems with human dentin. Am J Dent. 1996; 9:167-173
Lago MCA, Mendes CL, Annibal H Evaluation of bond strength to dentin of universal adhesive systems. Dent Mater. 2019; 35:(S1)
Bayne SC. Correlation of clinical performance with ‘in vitro tests’ of restorative dental materials that use polymer-based matrices. Dent Mater. 2012; 28:52-71 https://doi.org/10.1016/j.dental.2011.08.594
Loguercio AD, de Paula EA, Hass V A new universal simplified adhesive: 36-Month randomized double-blind clinical trial. J Dent. 2015; 43:1083-1092 https://doi.org/10.1016/j.jdent.2015.07.005
Perdigão J, Kose C, Mena-Serrano AP A new universal simplified adhesive: 18-month clinical evaluation. Oper Dent. 2014; 39:113-127 https://doi.org/10.2341/13-045-C
Lawson NC, Robles A, Fu CC Two-year clinical trial of a universal adhesive in total-etch and self-etch mode in non-carious cervical lesions. J Dent. 2015; 43:1229-1234 https://doi.org/10.1016/j.jdent.2015.07.009
Ruschel VC, Stolf SC, Shibata S Three-year clinical evaluation of universal adhesives in non-carious cervical lesions. Am J Dent. 2019; 32:223-228
Atalay C, Ozgunaltay G, Yazici AR. Thirty-six-month clinical evaluation of different adhesive strategies of a universal adhesive. Clin Oral Investig. 2020; 24:1569-1578 https://doi.org/10.1007/s00784-019-03052-2
Zanatta RF, Silva TM, Esper M Bonding performance of simplified adhesive systems in noncarious cervical lesions at 2-year follow-up: a double-blind randomized clinical trial. Oper Dent. 2019; 44:476-487 https://doi.org/10.2341/18-049-C
Oz FD, Ergin E, Canatan S. Twenty-four-month clinical performance of different universal adhesives in etch-and-rinse, selective etching and self-etch application modes in NCCL – a randomized controlled clinical trial. J Appl Oral Sci. 2019; 27 https://doi.org/10.1590/1678-7757-2018-0358
Perdigão J, Ceballos L, Giráldez I Effect of a hydrophobic bonding resin on the 36-month performance of a universal adhesive – a randomized clinical trial. Clin Oral Investig. 2020; 24:765-776 https://doi.org/10.1007/s00784-019-02940-x
van Dijken JW, Pallesen U. Three-year randomized clinical study of a one-step universal adhesive and a two-step self-etch adhesive in class ii composite restorations. J Adhes Dent. 2017; 19:287-294 https://doi.org/10.3290/j.jad.a38867
Szesz A, Parreiras S, Reis A, Loguercio A. Selective enamel etching in cervical lesions for self-etch adhesives: A systematic review and meta-analysis. J Dent. 2016; 53:1-11 https://doi.org/10.1016/j.jdent.2016.05.009
Burke FJT, Crisp RJ. A practice-based assessment of the handling properties of 3M ESPE Scotchbond universal adhesive. The Dentist. 2014; 50-54
Burke FJT, Crisp RJ. Handling evaluation of GC G-Premio Bond. The Dentist. 2021; 54-57
Burke FJT, Crisp RJ, Sands P. A ‘handling’ evaluation of the Dentsply Sirona Class II solutions system by the PREP Panel. Dent Update. 2018; 45:1032-1040
Burke FJT, Crisp RJ. Clinical evaluation of SDI Zipbond by the PREP Panel. The Dentist. 2020; 52-55
Demarco FF, Corrêa MB, Cenci MS Longevity of posterior composite restorations: not only a matter of materials. Dent Mater. 2012; 28:87-101 https://doi.org/10.1016/j.dental.2011.09.003
Brunton PA, Burke FJT, Sharif MO Contemporary dental practice in the UK: demographic details and practising arrangements in 2008. Br Dent J. 2012; 212:11-15 https://doi.org/10.1038/sj.bdj.2011.1098
Nagaoka N, Yoshihara K, Feitosa VP Chemical interaction mechanism of 10-MDP with zirconia. Sci Rep. 2017; 7 https://doi.org/10.1038/srep45563
Passia N, Mitsias M, Lehmann F, Kern M. Bond strength of a new generation of universal bonding systems to zirconia ceramic. J Mech Behav Biomed Mater. 2016; 62:268-274 https://doi.org/10.1016/j.jmbbm.2016.04.045
Göstemeyer G, Schwendicke F. Inhibition of hybrid layer degradation by cavity pretreatment: meta- and trial sequential analysis. J Dent. 2016; 49:14-21 https://doi.org/10.1016/j.jdent.2016.04.007
The ability to successfully bond restorations to dentine is central to minimally invasive restorative dentistry. While dentine bonding agents have gone through a variety of ‘generations’, it is the purpose of this article to describe the latest clinical and laboratory research on universal adhesives. Results from the latest laboratory and clinical research indicates that universal adhesives are a step forward in the quest for the ultimate bond to tooth substance and ease of use of the adhesive. The wide variety of studies that indicates the effectiveness of universal adhesives are discussed, along with research that indicates that selective enamel etching is a beneficial procedure when using these materials.
CPD/Clinical Relevance: Universal adhesives appear to hold promise in the quest for a reliable bond to dentine.
Article
Dentine bonding agents play a central role in the sealing and retention (where necessary) of resin composite restorations, which are increasingly placed by dentists worldwide.1 Bonding to dentine is also central to the practice of minimally invasive dentistry, given that restorations, which may be bonded to tooth substance, do not require the macro-mechanical retentive features such as locks and keys that are a feature of (non-adhesive) dental amalgam or gold cavity preparations.2
A dentine adhesive should perform the following functions:3
Provide an immediate, strong and definitive bond to dentine;
Seal the cavity and minimize leakage;
Resist microbial or enzymatic degradation;
Provide adhesion per se of the restoration in cases where this is necessary;
Prevent post-operative sensitivity;
Reduce the risk of recurrent caries;
Prevent marginal staining;
Be easy to use.
