Mattos CM, Santana RB A quantitative evaluation of the spatial displacement of the gingival zenith in the maxillary anterior dentition. J Periodontol. 2008; 79:(10)1880-1885
Chu SJ, Tan JH, Stappert CF, Tarnow DP Gingival zenith positions and levels of the maxillary anterior dentition. J Esthet Restor Dent. 2009; 21:(2)113-120
Chu SJ, Tarnow DP, Tan JH Papilla proportions in the maxillary anterior dentition. Int J Periodont Rest Dent. 2009; 29:(4)385-393
Tarnow DP, Magner AW, Fletcher P The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. J Periodontol. 1992; 63:(12)995-996
Gargiulo AW, Wentz F, Orban B Dimensions and relations of the dentogingival junction in humans. J Periodontol. 1961; 32:261-267
Wise MD Stability of gingival crest after gingival surgery and before anterior crown placement. J Prosthet Dent. 1985; 53:(1)20-23
Functional crown lengthening surgery in the aesthetic zone; periodontic and prosthodontic considerations Rajiv M Patel Paul Baker Dental Update 2024 42:1, 707-709.
Specialists in Periodontics, Clinical Demonstrators, Department of Periodontology and Preventive Dentistry, Guy's, King's and St Thomas' Dental Institute, Guy's Hospital, London
Crown lengthening surgery aims to increase the amount of supragingival tooth tissue by resection of the soft and/or hard tissues to enable otherwise unrestorable teeth to be restored by increasing the retention and resistance forms of the teeth. Restoration of the worn dentition may require significant prosthodontic knowledge and skill. A prosthodontist should be involved from the beginning of the management of the patient. A number of key stages should be considered for correct management. Although the periodontist may guide the prosthodontist with regards to what may or may not be possible surgically, the overall treatment plan should be prosthodontically driven.
Clinical Relevance: Toothwear of the anterior dentition provides a unique challenge to restore not only function but also to manage the aesthetic demands of the patient. To ensure that the correct outcome is reached, clinicians should be familiar with the normal anatomical proportions and relationships to enable planning and treatment to take place.
Article
Crown lengthening surgery aims to increase the amount of supragingival tooth tissue by resection of the soft and/or hard tissues to enable otherwise unrestorable teeth to be restored by increasing the retention and resistance forms of the teeth.
As restoration of the significantly worn dentition requires significant prosthodontic knowledge and skill; the restoring dentist should be involved from the beginning of the management of the patient and, indeed, lead treatment. Where necessary, the advice of a prosthodontist may also be sought.
Planning
Management of a patient with severe toothwear requiring crown lengthening surgery will require a number of planning stages:
Pre-prosthodontic planning;
Combined prosthodontic and periodontic planning;
Pre-surgical planning.
Pre-prosthodontic planning
The restoring dentist has a number of decisions to make regarding the rehabilitation of the worn dentition based on the extent of toothwear and its distribution, and the general restorative and endodontic status of the whole dentition. The occlusion will also have to be assessed prior to planning restorations. Where the existing intercuspal position (ICP) is unsatisfactory or does not exist due to excessive wear, centric relation may be used as the basis for reconstructing a new ICP. There are two other principles to consider when reorganizing the occlusion in this manner:
Decide the vertical dimension: Where there has been a loss of vertical dimension (reduced lower face height) it may be possible to increase it. Generally speaking, if the occlusal vertical dimension is being increased to produce teeth with ‘normal’ dimensions, the space required for the restorations will determine the increase.
Create stability in ICP and avoid damage in excursions: The occlusal scheme should be designed to optimize transmission of occlusal forces while providing stability and harmony in order to allow the patient to adapt. This may be a mutually protected scheme that in ICP will allow the posterior teeth to support maximum biting forces whilst the anterior teeth are just out of contact. In excursions, the anterior teeth provide guidance to disclude the posterior teeth and protect them from lateral loading. This may be important if attrition from parafunctional habits has been part of the aetiology of wear.
