Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of untreated caries: a systematic review and metaregression. J Dent Res. 2015; 94:650-658
Kidd E. The implications of the new paradigm of dental caries. J Dent. 2011; 39:3-8
Innes NPT, Evans DJP. Modern approaches to caries management of the primary dentition. Br Dent J. 2013; 214
Santamaría RM, Innes NPT, Machiulskiene V, Schmoeckel J, Alkilzy M, Splieth CH. Alternative caries management options for primary molars: 2.5-year outcomes of a randomised clinical trial. Caries Res. 2017; 51:605-614
Rosenblatt A, Stamford TCM, Niederman R. Silver diamine fluoride: a caries “silver-fluoride bullet”. J Dent Res. 2009; 88:116-125
Mei ML, Ito L, Cao Y, Lo EC, Li QL, Chu CH. An ex vivo study of arrested primary teeth caries with silver diamine fluoride therapy. J Dent. 2014; 42:395-402
Stebbins EA. What value has argenti nitras as a therapeutic agent in dentistry?. Int Dent J. 1891; 12:661-670
Howe PR. A method of sterilizing and at the same time impregnating with a metal affected dentinal tissue. Dent Cosmos. 1917; 59:891-904
Duffin S. Back to the future: the medical management of caries introduction. J Calif Dent Assoc. 2012; 40:852-858
Suzuki T, Nishida M, Sobue S, Moriwaki Y. Effects of diammine silver fluoride on tooth enamel. J Osaka Univ Dent Sch. 1974; 14:61-72
Patel J, Anthonappa RP, King NM. Evaluation of the staining potential of silver diamine fluoride: in vitro. Int J Paediatr Dent. 2018; https://doi.org/10.1111/ipd.12401
Chu CH, Lo ECM. Promoting caries arrest in children with silver diamine fluoride: a review. Oral Health Prev Dent. 2008; 6:315-321
Mei ML, Ito L, Cao Y, Li QL, Lo EC, Chu CH. Inhibitory effect of silver diamine fluoride on dentine demineralisation and collagen degradation. J Dent. 2013; 41:809-817
Zhao IS, Gao SS, Hiraishi N, Burrow MF, Duangthip D, Mei ML Mechanisms of silver diamine fluoride on arresting caries: a literature review. Int Dent J. 2018; 68:67-76
Lou YL, Botelho MG, Darvell BW. Reaction of silver diamine fluoride with hydroxyapatite and protein. J Dent. 2011; 39:612-618
Mei ML, Li QL, Chu CH, Lo ECM, Samaranayake LP. Antibacterial effects of silver diamine fluoride on multi-species cariogenic biofilm on caries. Ann Clin Microbiol Antimicrob. 2013; 12
Chu CH, Mei L, Seneviratne CJ, Lo EC. Effects of silver diamine fluoride on dentine carious lesions induced by Streptococcus mutans and Actinomyces naeslundii biofilms. Int J Paediatr Dent. 2012; 22:2-10
Mei ML, Nudelman F, Marzec B, Walker JM, Lo ECM, Walls AW, Chu CH. Formation of Fluorohydroxyapatite with Silver Diamine Fluoride. J Dent Res. 2017; 96:1122-1128
Frencken JE, Pilot T, Songpaisan Y, Phantumvanit P. Atraumatic Restorative Treatment (ART): rationale, technique, and development. J Public Health Dent. 1996; 56:135-140
Gao SS, Zhao IS, Hiraishi N, Duangthip D, Mei ML, Lo ECM Clinical trials of Silver Diamine Fluoride in arresting caries among children: a systematic review. JDR Clin Trans Res. 2016; 1:201-210
Chibinski AC, Wambier LM, Feltrin J, Loguercio AD, Wambier DS, Reis A. Silver Diamine Fluoride has efficacy in controlling caries progression in primary teeth: a systematic review and meta-analysis. Caries Res. 2017; 51:527-541
Mei ML, Zhao IS, Ito L, Lo EC, Chu CH. Prevention of secondary caries by silver diamine fluoride. Int Dent J. 2016; 66:71-77
Zhao IS, Mei ML, Burrow MF, Lo EC-M, Chu C-H. Effect of Silver Diamine Fluoride and Potassium Iodide treatment on secondary caries prevention and tooth discolouration in cervical glass ionomer cement restoration. Int J Mol Sci. 2017; 18
Chu CH, Lo EC, Lin HC. Effectiveness of silver diamine fluoride and sodium fluoride varnish in arresting dentin caries in Chinese pre-school children. J Dent Res. 2002; 81:767-770
