Liou EJ, Pai BC, Lin JC. Do miniscrews remain stationary under orthodontic forces?. Am J Orthod Dentofacial Orthop. 2004; 126:42-47
Mizrahi E, Mizrahi B. Mini-screw implants (temporary anchorage devices): orthodontic and pre-prosthetic applications. J Orthod. 2007; 34:(2)80-94
Wahl N. Orthodontics in the 3 millenia. Chaper 15: Skeletal anchorage. Am J Orthod Dentofacial Orthop. 2008; 134:707-710
Hong H, Ngan P, Han G. Use of onplants as stable anchorage for facemask treatment: a case report. Angle Orthod. 2005; 75:(3)
Gainsforth BL, Higley LB. A study of orthodontic anchorage possibilities of basal bone. Am J Orthod Dentofacial Orthop. 1945; 31:(8)406-417
Creekmore TD, Eklund MK. The possibility of skeletal anchorage. J Orthod. 1983; 17:(4)266-269
Melsen B, Petersen JK, Costa A. Zygoma ligatures: an alternative form of maxillary anchorage. J Clin Orthod. 1998; 32:(3)154-158
Kanomi R. Mini-implant for orthodontic anchorage. J Clin Orthod. 1997; 31:(11)763-767
Roberts WE, Marshall KJ, Mozsary PG. Rigid endosseous implant utilized as anchorage to protract molars and close an atrophic extraction site. Angle Orthod. 1990; 60:(2)135-151
Triaca A, Antonini M, Wintermantel E. Ein neues Titan-Flachschrauben-Implantat zur orthodontischen verankerung an anterioren Gaumen. Inform Orthod Kieferorthop. 1992; 24:251-257
Costa A, Raffaini M, Melsen B. Microscrews as orthodontic anchorage: a preliminary report. Int J Adult Orthod Orthognathic Surg. 1998; 13:201-209
Young KA, Melrose CA, Harrison JEH. Skeletal anchorage systems in orthodontics: absolute anchorage. A dream or reality?. J Orthod. 2007; 34:(2)101-110
Baumgaertel S, Razavi MR, Hans MGM. Mini-implant anchorage for the Orthodontic Practitioner. Am J Orthod Dentofacial Orthop. 2008; 133:(4)621-627
Cacciafesta V. JCO Roundtable: Skeletal anchorage Part 1. Panelists discuss common applications of miniscrews. J Clin Orthod. 2009; 43:(5)
Sherwood KH, Burch JG, Thompson WJ. Closing anterior open bites by intruding molars with titanium miniplate anchorage. Am J Orthod Dentofacial Orthop. 2002; 122:593-600
Reynders R, Ronchi L, Bipat S. Mini-implants in orthodontics: a systematic review of the literature. Am J Orthod Dentofacial Orthop. 2009; 135
Park HS, Kwon TG, Kwon OW. Treatment of open bite with microscrew implants anchorage. Am J Orthod Dentofacial Orthop. 2004; 126:(5)627-636
Kuroda S, Katayama A, Takano-Yamamoto T. Severe anterior open bite case treated using titanium screw anchorage. Angle Orthod. 2004; 74:(4)
Rachala MR, Harikrishnan P. Management of severe anterior open bite in an adult patient using miniscrews as skeletal anchorage. Int J Orthod. 2010; 21:(1)9-14
Kuroda S, Sakai Y, Tamamura N Treatment of severe anterior open bite with skeletal anchorage in adults: comparison with orthognathic surgery outcomes. Am J Orthod Dentofacial Orthop. 2007; 132:(5)
Vibhute PJ. Molar-stabilising power arm and miniscrew anchorage for anterior retraction. J Clin Orthod. 2010; 44:(11)
Breuning KH. Correction of a Class III malocclusion with over 20 mm of space to close in the maxilla by using miniscrews for extra anchorage. Am J Orthod Dentofacial Orthop. 2008; 133:(3)459-469
Jamilian A, Showkatbakhsh R. Treatment of maxillary defiency by miniscrew implants. J Orthod. 2010; 37:(2)
