Cohen DW.Washington DC, USA: Walter Reed Army Medical Center; 1962
Gargiulo AW, Wentz FM, Orban B Dimensions and relations of the dentogingival junction in humans. J Periodontol. 1961; 32:261-267 https://doi.org/10.1902/jop.1961.32.3.261
Vacek JS, Gher ME, Assad DA The dimensions of the human dentogingival junction. Int J Periodontics Restorative Dent. 1994; 14:154-165
Makigusa K. Histologic comparison of biologic width around teeth versus implant: the effect on bone preservation. J Implant Reconstr Dent. 2009; 1:20-24
Jepsen S. New classification of periodontal and peri-implant diseases and conditions. Guidance for Clinicians.: European Federation of Periodontology. Today; 2019
Eaton KA, Ower P. Practical Periodontics E-Book. Elsevier Health Sciences. 2015; 179
Claffey N, Shanley D. Relationship of gingival thickness and bleeding to loss of probing attachment in shallow sites following nonsurgical periodontal therapy. J Clin Periodontol. 1986; 13:654-657 https://doi.org/10.1111/j.1600-051x.1986.tb00861.x
Jorgic-Srdjak K, Plancak D, Maricevic T Periodontal and prosthetic aspect of biological width part I: violation of biologic width. Acta Stomatol Croat. 2000; 34:195-197
Nevins M, Skurow HM. The intracrevicular restorative margin, the biologic width, and the maintenance of the gingival margin. Int J Periodontics Restorative Dent. 1984; 4:30-49
Wagenberg BD, Eskow RN, Langer B. Exposing adequate tooth structure for restorative dentistry. Int J Periodontics Restorative Dent. 1989; 9:322-331
Misch CE, Perel ML, Wang HL Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant Dent. 2008; 17:5-15 https://doi.org/10.1097/ID.0b013e3181676059
Hermann JS, Buser D, Schenk RK Biologic width around titanium implants. A physiologically formed and stable dimension over time. Clin Oral Implants Res. 2000; 11:1-11 https://doi.org/10.1034/j.1600-0501.2000.011001001.x
Jepsen S, Caton JG, Albandar JM Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. 2018; 45:S219-S229 https://doi.org/10.1111/jcpe.12951
Supracrestal tissue attachment (STA) is a relatively new term that was introduced in 2017 following the World Workshop on the Classification of Periodontal and Peri-implant Diseases and Conditions, co-sponsored by the American Academy of Periodontology (AAP) and the European Federation of Periodontology (EFP), which included expert participants from all over the world. It has replaced the term biological width, and refers to the junctional epithelium and supracrestal connective tissue. This article provides an updated review of the anatomy of STA, highlights the negative effects of violation and discusses its clinical relevance in restorative dentistry, including the use of crown lengthening. The impact of implants on STA is highlighted, and a summary of the relevance of STA in implant dentistry is also discussed.
CPD/Clinical Relevance: To allow dental practitioners to have more confidence providing adequate function, comfort, and aesthetics in the dentition, while maintaining periodontal health.