It is the intention of this article to trace the history of dentine adhesives since that is relevant to the performance of the latest group of adhesives, the universal adhesives (UAs), and thereby to update readers on the progress of UAs since a previous Dental Update paper in 2017,4 and to compliment other Dental Update publications on the subject, which readers may wish to read as background, such as those by Green and Banerjee,2 and, Green et al.5
A brief history of bonding to dentine
In the past, dentine bonding agents were classified into generations.6 However, this means of identifying different groups of bonding agents generally fell into disarray because of confusion regarding which ‘generation’ each type of bonding agent fitted into. Until recently, the classification has therefore been to simply subdivide resin-based dentine bonding agents into etch and rinse materials (also known as total etch materials) and self-etch materials, with some workers classifying these according to the number of steps involved in their placement (one or two), or by their pH.3,7
The year 1955 heralded what we now realize to be a game-changing breakthrough in restorative dentistry, namely the genesis of adhesive (and, therefore, more minimally invasive) dentistry by enabling clinicians to bond to enamel, when this was first described by Buonocore.8 This also has facilitated the development of resin composite materials, with these materials becoming increasingly used worldwide,1 principally because of patient concerns regarding mercury in dental amalgam, the Minamata Agreement of 2013 that recommended reduction in the use of dental amalgam, and increasing patient requests to receive tooth-coloured restorations in their posterior teeth.9
Unlike enamel, dentine is a vital substrate with circa 20% organic material and 10% water by weight. These factors make bonding to dentine more challenging than to enamel. Also involved in this challenge is the smear layer on the dentine surface, this having been defined as a ‘layer which appears on the surface of teeth that have undergone dental instrumentation procedures, such as cutting with a dental bur: it cannot be rinsed away, but it can be dissolved by dilute organic acids, such as phosphoric acid’.10 This crystalline, uniform layer comprises debris consisting of hydroxyapatite particles, altered collagen and bacteria. Early resin-based dentine bonding agents were little more than wetting agents that penetrated the smear layer. When it was realized that the smear layer was not well adherent to the underlying dentine, it became obvious that it was necessary to treat it in some way. Until recently, therefore, there were two distinct types of resin-based dentine adhesive.
Etch and rinse (or total etch) materials
The etch and rinse (or total etch) materials are for which the smear layer was dissolved by the application of 30–35% phosphoric acid, followed by washing, drying and the application of a primer and the bonding agent. These materials, with a four-stage clinical application protocol, could be considered technique sensitive because of the risk of a failure if any stage was not carried out optimally.3 However, some materials of this type, such as Optibond FL (Kerr, Orange, CA, USA) remain in use, given that they are considered by some clinicians to be the gold standard to which other bonding agents must be compared.11 This material has been shown to provide excellent retention at 13 years in non-carious cervical lesions (NCCL).12 It may also be relevant to note that, according to two reviews, Optibond FL and Clearfil SE (Kuraray, Tokyo, Japan) have been considered to be the gold standard of etch and rinse and self-etch adhesives, respectively.13,14
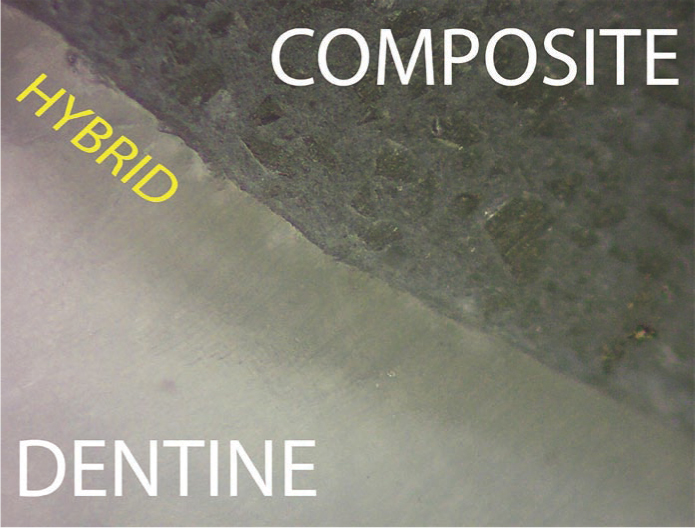
What happens to the smear layer with etch and rinse adhesives? The smear layer is dissolved and then washed away, with the acid also dissolving the most superficial 1–5 microns of dentine, removing hydroxyapatite, leaving only collagen fibres. When the resin bonding agent is applied to the decalcified dentine surface, a layer is formed on the decalcified dentine surface, with the resin polymerizing around the collagen fibres: this was termed the hybrid layer by Nakabayashi (Figure 1).15
Figure 1. The hybrid layer.
Self-etch adhesives
Because of the clinical technique sensitivity associated with etch and rinse materials, and the belief by manufacturers that clinicians seek materials that are easy and fast to use, the group of bonding agents known as self-etch adhesives were presented to clinicians in the early 1990s. (In this regard, it has been considered that a material that is easy to use will produce optimal results.16) In these self-etch bonding systems, the bonding resin is combined with an acid (generally phosphoric acid) in order to reduce the pH to a level that is said to be sufficiently low to carry out the etching step at the same time as producing bonding. These materials were, therefore, significantly simpler to use than the etch and rinse materials and could be presented in only one bottle, thereby facilitating their use. The so-called self-etch adhesives may be considered to have advantages when compared to etch and rinse types, for example:3
No post-conditioning rinsing, hence less operator sensitivity;
Less sensitive to the degree of wetness/dryness of the dentine surface;
Single unit dose packaging possible, hence reduced risk of cross infection, and simple to use;
Simultaneous demineralization and resin-infiltration meant that it was not possible to over-etch the dentine, leading to reduced levels of post-operative sensitivity.