Weerheijm KL, Groen HJ. The residual caries dilemma. Community Dent Oral Epidemiol. 1999; 27:436-441
Yee R, Holmgren C, Mulder J, Lama D, Walker D, van Palenstein Helderman W. Efficacy of silver diamine fluoride for arresting caries treatment. J Dent Res. 2009; 88:644-647
Fung MHT, Duangthip D, Wong MCM, Lo ECM, Chu CH. Arresting dentine caries with different concentration and periodicity of Silver Diamine Fluoride. JDR Clin Trans Res. 2016; 1:143-152
Chairside Guide: Silver Diamine Fluoride in the management of dental caries lesions. Pediatr Dent. 2017; 39:478-479
Horst JA, Ellenikiotis H UCSF protocol for caries arrest using Silver Diamine Fluoride: rationale, indications, and consent. J Calif Dent Assoc. 2016; 44:16-28
Zhi QH, Lo EC, Lin HC. Randomized clinical trial on effectiveness of silver diamine fluoride and glass ionomer in arresting dentine caries in preschool children. J Dent. 2012; 40:962-967
Duangthip D, Chu CH, Lo EC. A randomized clinical trial on arresting dentine caries in preschool children by topical fluorides – 18 month results. J Dent. 2016; 44:57-63
Duangthip D, Wong MCM, Chu CH, Lo ECM. Caries arrest by topical fluorides in preschool children: 30-month results. J Dent. 2018; 70:74-79
Wang AS, Botelho MG, Tsoi JKH, Matinlinna JP. Effects of silver diammine fluoride on microtensile bond strength of GIC to dentine. Int J Adhes Adhes. 2016; 70:196-203
Quock RL, Barros JA, Yang SW, Patel SA. Effect of silver diamine fluoride on microtensile bond strength to dentin. Oper Dent. 2012; 37:610-616
Wu DI, Velamakanni S, Denisson J, Yaman P, Boynton JR, Papagerakis P. Effect of Silver Diamine Fluoride (SDF) application on microtensile bonding strength of dentin in primary teeth. Pediatr Dent. 2016; 38:148-153
Mei ML, Zhao IS, Ito L, Lo ECM, Chu CH. Prevention of secondary caries by silver diamine fluoride. Int Dent J. 2016; 66:71-77
Zhao IS, Mei ML, Burrow MF, Lo EC-M, Chu C-H. Prevention of secondary caries using silver diamine fluoride treatment and casein phosphopeptide-amorphous calcium phosphate modified glass-ionomer cement. J Dent. 2017; 57:38-44
Korwar A, Sharma S, Logani A, Shah N. Pulp response to high fluoride releasing glass ionomer, silver diamine fluoride, and calcium hydroxide used for indirect pulp treatment: an in-vivo comparative study. Contemp Clin Dent. 2015; 6:288-292
Alvear Fa, Jew JA, Wong A, Young D. Silver Modified Atraumatic Restorative Technique (SMART): an alternative caries prevention tool. Stoma Edu J. 2016; 3:243-249
Dos Santos VE, de Vasconcelos FM, Ribeiro AG, Rosenblatt A. Paradigm shift in the effective treatment of caries in schoolchildren at risk. Int Dent J. 2012; 62:47-51
Duangthip D, Fung M HT, Wong M, Chu CH, Lo ECM. Adverse effects of Silver Diamine Fluoride treatment among preschool children. J Dent Res. 2017; 97:395-401
Llodra JC, Rodriguez A, Ferrer B, Menardia V, Ramos T, Morato M. Efficacy of silver diamine fluoride for caries reduction in primary teeth and first permanent molars of schoolchildren: 36-month clinical trial. J Dent Res. 2005; 84:721-724
Mei ML, Chu CH, Lo ECM, Samaranayake LP. Fluoride and silver concentrations of silver diammine fluoride solutions for dental use. Int J Paediatr Dent. 2013; 23:279-285
Vasquez E, Zegarra G, Chirinos E, Castillo JL, Taves DR, Watson GE Short term serum pharmacokinetics of diammine silver fluoride after oral application. BMC Oral Health. 2012; 12
Browne D, Whelton H, O'Mullane D. Fluoride metabolism and fluorosis. J Dent. 2005; 33:177-186
Silver Diamine Fluoride: a critical review and treatment recommendations Jilen Patel Robert P Anthonappa Nigel M King Dental Update 2024 46:7, 707-709.