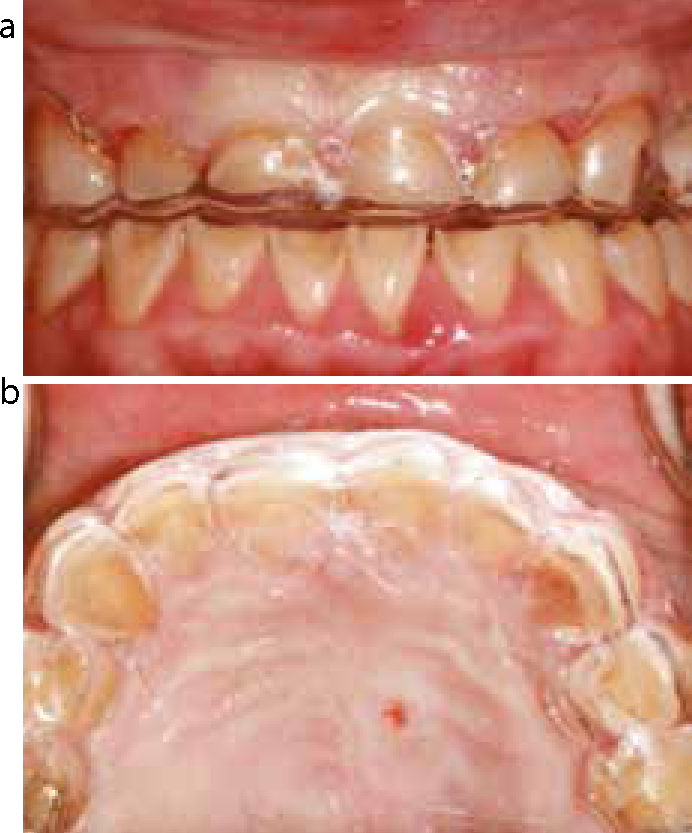
Study casts mounted on a semi- or fully adjustable articulator will allow the restoring dentist to determine some of the aspects outlined above and to construct diagnostic wax-ups. Chairside try-ins (with the aid of a blow down stent of the wax-ups filled with a temporary acrylic restorative material placed directly over the teeth) will allow the clinician and the patient to determine the appearance of the proposed restorations in relation to the soft tissues and lips. This is an important process as it informs the restoring dentist by how much the teeth must be lengthened at the gingival margin and by how much the length of the teeth can be increased from the incisal edge. Excessive tooth display (more than 2 mm) in relation to the upper lip at rest is an indication for crown lengthening surgery to allow tooth length to be increased at the gingival margin (Figures 1, 2, 3, 4).
Figure 1. Pre-operative view of the anterior dentition demonstrating severe tooth surface loss.Figure 2.
(a, b) Pre-operative view of the upper and lower occlusal surfaces demonstrating severe tooth surface loss consistent with erosive tooth loss.Figure 3.
(a) Upper occlusal view of diagnostic wax-ups. (b) Articulated casts with diagnostic wax-ups with tooth form restored to correct dimensions. (c) Lower occlusal view of diagnostic wax-ups.Figure 4.
(a) Modification of the gingival margin positions; an upper study cast to the proposed new gingival margin positions. (b) Construction of the acrylic surgical guide on the modified cast.
Combined prosthodontics and periodontic planning
The periodontist should liaise with the restoring dentist to ensure that the new proposed positions of the gingival margins are in the correct relationship to one another.
Principles of planning gingival aesthetics
Determining the position of the gingival zeniths: Studies examining gingival morphology in periodontal health have noted that the gingival zeniths of the upper central incisors are usually located approximately 1 mm distal to the midline of the crowns.1,2 These studies have also shown that the zeniths of the upper lateral incisor and upper canine teeth are located in the midline of the teeth, though they may appear distal when viewed from in front of the patient owing to the relative disto-angulation of the roots (Figure 5).
Relative gingival margins: The same studies mentioned above have also demonstrated that gingival zeniths of upper lateral incisor teeth are approximately 1 mm coronal to those of the upper central incisor and canine teeth (Figure 6).