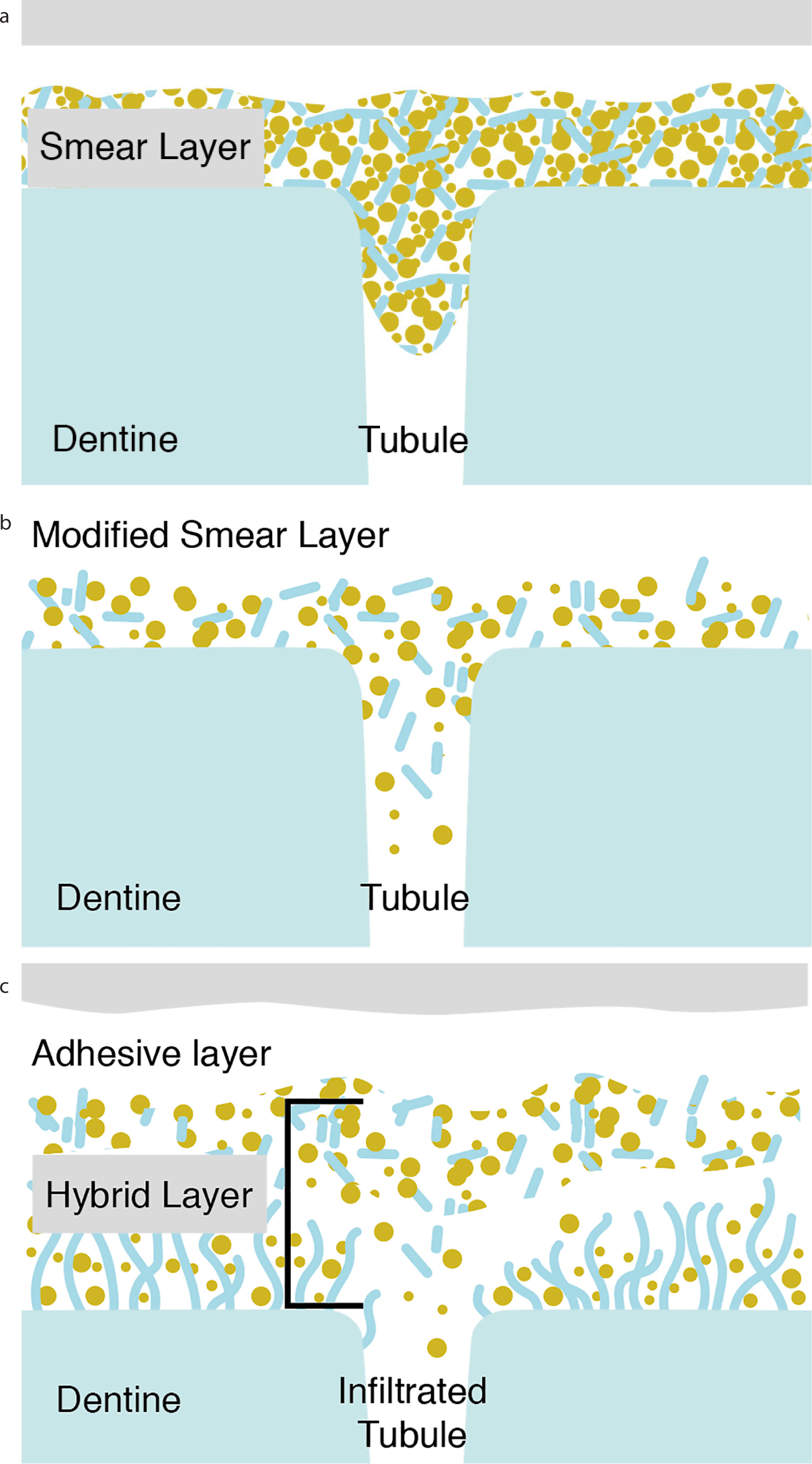
What happens to the smear layer with self-etch adhesives? The acidic resin does not remove the smear layer: the slightly decalcified surface leads to the formation of a hybrid layer, with the smear layer becoming incorporated into the hybrid layer (Figure 2).
Figure 2.
(a) Dentine prior to application of adhesive. The smear layer is on the dentine surface. (b) Application of the self-etch adhesive modifies the smear layer. (c) When the adhesive is polymerized, a hybrid layer is formed, with the smear layer particles within it.
Among the disadvantages of self-etch adhesives listed in 2004 was: ‘adhesion to enamel requires further long-term evaluation in some systems’.3 Hence, the development of the concept of selective enamel etching.
The advent of selective enamel etching
While laboratory testing allows variables to be investigated, it may be considered that the ultimate test of adhesives is their clinical performance in a non-retentive class V cavity. Results of a 5-year landmark study from Peumans and colleagues17 involving the clinical use of the (so-called) self-etch adhesive, Clearfil SE (Kuraray), in 100 non-retentive class V cavities, restored with resin composite, has indicated that, when the enamel margins were ‘selectively etched’ with phosphoric acid, the enamel cavity margins had advantages in terms of integrity and lack of staining. Accordingly, the concept of selective enamel etching was born.17 When these workers extended their study to 13 years,18 the results, with a 62% recall rate and 96% retention rate, continued to indicate fewer small marginal defects on enamel in the selective enamel etch group (16% cf 4% in the self/non-etch group). The authors commented that ‘the limited micromechanical retention of the enamel surface conditioned by the self-etching primer (pH = 2) and the stable chemical bond between 10-methacryloyloxydecyl dihydrogen phosphate (10-MDP) and hydroxyapatite (HA), seems to be strong and durable enough to have a clinically acceptable enamel bond in 95% of restorations after 13 years of clinical functioning. The authors added that ‘the only remarkable (not significant) difference in the present clinical trial was that small marginal defects and/or superficial discoloration at the enamel side were observed more frequently in the solely self-etch group. This difference between both groups, also noticed at previous recalls, has remained quite stable during the last 5 years’. In this regard, the so-called self-etch adhesives were introduced because of dentists' requests for ease of use and speed, with this not involving the use of phosphoric acid. However, with the benefit of hindsight, it could be considered that clinicians were naïve to expect materials with a pH of circa 2.5 to provide similar marginal integrity or low incidence/absence of marginal discolouration on enamel margins as could be obtained when these were etched using phosphoric acid (pH circa 0.5), remembering that pH operates on a logarithmic scale.
Universal adhesives
It should be added that the two groups of bonding agents discussed above were type specific, in other words, for the etch and rinse materials to be clinically effective, the dentine surface must be etched, while for the self-etch materials, the dentine surface must not be etched, but merely be physically clean. In this regard, the present authors suggest cleaning with pumice and water. A new group of adhesives, the universal adhesives (UAs), has therefore been introduced to overcome the type specificity associated with previous adhesives in regard to mode of etching.
Is capable of being used in whichever etching mode that the operator considers appropriate (total etch, self-etch or selective enamel etch): the authors of this paper consider that selective enamel etching is appropriate, as will be demonstrated when the results of recent research are discussed later;
May be used for direct and indirect dentistry, the latter generally in conjunction with a resin-based luting system from the same manufacturer as the bonding agent, with the luting system incorporating a material-specific initiator. However, at the time of writing, this only applies to the materials from two manufacturers, 3M and GC.
In addition:
According to Matos and co-workers,20 the term ‘universal’ is appropriate due to the addition of the resinous monomer 10-MDP to provide chemical bonding to hard tissue and metals;
According to Nagarkar and colleagues,21 there is no official definition for what qualifies as a UA, the literature describes it as a single-bottle, no-mix adhesive system that performs equally well with any adhesion strategy and bonds adequately to tooth structure, as well as to different direct and indirect restorative materials;
According to Perdigão et al,22 UAs were recommended for a number of clinical applications, including direct and indirect restorations, core build-ups, zirconia primers and dentine densensitizing.
So, while the etch and rinse and self-etch bonding agents were type specific, the UAs are indeed universal, insofar that they can be used in whichever etching mode a clinician feels is appropriate and for other clinical applications. Factors involved in the decision process regarding etch mode may include:
Not wishing to etch dentine for fear of producing post-op sensitivity (particularly in posterior teeth) while etching enamel margins to optimize the marginal characteristics (ie no long-term defects or staining) of the restoration (ie using selective enamel etching);
Using self-etch mode in a patient lacking co-operation, or for speed of use;
Using etch and rinse mode because of a belief that this is superior.