Kook YA, Kim SH. Treatment of Class III relapse due to late mandibular growth using miniscrew anchorage. J Clin Orthod. 2008; 42:(7)
Park HS, Kwon TG. Sliding mechanics with miniscrew implant anchorage. Angle Orthod. 2004; 74:(5)
Upadhyay M, Yadav S, Nagarai K. Treatment effects of mini-implants for en-masse retraction of anterior teeth in bialveolar dental protrusion patients: a randomised controlled trial. Am J Orthod Dentofacial Orthop. 2008; 134:18-29
Jung MH. Biomechanical considerations in treatment with miniscrew anchorage. J Clin Orthod. 2008; 42:(6)329-337
Park YC, Choi YJ, Choi NC Aesthetic segmental retraction of maxillary anterior teeth with a palatal appliance and orthodontic mini-implants. Am J Orthod Dentofacial Orthop. 2007; 131:(4)
Park HS, Lee SK, Kwon OH. Group distal movement of teeth using microscrew implant anchorage. Angle Orthod. 2005; 75:602-609
Herman RJ, Currier GF, Miyake A. Mini-implant anchorage for maxillary canine retraction: a pilot study. Am J Orthod Dentofacial Orthop. 2006; 130:228-235
Papadopoulis MA. Orthodontic treatment of Class II malocclusion with miniscrew implants. Am J Orthod Dentofacial Orthop. 2008; 134:(5)
Munoz A, Maino G, Lemler J. Skeletal anchorage for Class II correction in a growing patient. J Clin Orthod. 2009; 43:(5)325-331
Lee JS, Park HS, Kyung HM. Micro-implant anchorage for lingual treatment of a skeletal class II malocclusion. J Clin Orthod. 2001; 35
Yao CC, Wu CB, Wu HY Intrusion of the overerupted upper first left first and second molars by mini implants with partial fixed orthodontic appliances: a case report. Angle Orthod. 2004; 74:550-557
Bonetti GA, Verganti S, Zanarini M Orthodontic intrusion of posterior teeth using dental implant anchorage. J Clin Orthod. 2008; 42:(4)222-225
Choi KJ, Choi JH, Lee SY Facial improvements after molar intrusion with miniscrew anchorage. J Clin Orthod. 2007; 41:(5)273-280
Graham JW. Temporary replacement of maxillary lateral incisors with miniscrews and bonded pontics. J Clin Orthod. 2007; 41:(6)321-325
Weisner SM. Treatment of a skeletal class III malocclusion with mandibular asymmetry using a single miniscrew. J Clin Orthod. 2009; 43:(5)335-341
Kinzinger GS, Gulden N, Yildizhan F Efficiency of a skeletonised distal jet appliance supported by miniscrew anchorage for noncompliance maxillary molar distalisation. Am J Orthod Dentofacial Orthop. 2009; 136:(4)578-586
Buschang P, Carrillo R. 2008 Survey of AAO members on miniscrew usage. J Orthod. 2008; 42:(9)
Moon C, Lee D, Lee H Factors associated with the success rate of orthodontic miniscrews placed in the upper and lower posterior buccal region. Angle Orthod. 2008; 78:(1)
Janssen V. Skeletal anchorage in Orthodontics – a review of various systems in animal and human studies. Int J Oral Maxillofac Implants. 2008; 23:75-88
Cheng SJ, Tseng IY, Lee JJ. A prospective study of the risk factors associated with failure of mini-implants used for orthodontic anchorage. Int J Oral Maxillo Impl. 2004; 19:(1)
Kim YH, Yang SM, Kim S Midpalatal miniscrews for orthodontic anchorage: factors affecting clinical success. Am J Orthod Dentofacial Orthop. 2010; 137:66-72
Kuroda S, Sugawara Y, Deguchi T Clinical use of miniscrew implants as orthodontic anchorage: success rates and postoperative discomfort. Am J Orthod Dentofacial Orthop. 2007; 131:9-15