Professor in Paediatric Dentistry, Faculty of Dentistry, The University of Hong Kong, 2/F, Prince Philip Dental Hospital, 34 Hospital Road, Hong Kong, P R China
Over the last decade there has been a renewed interest in the use of Silver Diamine Fluoride (SDF) as an adjunctive modality in the management of caries among high-risk populations. This review presents the current evidence behind the use of SDF and recommendations for its use in caries management dental practice.
CPD/Clinical Relevance: Silver diamine fluoride is an effective, evidence-based modality that can contribute towards arresting carious lesions among high-risk children and disadvantaged populations.
Article
Dental caries remains a global public health issue affecting over 621 million children worldwide.1 For high-risk groups who continue to experience high burdens of dental caries, the traditional restorative approach to caries management is neither readily available, accessible nor affordable, and has shown limited success in controlling the carious process on a population level.2 Non-restorative techniques aimed at managing the caries biofilm and supporting remineralization are therefore becoming more common.3,4
Over the last decade there has been a renewed interest in the use of silver diamine fluoride (SDF) as an adjunctive modality in the management of dental caries among high-risk groups. SDF is deemed to be a safe, effective, efficient and equitable caries control agent that can be used to help meet the WHO Millennium oral health goals and fulfil the USA Institute of Medicine's criteria for 21st Century medical care.5,6
This review discusses the current evidence and guidelines on the use of SDF in caries management.
History
As long ago as 1891, a mixture of nitric acid and amalgam scraps was used to inhibit caries progression.7 This silver nitrate solution was popularized by Howe who used it to arrest caries among disadvantaged children in Boston, USA, leading to the solution being termed ‘Howe's solution’.8 Silver nitrate was advocated by leaders in the dental profession such as WD Miller, GV Black and Percy Howe; hence the solution was widely used in the USA up until the 1960s. The use of silver nitrate declined in popularity after this time, probably due to the advent of fluoride varnishes, increased access to surgical care and improved restorative techniques. Duffin proposed the use of 25% silver nitrate (AgNO3) solution followed by 5% sodium fluoride (NaF) varnish to arrest carious lesions in dentine.9 Although this protocol has shown some promise in the laboratory setting, further research is required to establish the clinical efficacy and safety of this mixture.
During the 1960s and 1970s, SDF was further developed and studied in Japan.10 SDF use was supported by Japan's Ministry of Health and Welfare and has been in use for the last 40 years. Advances in the formulation and preparation of silver fluoride solutions internationally have led to a number of commercially available forms of SDF (Table 1). Currently in the UK, Riva Star™ (SDI, Bayswater, Victoria) is the only available preparation and uses a formulation of 38% SDF with potassium iodide (KI) as a separately applied reagent. The application of KI following SDF has been advocated to reduce the degree of black staining, which is the main clinical disadvantage of using SDF alone.11 Notably, preparations such as Riva Star™ are registered only as desensitizing agents; thus, the use of such preparations for caries prevention or caries arrest is considered to be off-label.