The rise and rise of 10-MDP
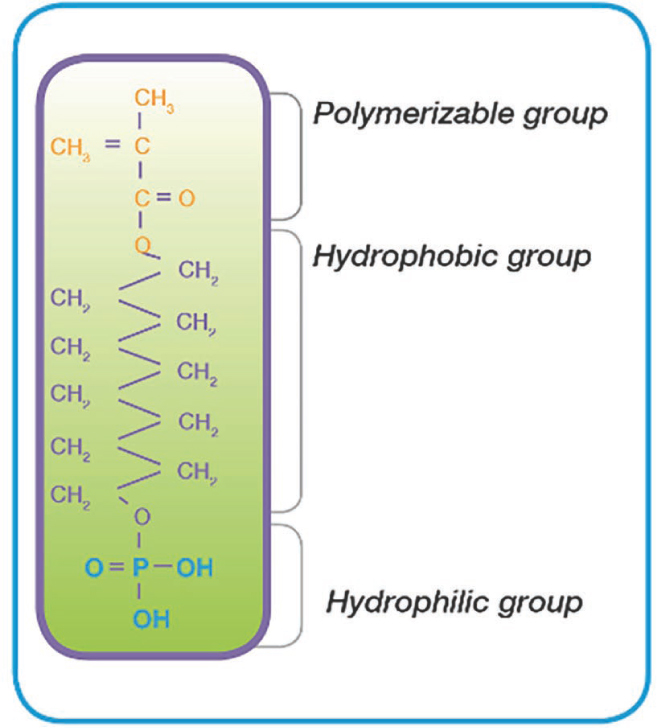
Another difference between UAs and self-etch adhesives are the functional phosphate and/or carboxylate monomers incorporated into their constituents that facilitate chemical bonding to the calcium in HA. A factor that the majority of this new group of bonding agents has in common is the resin 10-MDP,23 with this monomer first appearing in the adhesive, Clearfil New Bond (Kuraray), in the early 1980s (Figure 3). Van Meerbeck and colleagues24 have considered that 10-MDP is one of the most effective monomers to strongly ionically bond to HA, forming stable 10-MDP-Ca salts, with these authors adding that this chemically stable bond has been shown to contribute to bond durability. This has been demonstrated clinically in the 13-year study by Peumans et al18 when using Clearfil SE Bond (Kuraray), which includes 10-MDP, as adhesive for restoration of class V resin composite restorations, with very positive results,18 this having been attributed by the authors to the presence of 10-MDP in the formulation, given that the restorations without selective enamel etching were still retained despite marginal discrepancies.
Figure 3. Chemical formula of 10-MDP.
It has been considered by Perdigão25 that, without calcium, it is unclear how 10-MDP adhesives are able to bond ionically to etched dentine. They therefore stated that 10-MDP-containing adhesives may need to be applied only on unetched dentine, additionally using a selective enamel-etching technique.
The length of the long hydrophobic 10-carbon chain has also been reported to contribute to its bonding ability.26 However, in this regard, longer chains in monomers such as 10-MDP are more hydrophobic, which could enhance the chemical interaction with calcium and reduce their degradation.27
In summary, therefore, it may be considered that the incorporation of 10-MDP into an adhesive's formulation provides a ‘belt and braces’ approach, this uniquely providing an ionic bond to calcium, ie to HA in dentine, via the hydrophilic group incorporated in the molecule, along with a micromechanical bond via the hybrid layer. However, although Van Meerbeck and colleagues,24 in their comprehensive review of dental adhesives, termed 10-MDP as ‘today's most effective functional monomer’, they stated that it was not the perfect functional monomer because it was sensitive to hydrolytic degradation at the two ester groups linking both functional groups to the central spacer group. The 10-MDP patent expired in 2003, with the result that manufacturers other than the patent holders, Kuraray, were able to start adding this phosphate monomer to their new adhesives.
The components of some universal bonding agents are presented in Table 1.21,22 From this, it is apparent that all UAs contain 10-MDP and some have an added resin to facilitate bonding, such as G Premio Bond with 4-META (developed by Nakaybashi), Optibond Universal (GPDM, Kerr) Prime&Bond Active (PENTA, Dentsply Sirona, Weybridge, UK) and others have a polyalkenoate derivative such as PAC (Scotchbond Universal and Scotchbond Universal Plus, both 3M, MN, USA), and MCAP (Adhese Universal, Ivoclar-Vivadent, Schaan, Liechtenstein).
Universal adhesive
Manufacturer
Classification by pH
Functional monomer(s)
All-Bond Universal (ABU)
BISCO
Ultra-mild 3.2
10-MDP
AdheSE Universal
Ivoclar Vivadent
Ultra-mild 2.5–3.0
10-MDP, MCAP
Optibond Universal
Kerr
Ultra-mild 2.5–3.0
GPDM, 10-MDP
One Coat 7 Universal
Coltene
Ultra-mild 2.8
10-MDP, methacrylated polyacid
Scotchbond Universal
3M
Ultra-mild 2.7
10-MDP, PAC
Scotchbond Universal Plus
3M
Ultra-mild 2.7
10-MDP, PAC
Prime&Bond Elect
Dentsply Sirona
Ultra-mild 2.5
10-MDP, PENTA
Clearfil Universal Bond
Kuraray Dental
Mild 2.3
10-MDP
Futurabond U
VOCO
Mild 2.3
10-MDP
iBOND Universal
Kulzer
Intermediate strong 1.6–1.8
10-MDP, 4-META
G-Premio Bond
GC
Intermediate strong 1.5
10-MDP, 4-META, MDTP
So, just how good are universal adhesives?
As with any recently introduced material, there is a relative paucity of evidence relating to these new materials, although this is building. The most researched UA is Scotchbond Universal Adhesive (SBU, 3M), given that this was the first of this group of materials to be released commercially, but other UAs have recently been examined.
UAs may be classified, similarly to self-etch adhesives, according to their pH, according to the classification by Miyazaki et al28 and van Meerbeck and colleagues24 in which the material was classified as shown in Table 2.
Classification
pH
Strong
<1
Intermediately strong
1–2
Mild
≈2
Ultra-mild
≥2.5
Laboratory studies
A number of laboratory studies were presented previously,4 namely those by Loguerico and co-workers,29 da Rosa and co-workers,30 Munoz and co-workers,31 Chen and co-workers32 and others,33,34,35,36 with generally positive results concerning the in vitro performance of UAs. Three substantial review articles will be used to update readers on the current laboratory performance of UAs.
A recent systematic review, by Cuevas-Suarez and colleagues,37 of shear bond strength testing to dentine, has updated a 2015 review by the same group. They identified 9284 publications, 81 of which were read in full and 57 finally accepted for the review. Their results indicated that:
The bond strength to dentine was affected by the bonding strategy and the pH of the adhesive used, with the etch- and-rinse approach improving the bond strength to dentine of intermediately strong universal adhesives;
When an etch-and-rinse approach is used, the acid etching step solubilizes the mineral content of dentine (including the smear layer), with subsequent application of the adhesive allowing monomer infiltration into the collagen network, replacing the water between the collagen fibrils;38
After this, in situ polymerization leads to the formation of a hybrid layer, which, in combination with the presence of resin tags within the dentinal tubules, provides the resin composite restoration adhesion.