Asscherickx K, Vannet BV, Bottenberg P Clinical observations and success rates of palatal implants. Am J Orthod Dentofacial Orthop. 2010; 137:114-122
Park HS, Jeong SH, Kwon OH. Factors affecting the clinical success of screw implants used as orthodontic anchorage. Am J Orthod Dentofacial Orthop. 2006; 130:18-25
Thiruvenkatachari AK. Comparison of rate of canine retraction with conventional molar anchorage and titanium implant anchorage. Am J Orthod Dentofacial Orthop. 2008; 134:30-35
Reinforcement of anchorage during orthodontic brace treatment with implants or other surgical methods (review). 2009. http://www.thecochranelibrary.com
Yao CC, Lai EHH, Chang JZC Comparison of treatment outcomes between skeletal anchorage and extraoral anchorage in adults with maxillary dentoalveolar protrusion. Am J Orthod Dentofacial Orthop. 2008; 134:(5)
Deguchi T, Murakami T, Kuroda S Comparison of the intrusion effects on the maxillary incisors between implant anchorage and J-hook headgear. Am J Orthod Dentofacial Orthop. 2008; 133:654-660
Benson PE, Tinsley D, O'Dwyer J Midpalatal implants vs headgear for orthodontic anchorage – a randomised clinical trial: cephalometric results. Am J Orthod Dentofacial Orthop. 2007; 132:606-615
Crismani B. Miniscrews in orthodontic treatment: review and analysis of published clinical trials. Am J Orthod Dentofacial Orthop. 2010; 137:108-113
Miyawaki S, Koyama I, Inoue M Factors associated with the stability of titanium screws placed in the posterior region for orthodontic anchorage. Am J Orthod Dentofacial Orthop. 2003; 124:373-378
Tsaousidis G, Bauss O. Influence of insertion site on the failure rates of orthodontic miniscrews. J Orofac Orthop. 2008; 69:(5)349-356
Chen KZ. Critical factors for the success of orthodontic mini-implants: a systematic review. Am J Orthod Dentofacial Orthop. 2009; 135:284-291
Luzi C, Verna C, Melsen B. A prospective clinical investigation of the failure rate of immediately loaded mini-implants used for orthodontic anchorage. Prog Orthod. 2007; 8:(1)192-201
Bayat B. Effect of smoking on the failure rates of orthodontic miniscrews. J Orofacial Orthop. 2010; 71:117-124
Garfinkle JS, Cunningham JR, Beeman CS Evaluation of orthodontic mini implant anchorage in premolar extraction therapy in adolescents. Am J Orthod Dentofacial Orthop. 2008; 133:(5)642-653
Gelgor I, Buyukyilmaz T, Karaman AI Intraosseous screw supported upper molar distalisation. Angle Orthod. 2004; 74:838-850
Chen C, Chang C, Hsieh CH The use of microimplants in orthodontic anchorage. J Oral Maxillofac Surg. 2006; 64:1209-1213
Lee K, Kim K, Lee J Computed tomographic analysis of tooth-bearing alveolar bone for orthodontic miniscrew placement. Am J Orthod Dentofacial Orthop. 2009; 135:486-494
Pickard M, Dechow P, Rossouw P Effects of miniscrew orientation on implant stability and resistance to failure. Am J Orthod Dentofacial Orthop. 2010; 137:91-99
Viwattanatipa N, Thanakitcharu S, Uttraravichien A Survival analyses of surgical miniscrews as orthodontic anchorage. Am J Orthod Dentofacial Orthop. 2009; 136:29-36
Kadioglu O, Buyukyilmaz T, Zachrisson BU Contact damage to root surfaces of premolars touching miniscrews during orthodontic treatment. Am J Orthod Dentofacial Orthop. 2008; 134:353-360
Maino G, Weiland F, Attanasi A Root damage and repair after contact with miniscrews. J Clin Orthod. 2007; 41:(12)