Product Name
SDF Concentration
Country
Cariostatic
10%
Brazil
Cariestop
12%
Brazil
Cariestop
38%
Brazil
Bioride
30%
Brazil
Saforide
38%
Japan
Advantage Arrest
38%
USA
Fluoroplat V
38%
Argentina
Riva Star™
38%
United Kingdom
Terminology
There are a number of terms used in the literature to describe SDF and the variations (Table 2). The term SDF is often colloquially used interchangeably with silver fluoride (AgF), however, these are two distinctly different compounds. The bound ammonia in SDF confers different chemical properties on the compound, making it significantly more stable than AgF, which enhances the shelf-life characteristic by maintaining a constant concentration for a longer period.12
Ammoniated silver fluoride
Ammoniacal silver fluoride
Diamine silver fluoride
Silver diamine fluoride (most commonly used spelling in the literature)
Silver diammine fluoride (most chemically correct description referring to the complex between ammonia molecules and a metal ion)
Diammine silver fluoride
How does it work?
The exact mechanism of action of SDF, whether it is chemical, physical, mechanical or antibacterial, remains unclear. However, it has been proposed that SDF interacts with the structure of both enamel and dentine, as well as having an antibacterial action on the organisms in oral biofilms. Studies have shown that SDF has the ability to preserve collagen from degradation in demineralized dentine while inhibiting collagenases such as matrix metalloproteinases and cysteine cathepsins.13,14 SDF produces a highly remineralized zone that is rich in calcium and phosphate in cavitated dentinal lesions of primary teeth that in turn protects collagen from being exposed to the oral environment.6,15 Furthermore, SDF inhibits multi-species cariogenic biofilm formation on dentine carious lesions.16,17 In addition, SDF reacts with calcium and phosphate ions to produce fluorhydroxyapatite, thereby inhibiting demineralization.18
Justification for SDF use
The challenge to provide oral healthcare for vulnerable populations with limited access to care led to the development of non-restorative caries treatments and the ‘atraumatic restorative technique’ (ART).4,19 The use of SDF can be considered a non-restorative approach to caries management and may be used in cases where conventional treatment is impossible, such as for children who are pre-cooperative or are medically compromised. With respect to non-restorative caries treatment, SDF offers more time for improving and stabilizing caries-affected dentition. In the interim, heightened preventive regimes focused on dietary and oral hygiene practices can be implemented. Definitive restorative treatment can then be planned following successful caries stabilization.
How effective is SDF in arresting caries?
A meta-analysis of eight randomized control trials (RCTs) using 38% SDF found that the caries arresting rate of SDF treatment was 86% (95% confidence interval (CI), 47% to 98%; P = 0.06) at 6 months, 81% (95% CI, 59% to 93%; P = 0.01) at 12 months, 78% (95% CI, 70% to 85%; P < 0.001) at 18 months, 65% (95% CI, 35% to 86%; P = 0.32) at 24 months, and 71% (95% CI, 56% to 83%; P = 0.01) at or beyond 30 months. The overall proportion of arrested dental caries after SDF treatment was 81% (95% CI, 68% to 89%; P < 0.001).20 Recently, a meta-analysis by Chibinski and co-workers reported that the available evidence was of a high quality and concluded that SDF was 89% more effective in controlling or arresting caries than other treatments or placebos.21In vitro studies have suggested that treatment with SDF can increase resistance of cavity margins around GIC restorations to secondary caries development.22,23
Does caries need to be removed prior to SDF application?