Cuevas-Suarez and colleagues37 finally stated that ‘the new meta-analyses performed in this update demonstrated that the stability of multimode adhesives' bond strength to dentine depends largely on their pH’. On enamel, irrespective of the pH of the adhesive, bond strength was improved by prior phosphoric acid etching. On the other hand, dentine bond strength of mild UAs was not dependent on the adhesive strategy used, and these adhesives seemed to be the materials with better stability. Summarizing the results of their review, Cuevas-Suarez and colleagues37 provided the following helpful recommendations to clinicians:
‘when applied to dentine, prior acid etching before the use of intermediately strong and ultra-mild universal adhesives it is not recommended’; and,
‘selective etching of enamel followed by the application of a mild universal adhesive currently appears to be the best choice to effectively achieve a durable bond to tooth tissues since bonding performance of mild universal adhesives could be improved by using the selective enamel-etch strategy. When applied to dentine, mild universal adhesives seem to provide better stability in both etch-and-rinse and self-etch strategies’.
Nagarkar and co-workers21 reviewed the laboratory testing and clinical performance of UAs. They identified 1250 articles, including 285 for final data analysis, of which, 12 were clinical studies (vide infra). They pointed out that chemical bonding promoted by 10-MDP was more effective and stable in water than that provided by other functional monomers, but concluded that, overall, for durable bonding with UAs, laboratory studies recommend the use of a selective enamel-etching strategy for permanent teeth, and an etch and rinse strategy for primary teeth. They concluded that ‘available laboratory and clinical evidence does not support the claim that UAs can be used with any adhesive strategy’.
Van Meerbeck and colleagues24 reviewed the pros and cons of UAs. They considered that, while the etch and rinse strategy was ‘undoubtedly’ the best bonding strategy to enamel, the resultant thick and hydroxyapatite-free hybrid layer formed on dentine was highly sensitive to degradation with time.
Finally, recent laboratory studies include the work by Lago and co-workers39 who compared the shear bond strength of six UAs to dentine, using Clearfil SE Bond (Kuraray) as control. The results indicated highest bond strength values for Scotchbond Universal (3M) (33.9MPa), but this was not significantly different to Clearfil Universal (Kuraray) and Tetric N-Bond (Ivoclar-Vivadent). All six UAs provided superior bond strength values to the Clearfil SE control.
In summary, therefore, laboratory studies appear to confirm that the bond strengths obtained by UAs are generally an improvement over those previously attained, with a selective enamel etch strategy being preferred.
Clinical studies
While laboratory data may provide an indicator regarding the performance of a given material, there is no substitute for clinical evaluation, given the tenuous association between in vitro and in vivo studies.40 The previous paper4 cited Loguerico and colleagues,41 Perdigão and colleagues42 and Lawson et al,43 in demonstrating the short-term clinical success of Scotchbond Universal (SBU). Recently published clinical research on UAs, with evaluation periods of greater than 2 years, includes the following:
The laboratory work of Loguerico and co-workers,29 and Munoz and co-workers,31 could be considered to be in agreement with results, published in 2017, of a randomized controlled trial by Burke and colleagues from a practice-based research group19 who used a split mouth design study to assess restorations (mainly in loadbearing cavities in posterior teeth) bonded with SBU (3M) in self-etch mode (ie no etching with phosphoric acid) or total etch mode (all surfaces in the cavity etched with phosphoric acid). The results indicated that, when 45 restorations were evaluated at 3 years, there was no difference in the quality of the margins;19
However, the numbers were relatively small in comparison with a recent publication by Matos and colleagues,20 who placed a total of 200 class V restorations in 39 patients and evaluated these at 5 years. There were four different treatment groups, namely:
– SBU etch and rinse + moist dentine;
– SBU etch and rinse + dry dentine;
– SBU selective enamel etch; and
– SBU self-etch.
The recall rate was 86%, with 19 restorations (of 153 assessed) lost, and the results indicated that the SBU adhesive performed worse in self-etch mode. Significant differences were also observed for both marginal staining and adaptation, with the clinical behaviour of this UA being better in etch and rinse mode when compared with the self-etch category. The authors therefore recommended that, if a self-etch strategy was used, selective enamel etching be employed.
Ruschel et al44 carried out a 3-year evaluation of UAs in NCCLs, involving 63 patients who had 203 NCCLs restored using resin composite and one of two UAs, Scotchbond Universal (SBU, 3M) and Prime&Bond Elect (PBE, Dentsply Sirona) used in either self-etch or etch and rinse modes. At the 3-year review, 150 restorations were assessed. Three restorations in the PBE self-etch group failed due to loss of retention, and restorations with etched margins were more likely to score optimally for marginal discolouration than in the self-etch groups;
Atalay and co-workers45 compared the 3-year performance of a UA used with different adhesive strategies in NCCL. They placed 165 restorations in 35 patients, using three etch protocols, namely: selective enamel etch; etch and rinse; and self-etch, placed using Single Bond Universal (3M), known in the UK as Scotchbond Universal. A recall rate of 98% was achieved, with three restorations (one from each group) having failed due to loss of retention. For all groups, only one criterion was significantly different. Restorations in the self-etch mode showed ‘less satisfying’ performance for marginal staining and marginal adaptation;
Zanatta et al46 evaluated the bonding performance of three adhesives, SBU (3M) (a UA system), Adper Single Bond (3M) (an etch and rinse) and Clearfil SE Bond (Kuraray) (self-etch) in a total of 152 restorations in 34 patients. The results indicated that the UA system performed similarly to the ‘conventional’ etch and rinse or self-etch systems;
Oz and colleagues47 examined 20 patients in a randomized controlled prospective trial, where each had a minimum of seven NCCLs, giving a total of 155 restorations. Seven different adhesives and application modes were employed. The recall rate was 82%. The results indicated that the cumulative retention rate for the self-etch groups was significantly lower than for the other experimental groups. The authors concluded that GLUMA Universal (Hereaus Kulzer, Germany) and All-Bond Universal (Bisco, IL, USA) showed better results in etch and rinse and selective enamel etch modes, compared with the restorations placed in the self-etch mode, concluding that the strategies in which the enamel was etched provided better clinical outcomes, including retention, marginal adaptation and marginal staining;
Perdigão et al,48 in a randomized controlled trial, assessed restorations of NCCLs in 39 subjects using four different etch protocols and evaluated whether an additional layer of hydrophobic bonding resin improved clinical behaviour. The cumulative failure rate was 8.6%, with retention rate being worst for the self-etch category. The authors concluded that ‘phosphoric acid etching is still recommended to provide retention for composite restorations in NCCLs;’
Van Dijken and Pallesen49 examined the clinical performance of a UA (All Bond Universal, Bisco) with the control, the two-step self-etch adhesive Optibond XTR (Kerr). A total of 114 ‘extended’ class II resin composite restorations were assessed at 3 years. Eight restorations failed, principally due to composite fractures. The success rate of the restorations placed with the UA adhesive was 94.7% and the control 91.2%. The authors concluded that the class II restorations placed using a one-step UA showed good short-term performance;
Finally, Szesz and colleagues50 carried out a systematic review and meta-analysis, identifying 2689 articles but retaining only 10, in order to identify if selective etching of enamel margins improves the retention rates of cervical composite restorations in NCCLs. While their findings related to self-etch adhesives, it may be considered that their results are pertinent to UAs used in self-etch mode. They concluded that selective enamel etching prior to application of self-etch adhesive systems in NCCLs can produce composite restorations with better aesthetics (lower marginal discoloration rates and better marginal integrity) and higher longevity (higher retention rates).