Article
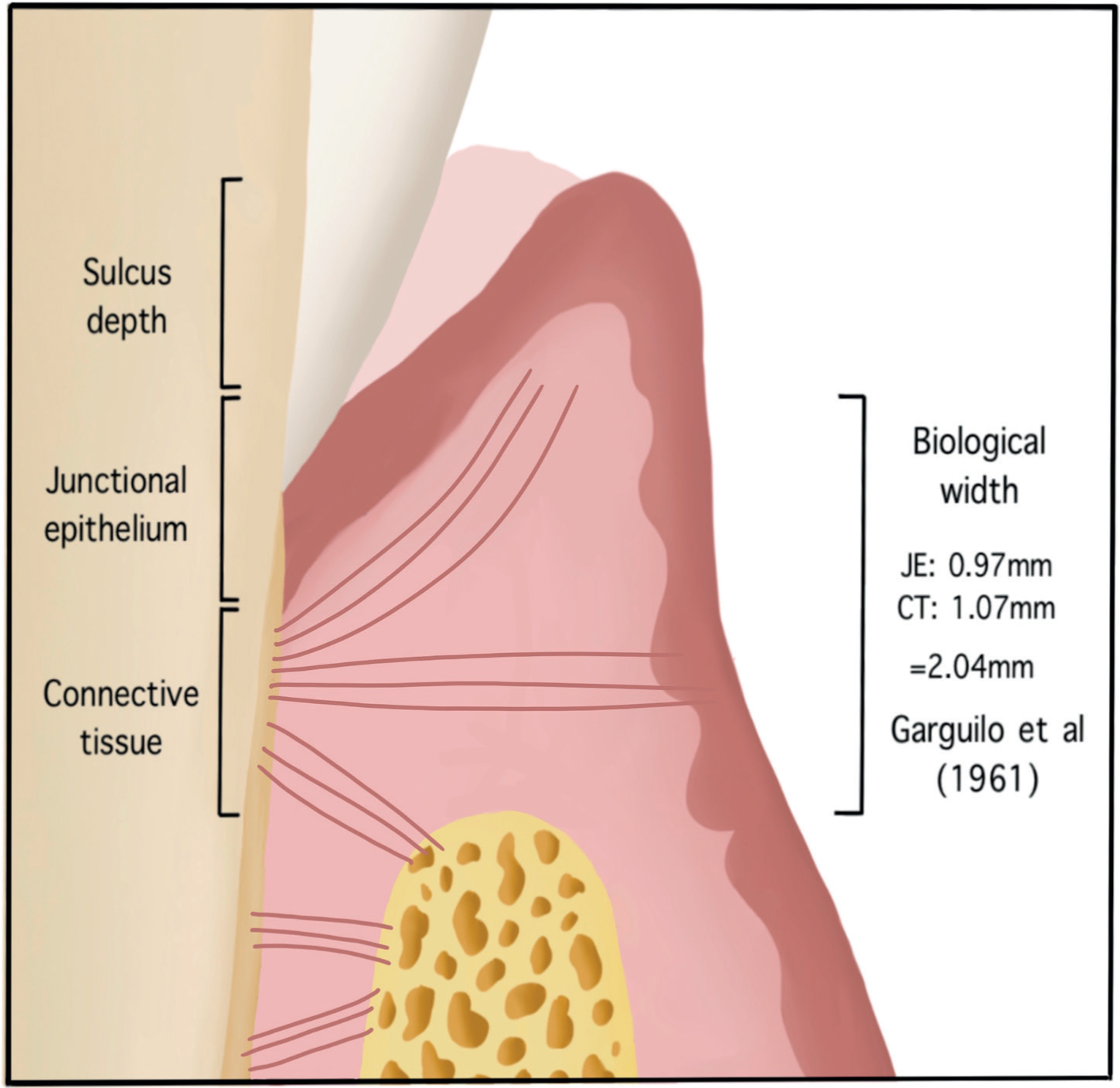
In 1962, Cohen introduced the term ‘biological width’, which describes the biological attachment of the soft tissues to the root of the tooth and comprises the junctional epithelium and connective tissue attachment, and this being equivalent to the distance between the base of the gingival sulcus and the alveolar bone crest.1 This term was coined following the work by Gargiulo et al in 1961, in which the width is referred to as the dentogingival junction.2 The dentogingival junction can be divided into two components: the connective tissue attachment and the epithelial attachment.
The term ‘biological width’ was updated in 2017 at the World Workshop on the Classification of Periodontal and Peri-implant Diseases and Conditions, to ‘supracrestal tissue attachment’ (STA), referring to the junctional epithelium and supracrestal connective tissue. The workshop was co-sponsored by the American Academy of Periodontology (AAP) and the European Federation of Periodontology (EFP) and included expert participants from all over the world. This article focuses on the clinical relevance of understanding the STA, particularly in the periodontal and restorative interface of dentistry.