Papillae height: Chu et al3 suggested that papillae length should be approximately 40% of the length of the crowns of the teeth. A study by Tarnow et al4 showed that papillae formation may be successful where the contact area between teeth is approximately 5 mm from the alveolar crest. These dimensions may help guide the restoring dentist to plan for crown morphology that will help achieve optimal (gingival) aesthetics (Figure 7).
Figure 5. Ideal gingival zenith points demonstrated by yellow line crossing gingival margin. Red line demonstrating relative position of gingival zenith point to midline of tooth.Figure 6. Gingival margins of the upper central incisor and canine teeth approximately 1 mm apical to the upper lateral incisor teeth.Figure 7. Illustration of the length of the central incisor papilla relative to the length of the crown.
Once a study cast has been modified (keeping in mind the principles discussed above) to create the new proposed gingival margin position, a blow down acrylic surgical stent can be created from the modified model to allow the proposed gingival margin position to be transferred with a degree of accuracy at the time of surgery.
Pre-surgical planning
Some of the surgical planning will be common to the prosthodontics planning (smile/lip line, general restorative/endodontic status). The patient's medical history should also be checked for any contra-indications to surgery. Poor oral hygiene should be addressed prior to surgery to allow easier handling of the tissues during surgery and allow adequate post-operative healing. Periodontal treatment should also be carried out prior to surgery if indicated. A healthy periodontium is a prerequisite to surgery.
Specific factors to consider:
Amount of keratinized tissue: Depending on the amount of tooth substance required by the restoring dentist, the amount of attached keratinized tissue will determine the surgical approach; resective versus apically positioning tissues (or a combination of both). It is preferable to leave at least 2 mm of keratinized tissue post surgery. This will enable the patient to maintain good plaque control more comfortably than if there was only lining mucosa remaining.
Pocket depths and bone sounding (with local anaesthesia): This allows the biologic width to be assessed. The biologic width is said to represent the tissue attachment as measured from the apical extent of the gingival sulcus to the alveolar crest. It comprises approximately 1.5 mm of junctional epithelial attachment and 1 mm of connective tissue attachment.5 The measurement does not include the sulcus or probing depth. Therefore the biologic width can be measured clinically by subtracting the probing depth from the depth to the alveolar crest. The biologic width can then be used to determine how much bone removal is required (if required) in order to maintain healthy marginal periodontium, eg a biologic width of approximately 3 mm plus a pocket depth of 2 mm would require bone adjustment such that a distance of 5 mm was present from the new gingival margin position to the alveolar crest. In thin gingival tissues, encroachment of restoration margin on the biologic width may result in gingival recession. In thick tissues it may result in chronic inflammation.
Extent of interproximal and palatal tooth tissue required: This information provided by the prosthodontist will help plan flap design (in association with the amount of attached tissue present). If no interproximal crown lengthening is required, it may be possible to design a flap that is papilla sparing. If interproximal space is required it is important to remember the cement-enamel junction (CEJ) runs more coronally interproximally and therefore bone levels should also remain more coronal relative to the mid labial and mid palatal crestal levels after ostectomy.
Peri-apical radiographs: Good quality peri-apical radiographs will allow assessment of the interproximal bone levels (and their relative positions to the CEJs) as well as root form and length. Short roots will severely limit the extent of crown lengthening that may be possible, otherwise teeth with dramatically reduced support and increased crown to root ratios may be produced. Teeth with narrow roots may be difficult to restore; restoration margins placed on roots may increase the risk of devitalization of the teeth. The emergence profile of the crown of the tooth will also be compromised and, in some instances, result in ‘dark’ interproximal triangles or voids (Figure 8).
Figure 8. Peri-apical radiographs of teeth to be crown lengthened.
Surgical procedure
Resective approach
Once planning has been completed, the surgical guide (constructed from the modified study cast) can be located on the teeth to be lengthened and the positions of the gingival margins marked out with a probe if a resective technique is proposed. The gingivae can then be resected to create the new gingival margin followed by full thickness flap elevation (maintaining papilla height if raised). Alveolar crest position can also be adjusted relative to the surgical guide to allow space for biologic width and the periodontal crevice.