In summary therefore, there is a strong body of evidence that indicates that recently developed UAs provide clinical effectiveness as good as, or better, than previous ‘gold standard’ adhesives, and that selective etching of the enamel is desirable, given that the results presented above indicate improved retention rates of class V restorations when the margins are etched, and reduced levels of discolouration around the margins of all restorations. The present authors therefore strongly recommend this procedure. Does that statement apply to all UAs? It is the authors' view that, in view of the similarities between many of the UAs (Table 121,22), and the fact that their pH values tend to lie between 1.5 and 3, it is prudent to suggest that this is carried out if the clinician wishes to limit marginal staining over time.
Handling evaluations
There have been four ‘handling’ evaluations of UAs51,52,53,54 by a UK-based practice-based research group, the PREP (Product Research and Evaluation by Practitioners) Panel. The first51 involved SBU soon after its release, with 12 evaluators placing a total of 875 restorations (class 1:172; class II:189; class III: 134; class IV: 178; class V: 182; other: 20) and rating the material on visual analogue scales. The results indicated that the bonding agent used prior to the evaluation scored 4.0 out of 5.0 (where 5 indicated optimal ease of use), with SBU scoring 4.9. More recently, G-Premio Bond (GC, Leuven, Belgium), Prime&Bond Active (Dentsply Sirona) and Zipbond (SDI, Melbourne, Australia) have been evaluated,52,53,54 with ease of use scores being 4.9, 4.8 and 4.9, respectively. It may therefore be concluded that the UAs tested, and possibly UAs in general, score highly for ease of use.
Finally, it has been considered that patient- and operator-related factors may have a higher impact on restoration longevity than the actual adhesive employed,55 therefore, with regard to the clinical use of UAs, it is worth adding that, while isolation with rubber dam is optimal (although not universally used56) and moisture control (by whatever means) is essential, it may be considered that a further advantage is the reduced number of steps, and concomitant reduced technique sensitivity of these new adhesive systems.
Recent innovations
A radiopaque dentine adhesive
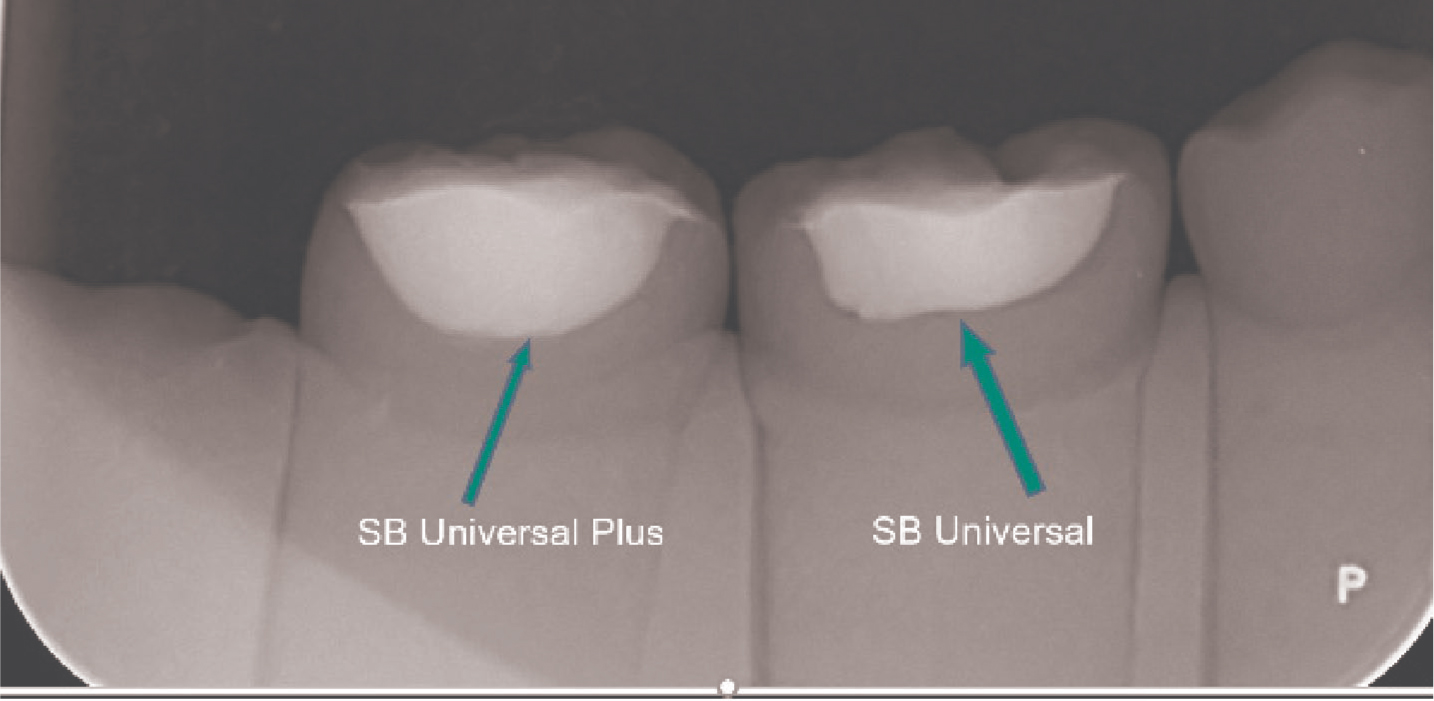
3M have recently introduced Scotchbond Universal Plus, which bears similarities to Scotchbond Universal, except that a radiopaque resin has been incorporated, substituting the BisGMA in the original version, and the silane has been improved, along with the adhesive's ability to bond to carious dentine, according to manufacturer's data. The addition of the radiopaque resin helps clinicians avoid any doubt regarding whether a radiolucent layer at the base of a posterior composite restoration is a pool of (non-radiopaque) resin or residual/secondary caries (Figure 4).
Figure 4. Comparison of radiopacity between Scotchbond Universal (original) and Scotchbond Universal Plus.
Back to the future?
GC have followed the ‘wish list’ for an ideal dentine adhesive published by Van Meerbeck and colleagues24 in which they stated the following:
The ideal adhesive system should contain:
A separate primer, which has the following features:
– It acts as the adhesion promoter and allows use of selective enamel etching;
– chemical bonding based on 10-MDP;
– photo-initiators, to ensure all areas, even in the deeper parts of the hybrid layer, will be covered.