Anatomy of biological width
The work that led to the term ‘biological width’ was based on the research of Gargiulo et al in 1961. This study researched the dimensions and relationship of the dentogingival complex on human cadavers, analysing specimens from 287 teeth. This pioneering work demonstrated a proportional relationship between the alveolar crest, connective tissue attachment, epithelial attachment and the sulcus depth. The mean dimensions from this study were 0.69 mm sulcus depth, 0.97 mm epithelial attachment and 1.07 mm connective tissue attachment. Based on this work, the average biological width is reported to be 2.04 mm; the sum of the epithelial attachment and connective tissue attachment (Figure 1).2 Despite an average, biological width dimensions are unique to each individual, and in 1994, Vacek et al showed these dimensions ranged from 0.75 mm to 4 mm.3
Figure 1. Diagram illustrating the dimensions based on the research of Garguilo et al.1
While it is useful to have these values as a reference, as is always the case in dentistry, it is important to consider genetic and anatomical variation and assess as far as possible each case on an individual basis.
For example in cases of altered passive eruption, where the clinical crown height is reduced, diagnosis depends on clinical and radiographic examination to determine the relationship of the gingival margin, cemento-enamel junction, and the bone ridge. The clinical crown height is compared with the radiograph and a gingivectomy may be performed with osseous resection as necessary in order to re-establish appropriate dimensions of STA in relation to the alveolar bone margins.
Clinical relevance
STA is a form of human tissue barrier that serves to protect against infection and other foreign materials, acting dynamically to maintain a constant distance.4 If this distance is infringed, a cellular reaction to re-establish the desired distance between the margin of the restoration and the bone crest will occur. The importance of the STA becomes clinically relevant particularly when considering the margin of restorations in restorative dentistry.
Margin types
There are three options for the placement of the restorative margin: supragingival, equigingival and subgingival. From a periodontal view, supragingival and equigingival margins are well tolerated, especially since the introduction of adhesive resin cements has meant that restorations can be finished on the tooth with a smooth polished interface, reducing any aesthetic concerns. However, considerations for root caries, retentive factors and aesthetics can dictate whether a margin lies subgingivally. This poses the risk of violating the supracrestal tissue attachment, which occurs when the filling, crown or bridge margin lies within the supracrestal connective-tissue attachment. 5
Supracrestal tissue violation
If supracrestal tissue violation occurs, it can lead to irreversible loss of periodontal attachment, pocket formation, inflammation, osseous resorption and occasionally, root resorption.6 Recession is seen more commonly in patients with a thin gingival tissue biotype (gingival thickness of <1.5 mm), and inflammation and periodontal pocketing where there is a thick gingival biotype (gingival thickness >2 mm).7,8
Diagnostics and planning
If there is an area of localized gingival recession, or bone loss, with generally good oral hygiene, it is always important to consider whether this is related to an overextended restoration that is impinging on STA.
It is also worth considering STA in the planning stages for restorative treatment to prevent avoidable damage. A basic principle to avoid impinging on the supracrestal tissue attachment is to allow 3 mm of space between the restoration margin and the alveolar bone.3,9 This 3 mm represents 1 mm of connective tissue, 1 mm of junctional epithelium and 1 mm of gingival sulcus. There is, however, significant individual variation in STA presented in Gargiulo et al's study, especially at the epithelial attachment, therefore it may be appropriate to allow more than 3 mm. When subgingival margins are required, it is recommended that the extension should be limited to 0.5–1.0 mm. This is because it is impossible clinically for the dentist to differentiate between the sulcular and junctional epithelium and impinging on the junctional epithelium risks periodontal damage.10
Where crown margins impinge on the STA, a distinctive area of inflammation can be seen around the crown margins as can be seen around UR2 and UR1 in Figure 2. This is distinguishable from marginal gingivitis as inflammation is isolated to the crowned teeth/restorations impinging on STA, and often is not directly linked to plaque deposits. Correction of this will need consideration of optimising oral hygiene and considering the need for crown lengthening and crown replacement to address this impingement.