In a RCT involving 375 children with a follow-up period of 24 months, Chu and colleagues24 compared 38% SDF to 5% NaF and further divided the groups into ‘with’ or ‘without’ caries excavation (n = 70 approximately per group). The findings demonstrated that removal of carious tissue prior to the application of the fluoride agents did not enhance the ability to arrest dentine caries.24 This is in contrast to the belief that ‘one has to strive for as near as complete caries removal as possible’ prior to fluoride treatment because the bacterial load in the carious lesion is reduced.25
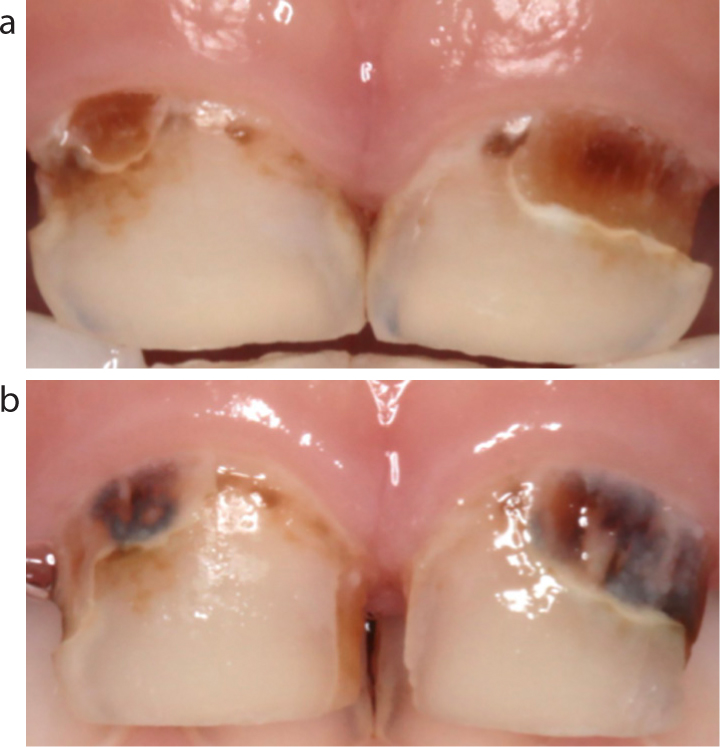
Figure 1.
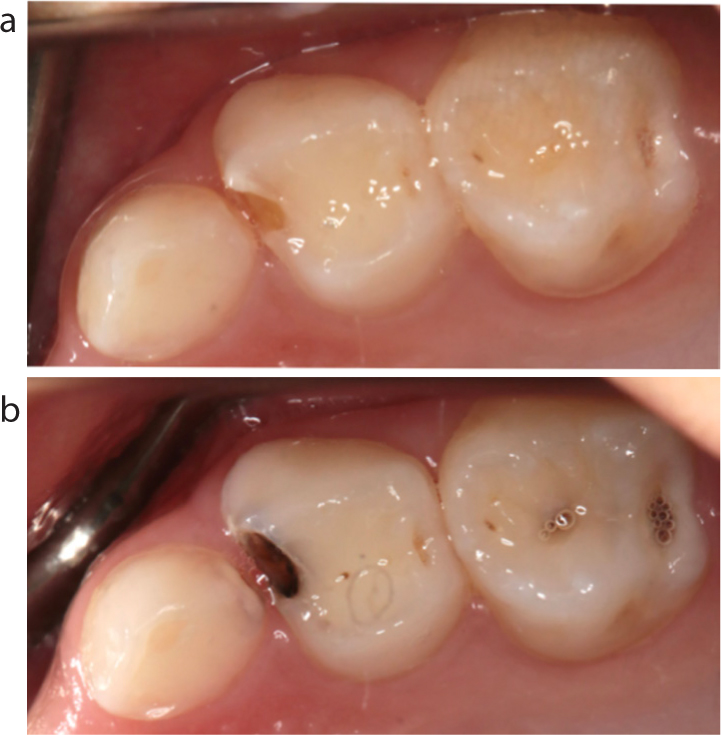
(a) Carious lesions on anterior teeth at baseline prior to application of 38% SDF. (b) Six months post-application of SDF.Figure 2.
(a) Carious lesions on posterior teeth at baseline prior to application of 38% SDF. (b) Six months post-application of SDF.
What concentration of SDF is most effective?