A separate bonding agent that can be light cured immediately with the following features:
– Solvent-poor/free adhesive resin, hydrophobic to reduce the water uptake;
– applied in a sufficiently thick layer, this provides stress-absorbing potential;
– a good seal of the interface.
GC's recently introduced G2-Bond Universal appears to have been modelled on these features. In this, a hydrophilic primer containing 4META, MDP, MDTP, dimethacrylates, water, acetone, photoinitiator and filler has been designed to wet and self-etch the tooth surface. A second bottle containing dimethacrylates, BisGMA, fillers and photoinitiator is then applied. Interestingly, this contains no solvent. In common with other UAs, clinicians may use whichever mode of etching that they wish.
Universal adhesives as zirconia/ceramic primers?
It is beyond the scope of this article to address these topics in detail. However, in short, given that the resin 10-MDP has a demonstrable adhesion to zirconia by ionic and hydrogen bonding,57 UAs containing this resin may act as zirconia primers. On the other hand, the bond strength has been shown to reduce following 6 months' storage in water58 and a further study questioned whether UAs containing 10-MDP produced a significant effect regarding bonding to zirconia.59 It would therefore appear that more work is required to solve one of dental materials' most problematical problems, namely, how to achieve a reliable bond of resin to zirconia.
Two UAs contain a silane in their list of components, namely Clearfil Universal (Kuraray) and Scotchbond Universal/Universal Plus (3M). These UAs could therefore be used as primers for materials such as glass ceramics, alumina ceramics and lithium disilicate, especially when used in conjunction with the resin luting material from the same manufacturer.
MMPs: friend or foe
Matrix metalloproteinases (MMPs) are proteolytic enzymes, found in dentine, that can lead to the destruction of collagen (ie the organic matrix) in dentine when the pH is low. Destruction of the collagen in the hybrid layer can result, potentially leading to a reduction in bond strength, and which could be extrapolated to failure of adhesive restorations. As a result, MMP inhibitors have been proposed by some workers, adding an extra step in a dentine bonding protocol, such as the application of chlorhexidine. Most of the work on this subject has been carried out in vitro; however, a meta-analysis has failed to endorse the use of MMP inhibitors.60 Clinicians may therefore breathe a sigh of relief that their dentine bonding has not been made more difficult!
If bonding is as good as this, what are the clinical applications?