Figure 2. A clinical photograph to demonstrate gingival inflammation caused by the crowns on UR1 and UR2 impinging on the biological width.
If a lack of ferrule or subgingival margins is recognized during an earlier stage, additional measures, such as crown lengthening, can be conducted to prevent STA violation.
Crown lengthening
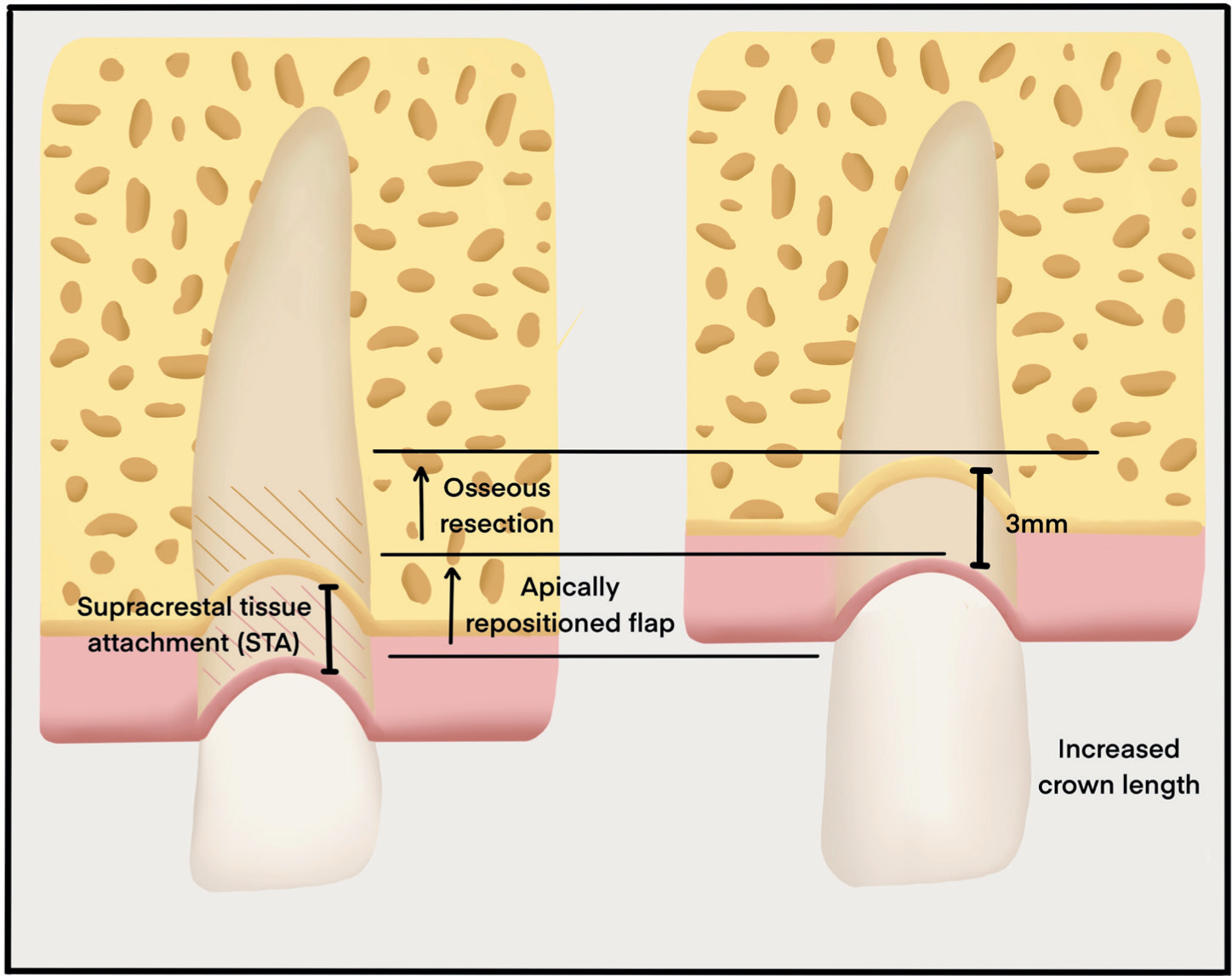
Crown lengthening involves surgically removing hard and soft periodontal tissue to increase the length of the crown and re-establish the supracrestal tissue attachment to maintain a ferrule.11 Teeth with subgingival caries, fractures, short clinical crowns with or without aesthetic deficiencies, and teeth shortened by incomplete exposure of the anatomical crown (eg altered passive eruption) are all candidates for surgical crown lengthening. To prevent invading the supracrestal tissue attachment, crown lengthening is indicated if the clinician believes that the final restoration will be at least 3 mm from the alveolar bone crest. Orthodontic extrusion should also be considered for these cases to prevent poor outcomes, such as gingival recession, poorer crown:root ratios and loss of bone support on adjacent teeth.6 Surgical methods for crown lengthening include gingivectomy, apically positioned flap surgery (APF), and APF with osseous reduction (Figure 