The ostectomy (removal of bone supporting teeth) and bone recontouring may be carried out with a combination of bone chisels, burs and ultrasonic tips. Bone removal may also be required in the region between the roots to maintain a natural anatomy and contour of the bone and avoid ‘flat ledges’ or ‘platforms’ being formed. Exposed root surfaces should also be root planed to prevent re-attachment of the periodontal tissues and minimize the risk of rebound of the gingival margin to the pre-surgical position.
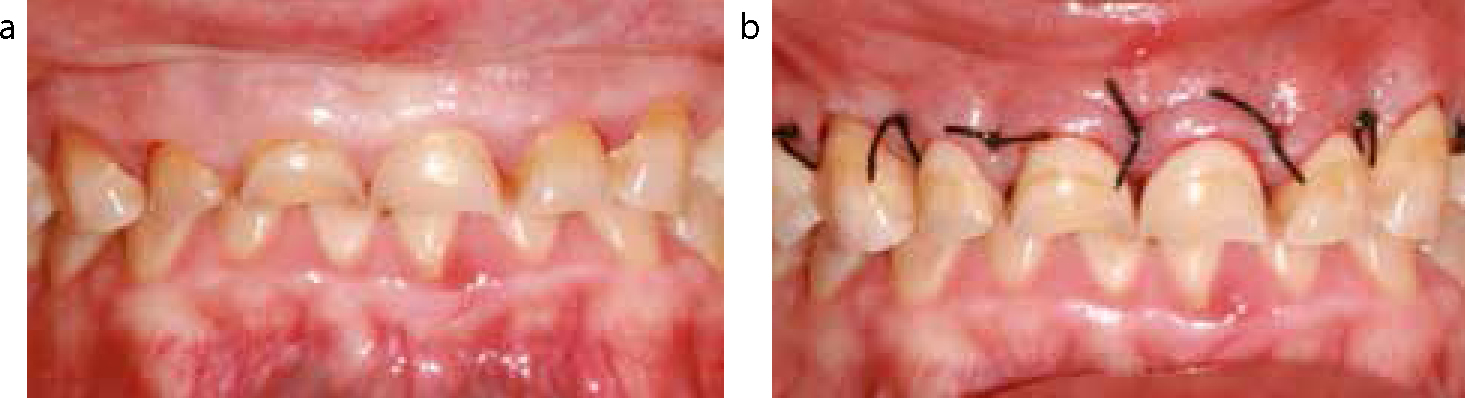
An everting vertical mattress suture technique may be useful in trying to maintain papilla height and position post surgically. Sutures are commonly removed 7–10 days post surgery.
Non-resective approach
If a resective technique is not possible owing to insufficient keratinized tissue, full thickness flaps raised from crevicular incisions or conservative inverse bevel incisions would have to be utilized. Apical displacement of the periodontal tissues (and exposure of further tooth tissue) may be achieved by elevating the flap past the muco-gingival junction and by incorporating vertical relieving incisions into the flap design. Management of the hard tissues would be as described above for the resective approach (Figures 9–13).
Figure 9.
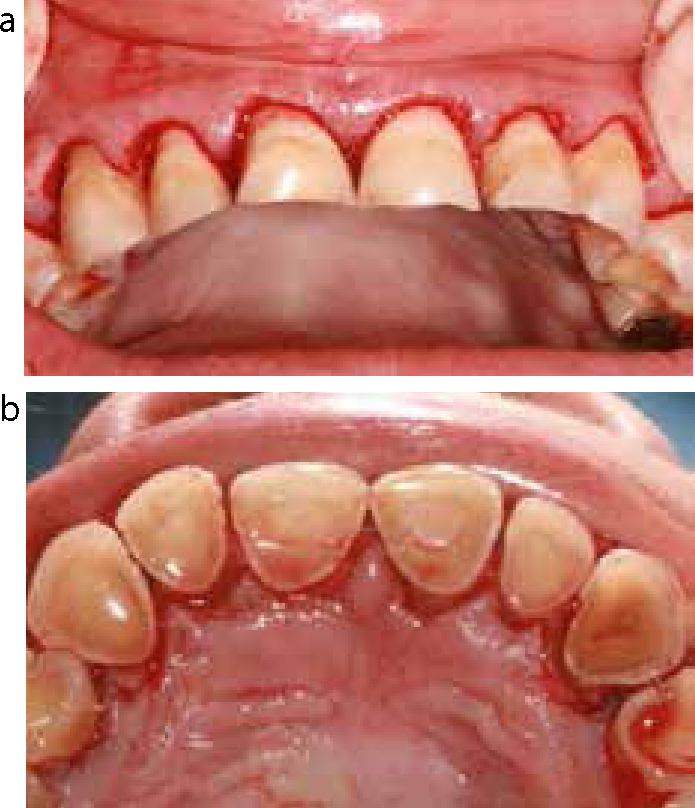
(a, b) Surgical guide in situ, buccal and palatal views providing a guide for the amount of gingiva to be resected both buccally and palatally.Figure 10.