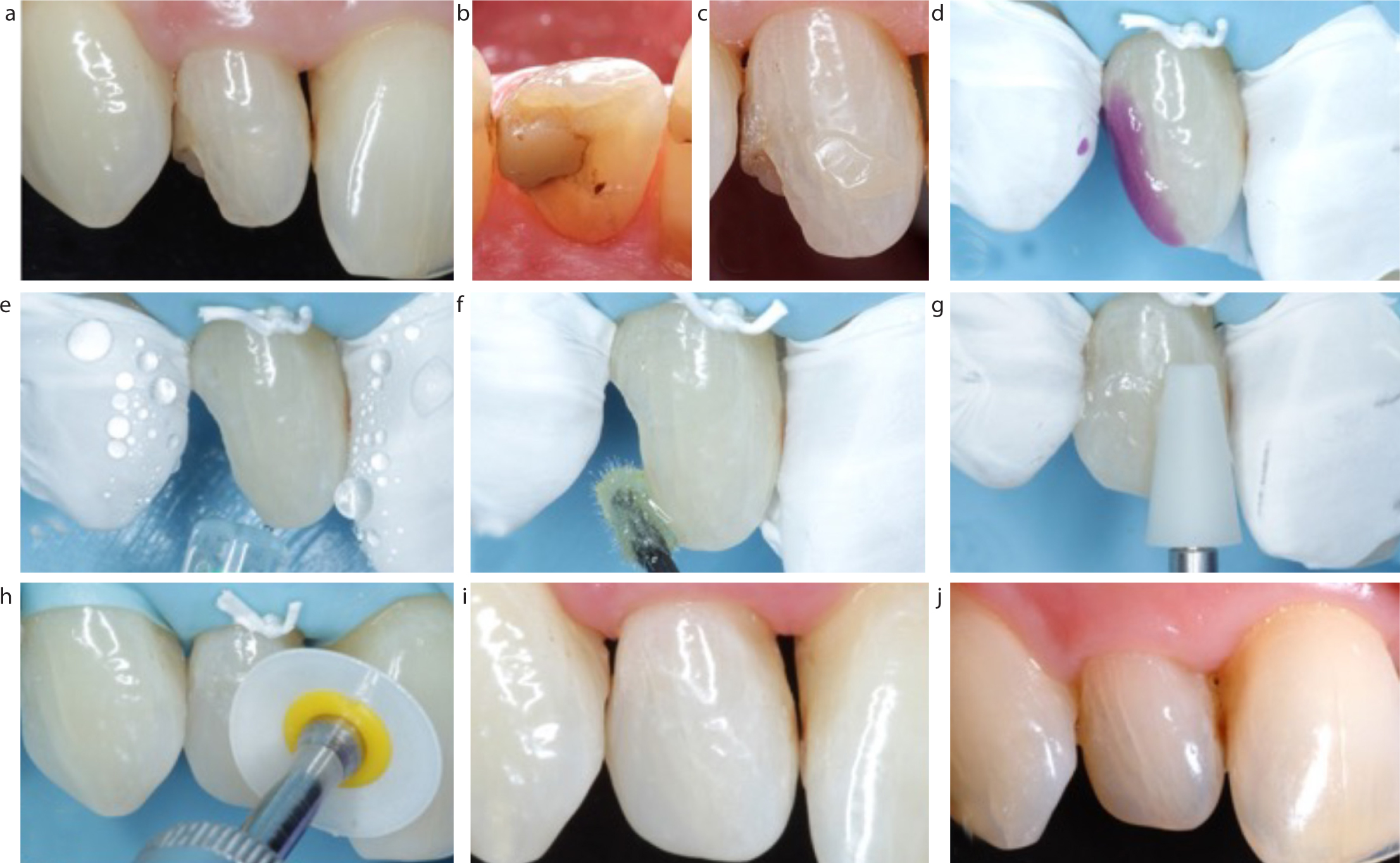
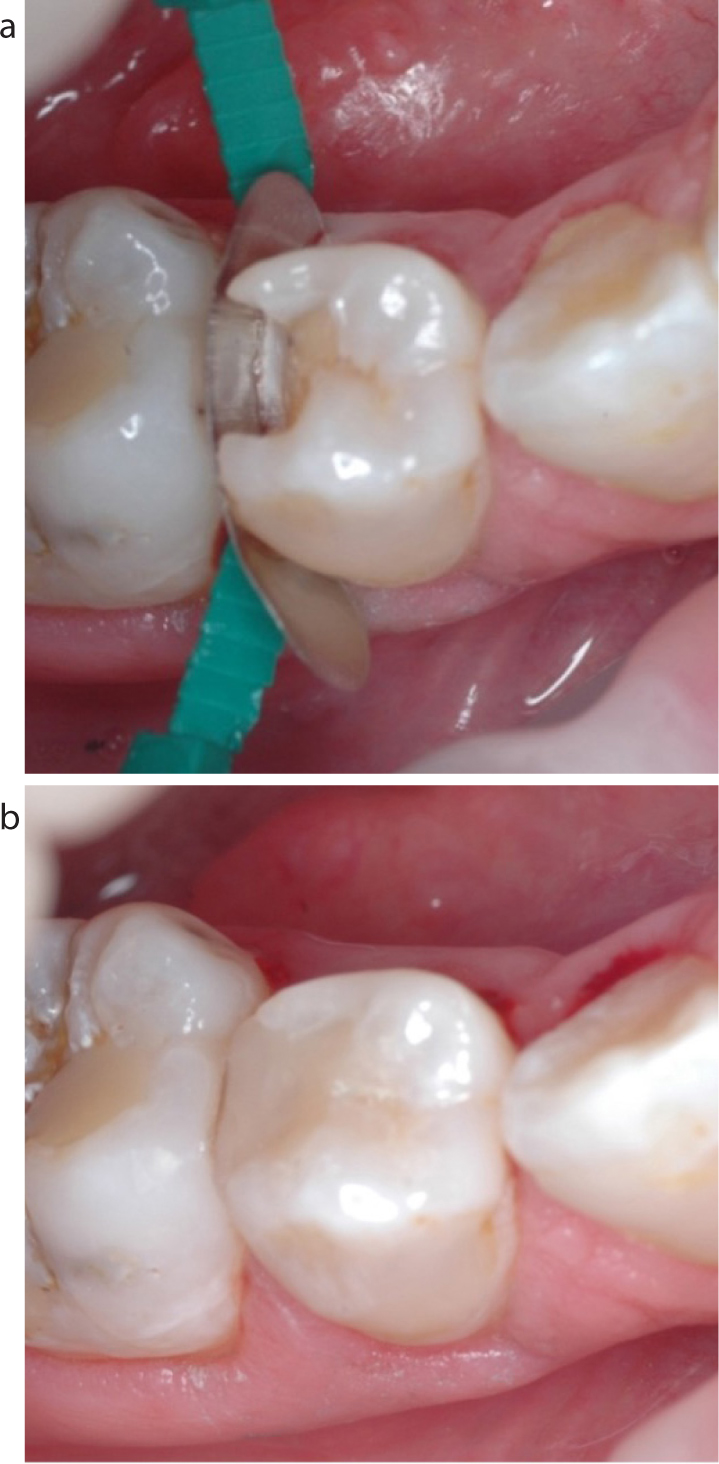
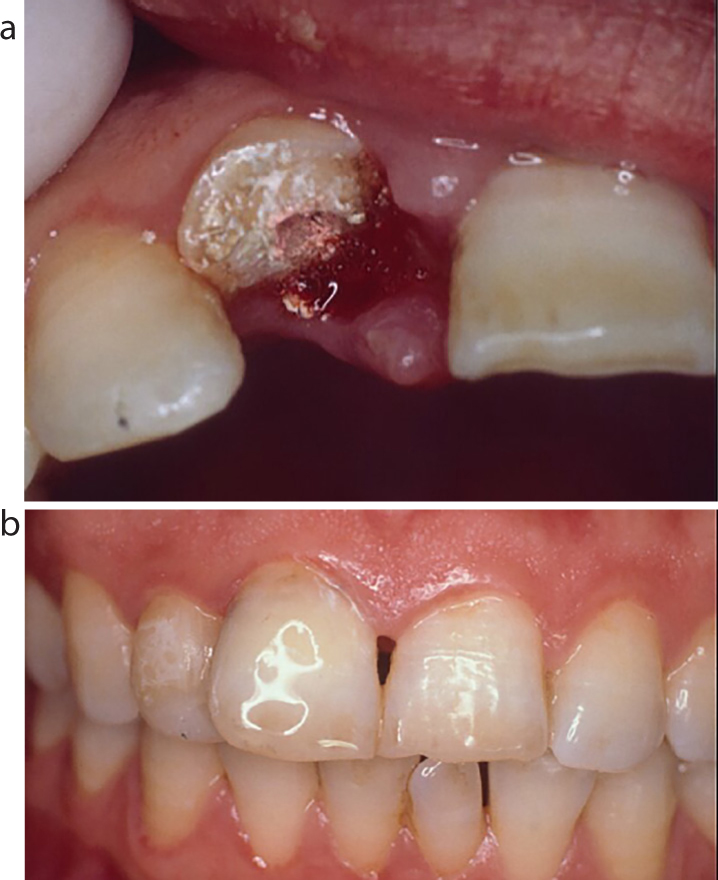
Figures 5–8 present a variety of the clinical applications that could be appropriate to today's universal adhesives.
Figure 5. (a–j) Stages in a bonding restorative procedure.Figure 6.
(a, b) This 35-year-old patient presented with palatal erosion (with large areas of dentine exposed) affecting his upper anterior teeth, and chipped incisal edges. Using a dentine adhesive, the worn palatal surfaces were restored with resin composite and the incisal edges of UL3 to UR3 restored with resin composite at an increased occlusal vertical dimension. The patient received oral hygiene instruction. This improved as his tooth sensitivity decreased following treatment.Figure 7. Dentine adhesives facilitate the use of non-retentive cavities with no resistance to distal displacement. (a) Non-retentive minimally invasive cavity design. (b) Cavity restored with resin composite.Figure 8.
(a) UR1 fractured in cycling accident. Fragment retained by patient. (b) UR1 root filled, electrosurgery carried out to expose fracture margin and fragment replaced using dentine and enamel bonding. Illustration taken after 2 weeks. The repair was successful for 2 years, following which further trauma led to loss of the tooth. However, it is thought to be psychologically good for the patient to have their own ‘tooth’ replaced.
Conclusions
In summary, universal adhesives hold promise and:
Can be used in total etch, self-etch, selective enamel etch modes, depending on the clinician's choice. The need to selectively etch the enamel has been demonstrated to be beneficial in many of the studies quoted in this review, both from the point of view of retaining class V restorations, but also because marginal staining and defects will be reduced;
In addition, in view of the potential to cause post-operative sensitivity as a result of (over) etching dentine, particularly in posterior teeth, it is the authors' view that this is not necessary or desirable and that selective enamel etching is the method of choice;
Some are compatible with direct and indirect procedures, when used with a designated resin luting material from the same manufacturer as the bonding agent because this will contain a separate activator;
May be suitable primers for silica and zirconia;
Can bond to different substrates, such as metal.
However, as with any new material or technique, more long-term clinical evaluations (alongside those referenced above) are needed to adequately demonstrate the value of these universal adhesives.