3). Although the Gargiulo et al study established that the supracrestal tissue attachment is 2 mm, it is difficult to measure this clinically when preparing crown margins. Therefore, a figure of 3 mm is used (Figure 4), considering possible measurement error.7
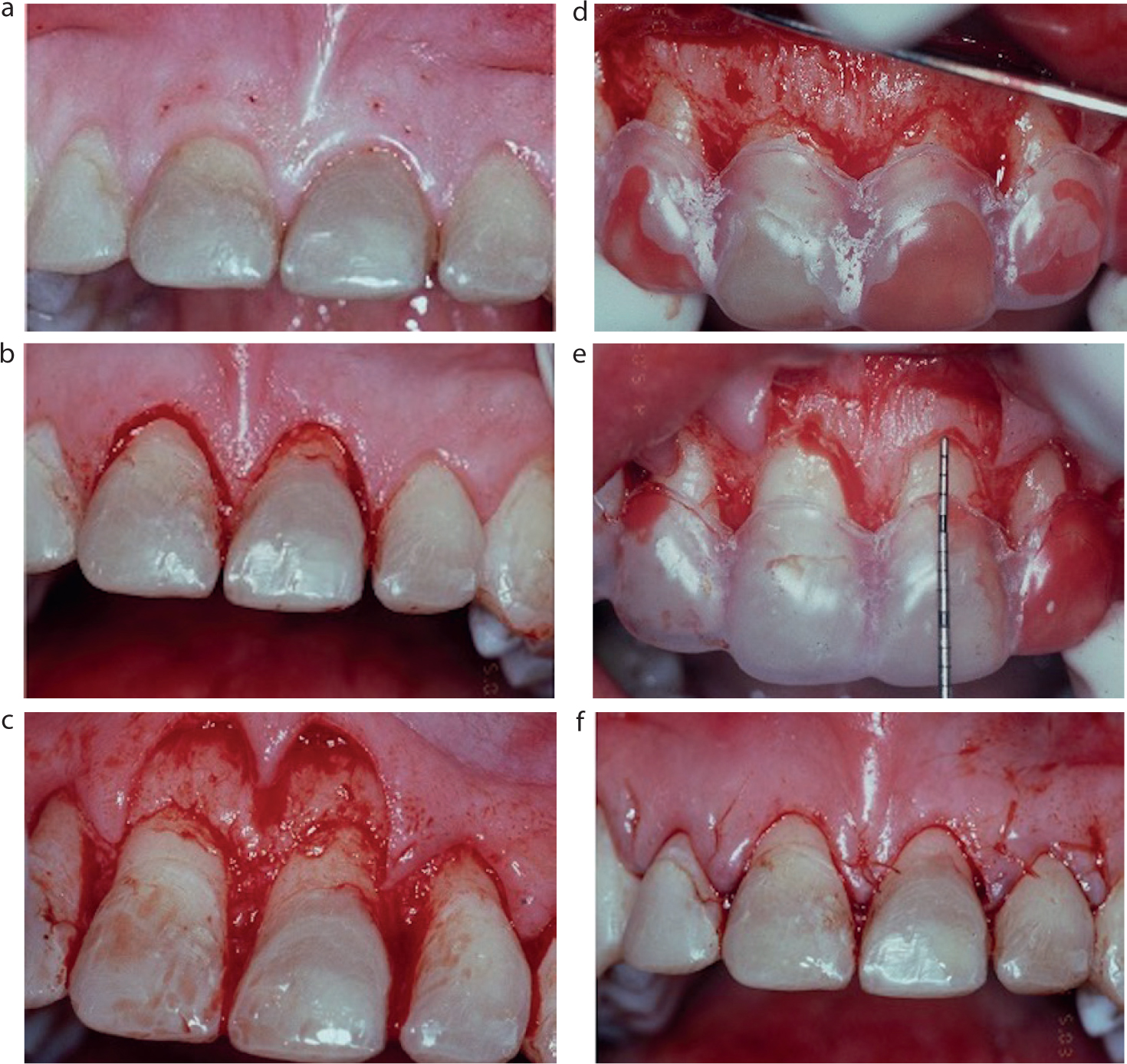
Figure 3. Diagram demonstrating the difference between the STA in healthy tissue and following crown lengthening. The measurements are based on the research of Garguilo et al and Misch et al.1,12Figure 4. Series of clinical photographs to demonstrate the crown lengthening procedure (APF with osseous reduction) on a patient with tooth surface loss. (a) Probe markings. (b) UR1 and UL1 incisions. (c) Flap raised. (d) Stent in situ before bone removal). (e) Stent in situ following bone removal demonstrating 3 mm of osseous reduction. (f) Simple interrupted intra-papillary sutures.
Implants
How does the STA interface change when comparing to an implant? Using animal subjects, Misch et al12 proposed that there could be a supracrestal tissue attachment surrounding the implant; however, evidence to validate this theory is mainly derived from animal studies (eg dogs13,14). It is recognized that implants ankylose via osseo-integration and there is limited or no connective tissue fibre attachment in the connective tissue zone