Poggio PM, Incorvati C, Velo S “Safe zones”. A guide for miniscrew positioning in the maxillary and mandibular arch. Angle Orthod. 2006; 76
Oliver R, Knapman YM. Attitudes to orthodontic treatment. Br J Orthod. 1985; 12:(4)
Cornelis MA, Scheffler NR, Nyssen-Behets C. Patients' and orthodontists' perceptions of miniplates used for temporary skeletal anchorage: a prospective study. Am J Orthod Dentofacial Orthod. 2008; 133:(1)18-24
Lee TC, McGrath CP, Wong RW Patients' perceptions regarding microimplant as anchorage. Angle Orthod. 2008; 78:(2)
Baxmann M Expectations, acceptance and preferences regarding microimplant treatment in orthodontic patients: a randomised controlled trial. Am J Orthod Dentofacial Orthop. 2010; 138:250.e1-250.e10
This is a literature search about the clinical use of temporary anchorage devices (TADs) as a means of providing effective orthodontic anchorage. It takes the reader through a journey from the initial description of the technique to the enormous popularity TADs are currently experiencing in clinical practice. This paper aims to present good quality clinical information to allow the clinician and the patient to make an informed decision.
Clinical Relevance: The purpose of this literature review is to provide readers with an overview of the current available literature on this subject and encourage general dental practitioners to adopt a more evidence-based approach to this aspect of orthodontic care.
Article
Anchorage in orthodontics can be defined as the resistance to unwanted tooth movement during treatment. This can be provided by intra-oral anchor sites like the teeth and palate or, alternatively, extra-oral devices such as headgear (Figure 1). Unfortunately, these conventional methods have a major drawback: they all rely on patient compliance in order to be successful.1 It has been every orthodontist's dream to have stationary anchorage. Recent literature has suggested that the introduction of miniscrews or temporary anchorage devices (TADs), a term of American origin,2 has created a whole new successful era in the world of orthodontics.
Figure 1. Headgear is a traditional ‘tried and tested’ way of providing anchorage.
Terminology
Successful skeletal anchorage is the main biological concept behind these devices and this offers two possibilities:
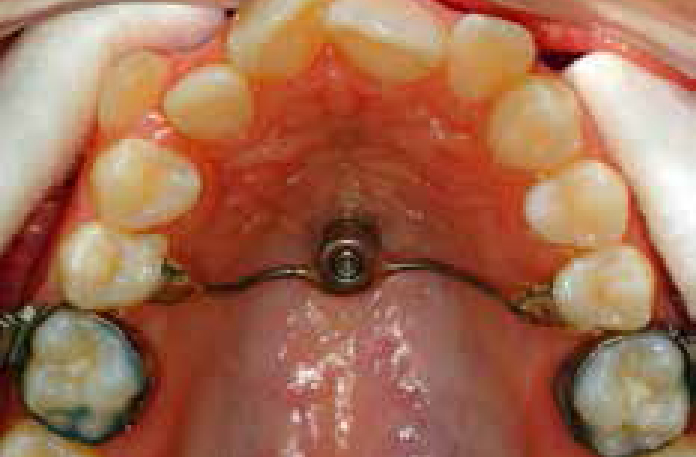
Indirect anchorage: use of such devices means provision of immovable connections to the teeth, which serve as the actual anchorage units (Figure 2); or alternatively
Direct anchorage: which means utilization of direct forces originating from the actual device itself, in this case the screws inserted into the bone (Figure 3).
Figure 2. Palatal implant connected to premolar teeth offers indirect anchorage for canine retraction.Figure 3. Canine being retracted directly onto the temporary anchorage device.
Osseo-integrated dental implants, including palatal implants and some retromolar implants, often fall into the category of indirect anchorage. One commonly used mid-palatal implant from Straumann has a diameter of 3.75 mm and length of 8 mm, whereas normal ‘dental’ implants, replacing individual teeth, can vary in length from 7–20 mm. These osseo-integrated implants have been used for direct anchorage in the past prior to them being used to replace the dentition.