The different commercially available preparations of SDF are presented in Table 1, with the most commonly available concentration being a 38% solution. In a RCT involving 976 Nepalese schoolchildren followed-up at 6 months, Yee and co-workers found that a one off application of 12% SDF solution was ineffective for arresting carious lesions in primary teeth, while the use of 38% SDF was found to be effective.26 This finding was supported by a recent RCT with a 30 month follow-up in which the 38% SDF was clearly more effective than 12% SDF.27
What are the criteria for SDF use?
SDF is indicated as an adjunctive modality for treating caries among high-risk patients who are unable to access dental treatment or tolerate conventional dental care. This includes young or ‘pre-cooperative’ children, medically or physically compromised patients and those that may be unable to access routine comprehensive care due to barriers such as geographic isolation.
Teeth with evidence of pulpitis or pulp necrosis are not appropriate for SDF treatment and require surgical treatment. Similarly, teeth with deep dentine lesions encroaching on the pulp are not suitable for SDF treatment due to the ammonia content and high pH, which may trigger pulpal inflammation. Other contra-indications to use include patients with a silver allergy and parents or patients who object to potential staining.
How is SDF applied?
Prior to SDF application it is imperative that (i) both the patient and practitioner have standard personal protective equipment, and (ii) appropriate diagnosis of the carious lesion and the pulp status has been made to ensure that the lesion is suitable for treatment using SDF. The recommended procedure for SDF application is as follows:28
Gross debris from the cavity can be removed to allow better contact of SDF with denatured dentine. However, carious dentine excavation prior to SDF application is not necessary.
Isolate the carious lesion from the adjacent soft tissues using cotton wool rolls, use a saliva ejector to remove excess saliva from the site of application. Note: petroleum jelly can be used as a gingival barrier, if required.
Dispense no more than a drop of SDF into a dappen dish. One drop (25 μL) is ample to treat 5 teeth, and contains 9.5 mg SDF. The University of California, San Francisco (UCSF) protocol recommends a limit of 1 drop (25 μL) per 10 kg per treatment visit, with weekly intervals at most.29
Dip the microbrush into SDF and dab on the side of the dappen dish to remove excess solution.
Apply SDF directly to the affected tooth surface only. Application time should be at least one minute, if possible. However, application time may be shorter in very young and difficult to manage patients. In these cases, the patient should be regularly reviewed and consideration made for re-application. Re-application of SDF may be indicated if the treated carious lesions do not appear arrested (dark and hard) 2 to 4 weeks post-application.
After application, blot the carious lesion with gauze, cotton roll, or cotton pellet to minimize systemic absorption.
After treating specific carious lesions with the SDF, the entire dentition can be coated with a thin layer of 5% NaF varnish for primary prevention, if appropriate.
How often should SDF be applied?
The commonly adopted frequency of SDF application is either 6-monthly or 12-monthly. However, the optimal protocol for SDF application still requires further research before a definitive protocol is established. Nevertheless, Zhi and co-workers suggest that 6-monthly applications increase the caries arrest rate compared to 12-monthly application protocol.30 This recommendation is supported by the findings of the RCT conducted by Fung and co-workers who found that carious lesions treated with SDF on a biannual basis had a higher chance of becoming arrested compared to those receiving annual applications of SDF (odds ratio, 1.33; 95% CI, 1.04–1.71; P = 0.025).27 However, fundamental preventive protocols, such as twice-daily toothbrushing using fluoridated toothpaste along with a balanced diet, should always maintain priority. As such, SDF should never be used or thought of as an alternative to proper oral health care.
How does SDF compare with traditional NaF varnish?
NaF has long been considered the best preventive therapeutic agent to arrest carious lesions in enamel. However, the results of some clinical trials suggest that 38% SDF was found to be more effective in arresting caries in primary teeth among children when compared with 5% NaF varnish.24,31 The results of a recent RCT involving 309 children with a 30 month follow-up period found that the annual applications of SDF solution were more effective in arresting dentine caries in primary teeth than three consecutive weekly applications of NaF varnish.32
Can SDF be used prior to placing a restoration?