(a, b) Gingival margin position following gingivectomy.Figure 11. Relationship of the new gingival margin position (demonstrated by the surgical guide) to the position of the alveolar crest.Figure 12. Appearance of the alveolar crest following completion of alveolar re-contouring (ostectomy and osteotomy).Figure 13.
(a, b) Immediate post-operative appearance in comparison to the pre-operative view demonstrating an increase in crown height.
Restorative phase
The crown lengthened teeth may be prepared soon after surgery (1–2 weeks) to allow the placement of provisional restorations if healing has occurred in an uncomplicated manner. The periodontist can provide the restoring dentist with advice on healing and when to proceed to provisional restorations.
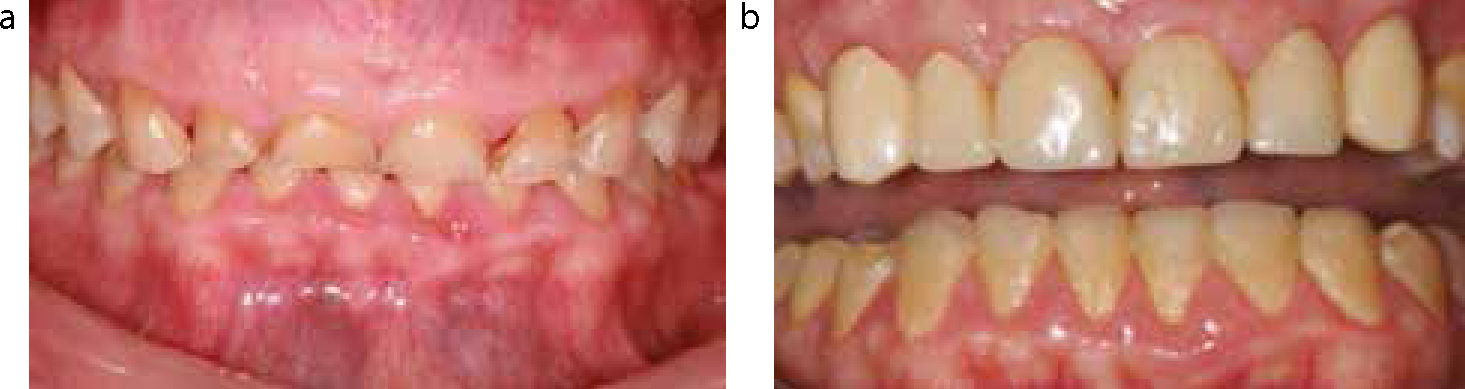
If crowns are considered, it would be worthwhile waiting six months prior to placement of the definitive restorations. There is limited research in this matter but a study by Wise6 demonstrated that the position of the gingival crest may continue to change (both coronal and apical movement) for up to five months post periodontal surgery, though it should be noted that this study did not look at crown lengthening surgery (Figure 14).
Figure 14.
(a, b) Comparison of pre-operative appearance with the appearance 6 months post surgery (provisional crowns in situ).
Conclusion
Planning the case from both prosthetic and periodontal aspects is key to a successful outcome. Though the periodontist may guide the restorative dentist with regards to what may or may not be possible surgically, the overall treatment plan should be prosthodontically driven.