Intra-oral implants developed further categories, including miniplates, which are attached to cortical bone by miniscrews. They are commonly inserted into the mandibular buccal bone or maxillary zygomatic buttress3 and allow indirect anchorage or direct anchorage, depending upon their position (Figure 4). Osseo-integration is not a desirable feature in this particular category, as it would complicate their removal, nor has it been found to be necessary to provide adequate anchorage.
Figure 4. Miniplates being used as anchors to allow tooth distalization.
Onplants are another completely different category from implants as these are placed sub-periosteally and are meant to integrate between their inferior surface and the outer surface of cortical bone. These are manufactured as flat, titanium discs, sometimes with hydroxyapatite-coated surfaces to encourage bone integration. Onplants have been reported to withstand orthodontic forces of up to 311 g,4 however, rapidly fell out of use as the early results were not particularly encouraging.
Method of literature search
Medline, PubMed and Cochrane Clinical Trials Register (CCTR) searches were conducted using the following keyword search:
Orthodontic miniscrews OR mini-implants;
Success of miniscrews OR mini-implants;
Temporary anchorage devices.
A total of 105 papers were found and manually sifted to exclude any that involved in vitro or animal studies. The final batch of 72 papers included in this search was divided into the following groups:
Clinical trials;
Case reports;
Comparison reports between TADs and other anchorage devices;
Relevant papers about history, surveys and types of miniscrews;
One paper about ongoing national audit processes has also been included.
History of implants
The first reported attempt to use intra-oral anchorage with metal screws was carried out on dogs, by Gainsforth and Higley.5 After the introduction of osseo-integrated implants in restorative dentistry and oral surgery in the 1960s, it became widely accepted that this new armamentarium could be a useful source of anchorage in orthodontic practice.2 One of the earliest successful human results with miniscrews was in 1983, when a report was published about incisor elevation using a screw placed in the anterior nasal spine region.6 It was not until the 1990s that further experiments with non osseo-integrated titanium microscrew implants were published by Melsen et al and Kanomi, consecutively.7,8 Roberts et al were one of the first to publish studies about successful closure of first molar extraction sites, utilizing mini-implants in the retromolar region as anchorage.9
The mid-palatal implant as an anchorage device was first described in 1992 by Triaca and colleagues.10 The first author, who described a mini-implant exclusively for orthodontic use was Kanomi, in 1997.8 Costa et al then described a 2 mm diameter titanium miniscrew that could be used for direct or indirect anchorage in a preliminary report published the year after.11 This looked particularly at anchorage problems and relative solutions associated with deficient dentitions by evaluating the evidence on bone quality in dry skulls.
Titanium has long been established as the material of choice for implants but new designs and clinical applications for these anchorage devices are still being developed. The burgeoning numbers of case reports in peer reviewed journals are continuing to illustrate the versatility of TADs and their use in increasing numbers of clinical situations where anchorage is of concern.
The main indications for TADs to date have been:
Reinforcement of anchorage;
Movement of buccal teeth in a mesial or distal direction;
Movement of anterior teeth in a lingual or labial direction;
Movement of buccal or anterior teeth in a vertical intrusive direction.2,13,14
Mini-implants or miniscrews have been classified in various ways:
Position: the site of anchorage is dictated by the type and severity of the malocclusion. The most common insertion site is in the endosseous position but some implants may involve subperiosteal or transosseous positioning;
Implant surface: which may be rough or smooth;
Screw design: which determines the extent of support it attracts from its surrounding bone. The smooth, cylindrical design is thought to increase such support.3 Self-drilling or self-tapping (thread-forming) miniscrews eliminate the necessity of drilling pilot holes, which is appealing to orthodontists who increasingly are placing these devices themselves.