SDF can be used in a two-stage approach to (i) stabilize and arrest caries initially, and (ii) place a conventional restoration at a later time. To date, the majority of studies indicate that SDF application does not adversely affect dentinal bond strength to resin composite or glass ionomer cement (GIC).33-34,35 Furthermore, in vitro studies suggest that conditioning with SDF prior to placement of GIC or resin composite restorations may increase resistance to secondary caries,36,37 while SDF has also been shown to have good capability to induce tertiary dentine deposition.38
SDF can also be used in conjunction with ART, a concept that has been referred to as the Silver Modified Atraumatic Restorative Technique (SMART).39 This technique involves application of SDF followed by placement of a GIC restoration. However, further studies are required to demonstrate the success of this technique.
When investigating the caries arrest potential of SDF with GIC, Dos Santos and co-workers40 compared the application of 30% SDF with an interim restorative treatment (IRT) using GIC (Fuji IX) in primary teeth over 12 months. The results indicated that, after 12 months, the caries arresting rate of SDF application alone was 67% compared with 39% for GIC. The authors suggested that this could be a paradigm shift in the treatment of carious lesions in high-risk children.40
Is SDF safe to use?
To date, several RCTs have been conducted on the use of SDF and these have found no serious adverse events following the application.41 Nevertheless, the main concerns around SDF use are:
The development of black staining post-application;
Transient gingival irritation; and
High fluoride concentrations and potential toxicity.
Black staining following SDF application to the tooth occurs as a soluble silver phosphate layer is formed after the application of SDF on carious dentine. This layer appears yellow initially, then turns dark brown or black under the influence of a reducing agent or under sunlight. Silver sulphide precipitates can also be formed which contributes to the discoloration of the tooth.31
Llodra and co-workers42 reported three cases (n = 675) where contact of SDF with the oral mucosa caused small white lesions that were mildly painful but disappeared within 48 hours without any treatment.42 Recently, a systematic review concluded that the reports on oral pain, gingival swelling and bleaching are uncommon and probably not related to the application of SDF.41 However, the mechanism of this phenomenon is unclear.
Concerns around the potential toxicity of SDF have been raised, given the high concentration of fluoride in SDF, reported to be around 44,800ppm.43 However, only a minute volume of SDF is actually applied to a carious lesion and it has been suggested that the average amount of fluoride following SDF application per patient ranges from approximately 0.17 mg to 0.36 mg, which is well below the No Observed Adverse Effect Limit (NOAEL).44
The NOAEL is defined as the highest dose of a chemical in a single study, found by experiment or observation, which causes no detectable adverse health effect.45 The NOAEL reported for fluorosis is 0.05 mgF/kg/body weight.45 As the most commonly adopted frequency of SDF application is annually or biannually, and the SDF application is restricted to carious lesions, the total amount is far below the NOAEL dose.
Conclusions
The use of SDF in paediatric dentistry may be a paradigm shift towards a more medical model of caries management, leading to an effective, affordable and sustainable solution for high-risk children around the world.
SDF has been used for over 40 years in dentistry; however, its use in the western world has increased and gained significant interest in the last decade. SDF is inexpensive, painless, and it is easy to apply. It has been shown to be more effective for arresting caries in the primary dentition than 5% NaF varnish or GIC restorations placed using the ART technique. The silver component acts as an antimicrobial agent, the fluoride promotes remineralization, and the ammonia stabilizes high concentrations in solution. The available literature supports the biannual use of 38% SDF and the available studies suggest a caries arrest rate of 80% after 24 months. Although SDF has the potential to arrest caries among high-risk groups, it should never be used or thought of as an alternative to proper oral healthcare and therefore implementation of fundamental preventive protocols, such as twice-daily toothbrushing using fluoridated toothpaste, a balanced diet and access to comprehensive care, should always remain a priority.