where only two main connective tissue groups are a present: parallel and circular. The implant is seen to be sealed via epithelial hemi-desmosomes. Other differences recorded when comparing the natural tooth to an implant are:
A lack of PDL leading to a decrease in protection from occlusal forces;
A hypovascular, hypocellular tissue zone with an increase in collagen fibres, relative to that seen around the natural tooth.
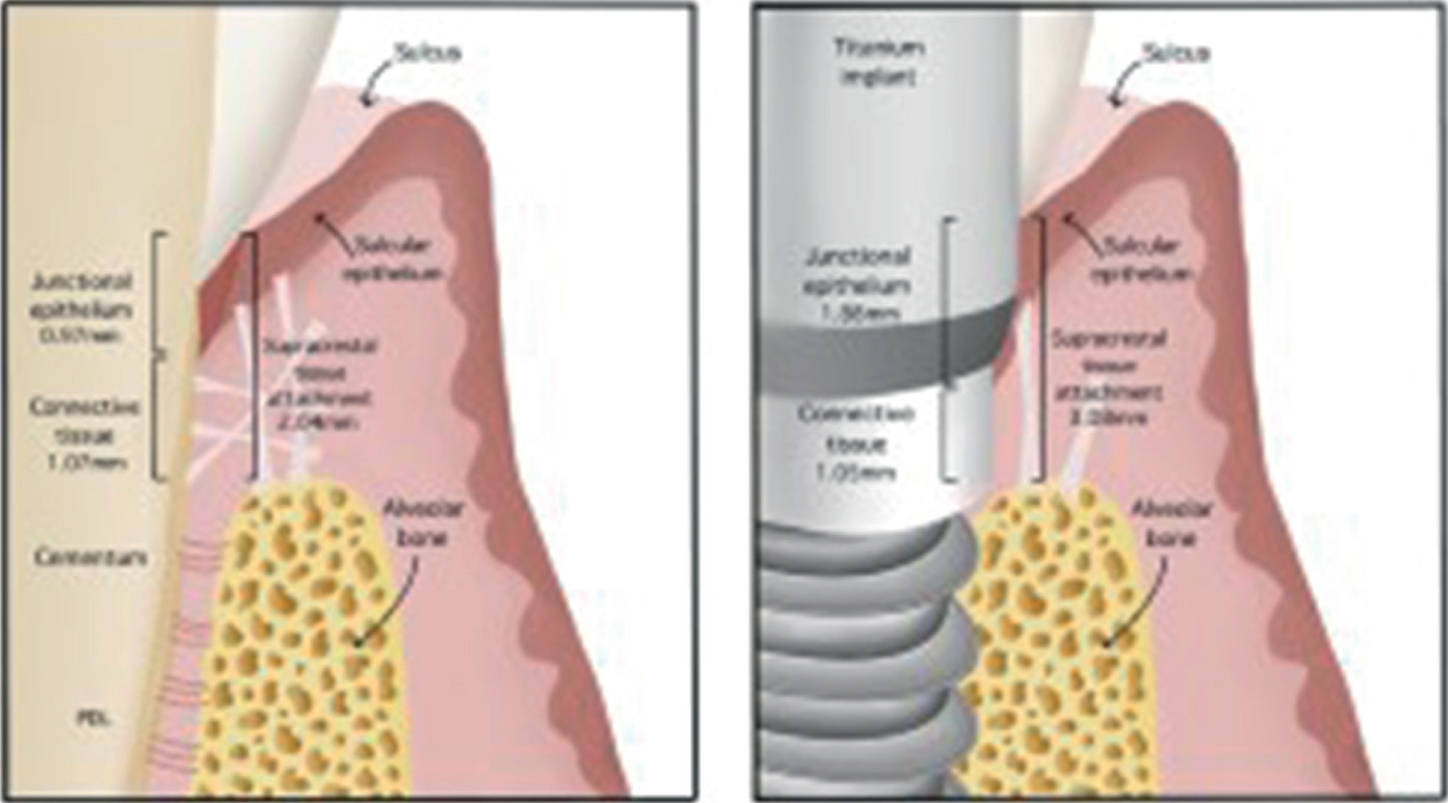
When looking at the soft tissue interface dimensions, Misch et al15 measured an average biological width of 3.08 mm, and Herman et al16 stated this could vary around implant type, for example one-or two-piece, or non-submerged and submerged. As mentioned, these tissues are less vascularized when compared to the natural tooth. With a reduction in the vascular network, thicker STA, and no connective tissue attachment, clinical probing depth can be increased, and thus bleeding on probing becomes less reliable around an implant (Figure 5).
Figure 5. Schematic demonstrating differences between supracrestal tissue attachment around teeth and implants.
It is essential to have in-depth knowledge of the interactions of the periodontium when placing an implant to provide both long-term survival and aesthetics. However, it is also important for the wider dental team to have a general knowledge of the implant–perio interface. With a greater understanding, there is a better appreciation of how peri-implant disease may present, as well as progress, and moreover, will lead to more successful treatment and preventive outcomes for our patients.
EFP/AAP update and significance
As previously mentioned, the term biological width was recently updated to a more anatomically correct term, supracrestal tissue attachment by the EFP/AAP. In the consensus report from the 2017 World Workshop, there were considerations for other factors that could negatively affect the periodontium, when infringement occurred.17 The consensus stated that there was a lack of evidence to support whether negative effects on the STA are caused by dental plaque biofilm, trauma, toxicity or dental materials, or a combination of these factors.
Summary
Correctly designed restorations and crowns with margins that do not violate the STA can improve the success of restorative procedures. Consideration of crown lengthening is vital when periodontal tissues may be compromised due to restorative treatment. There are several other factors that can negatively impact the STA of which we must be aware. By applying our knowledge of STA, we can prevent iatrogenic damage and provide better restorative treatment for our patients.