Various miniscrew head designs are also available: namely the bracket head or button head design, as well as the ‘through hole’ design which allows wire ligatures to be threaded through the head of the miniscrew that can be a very useful feature. The main purpose for these differing designs is to meet various skeletal anchorage requirements, by enabling the miniscrew to accept wires, hooks and elastics or even act as an orthodontic bracket. Most common TADs are produced in various lengths between 5 mm and 12 mm, and with diameters of 1.2 to 2.0 mm.
Advantages and disadvantages of these implants are summarized in Table 1. Examples of current systems include self-tapping screws, such as the Tomas, Imtec and the Orthoimplant. The Aarhus Mini-implant, originating from Denmark, stressed the possibility of immediate loading of such screws.15 The Spider Screw, which has been popularized in Italy, has a similar cylindrical design. Another popular self-drilling screw in the UK is the AbsoAnchor system originally developed in Korea.
Advantages
Disadvantages
Reduces need for patient compliance
Not ideal in mixed dentition stage
Eliminates need for ocular damage associated with headgear use
Possible root damage during micro-implant insertion
Relative ease of insertion
Possible infection
Good access to various placement sites
Possible failure
Ease of removal
Technique sensitive
Minimal discomfort and no residual surgical defects
Though the use of miniscrews has become widely popular throughout the nineties and is still one of the ‘hot topics’ in current orthodontic discussions, there is still a dearth of sound scientific evaluation in the form of clinical randomized controlled trials. The number of papers on this subject is enormous, over 3300 at the last count,16 and continues to expand, but many of these merely illustrate different clinical techniques and versatility of applications (Table 2) rather than adding to the body of ‘hard evidence’ on the subject.
Treatment of open bite
Park et al 200417Kuroda et al 200418Rachala & Harikrishnan 201019Kuroda et al 200720Vibhute 201021
Correction and space closure of Class III malocclusion
Buschang and Carrillo recently published the results of an electronic survey on the worldwide use of miniscrews amongst members of the American Association of Orthodontics (AAO). Out of 9,470 AAO members, a total of 564 members participated in this survey, giving a response rate of 6%. The survey included four main questionnaires with 28 multiple choice questions about miniscrew implant experience and training, techniques and type of cases, failures, patient experience and orthodontist satisfaction. Of the respondents, 42.6% had placed over 10 screws and, interestingly, more than half were now placing their own screws rather than referring this procedure to their surgical colleagues.40,14 The majority of clinicians had not received any specific training prior to their first screw placement, although this is generally recommended as studies have demonstrated lower failure rates in the more experienced operators.40
Efficacy
Osseo-integrated dental implants, such as the mid-palatal implants, have been reported to have a success rate ranging from 85% to 100% from human studies. Success rate in implant cases was defined by NICE as ‘stable anchorage for one year or until completion of orthodontic treatment’.41 A number of human studies have now revealed a success rate of more than 75% when orthodontic forces of 100–400 g are applied to such devices.16,42,43,44,45,46,47 The few comparative trials between mini-implant anchorage and conventional anchorage systems, such as headgear, showed that the former provide faster and effective anchorage reinforcement in cases of absolute anchorage.26,48,49,50,51,52 Crismani concluded that flap versus flapless placement and immediate versus delayed loading resulted in similarly successful outcomes.53
Failure of miniscrews has been reported to vary from 10% to 18% in recent years, and is the most commonly reported complication in the literature.2,13,54,55
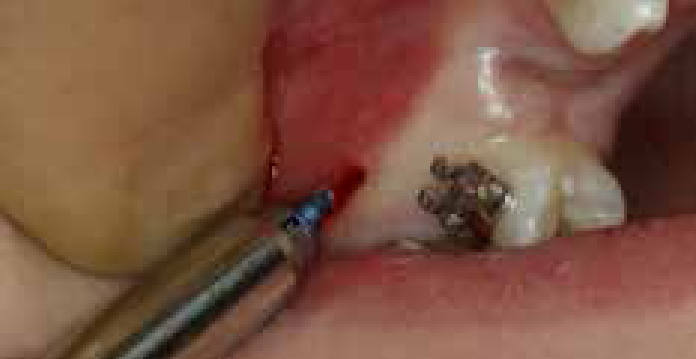
Breakages of miniscrews are rare and this could be because the quality of the bone is more dense or offers higher resistance to allow fracture of the titanium fixture (Figure 5). The clinician should also ensure, if at all possible, that the mini-implant is not placed directly into a root.14
Figure 5. Head of screw fractured during placement, thought to be due to very dense bone at the site.
Factors affecting success rates of miniscrews
Contra-indications for TADs are few but may include any systemic disease that results in poor bone quality. It is inadvisable to place miniscrews in a young child in the mixed dentition, especially in an area where there is a permanent successor tooth or insufficient inter-radicular space to accommodate the fixture.
The main factors reported to contribute to miniscrew failures are:
Improper surgical technique, possibly due to inadequate training which might lead to bone damage, root damage or miniscrew breakage.
Excessive force application: there have been no scientifically confirmed protocols for placing or loading miniscrews yet but, as their popularity increases, clinicians are generally opting for immediate loading with the use of lighter forces (50–75 g).
Inappropriate site: miniscrews are ideally placed in attached gingivae at the junction with the reflected mucosa where good quality bone is abundant. Ideally, this is in the inter-radicular spaces, mesial or distal to the bicuspids. The maxilla tends to offer higher success rates than the mandible.
Miniscrew factors, such as the type, diameter and length is thought to affect the success rate.
Host factors – smoking, parafunctional habits, poor bone quality and thin cortical bone.
Soft tissue response sometimes occurs such as peri-implantitis.
Chen et al reported, in their systematic reviews, that choice of implant size should depend on the quality and quantity of bone available. Although their evidence was not regarded as high quality, immediate implant loading in this study showed high success rates, with direct forces of up to 200 g, and resulted in shorter treatment time.53,56 Luzi et al also reported on the effectiveness of immediately loaded mini-implants, suggesting that the overall failure rate is not altered by the instant loading, especially when light forces are employed.57
Patients who smoke, or who are currently on bisphosphonates, predispose to higher failure rates and should only be treated on a case by case basis. Bayat reported a significantly higher failure rate of orthodontic miniscrews in heavy smokers than light or non-smokers.58
The main factors influencing the clinical success rate of mid-palatal miniscrews are the patient's age, with patients younger than 15 years increasing the failure risk; operator's skill;59 and placement of miniscrew in the palatal suture.44
Despite the implications of the above factors in miniscrew failures, stability or loosening of the screw is difficult to predict, therefore each patient should be warned specifically of the possibility of loss or failure of the implant during the consent process.
Operative factors
Several clinical guidelines on the placement have been proposed. Miniscrews are typically placed under topical or minimal local infiltration anaesthesia. They can be drilled or screwed into the bone cortex using a hand screwdriver or a contra-angled driver, either with or without prior pilot hole preparation. Procedure time ranges from 5 to 15 minutes, depending on the operator and the patient.60,61
Lee et al described the premolar and subapical areas in the anterior region as being the most reliable for orthodontic miniscrew placement. A depth of more than 4 mm of alveolar bone is easily available in intermolar regions and between the second premolar and the first molar in both arches.55,62 Adequate bone depth and appropriate miniscrew orientation will affect the resistance to failure on the implant-bone interface.63 Miniscrew placement at a high level, in non-keratinized mucosa, has been reported to promote an unwelcome inflammatory hypertrophic tissue response, a significant predictor for failure, especially in the mandible.47,64
Safety
Despite all the possible insertion sites discussed, the most common site is in the keratinized gingivae of the inter-radicular space between upper second premolar and first molar. There is always the possibility of root damage during insertion of the TAD, necessitating a careful clinical technique. Clinical and histological observations have shown that, if the implant touches the tooth during placement or subsequent tooth movement, the respective root areas react by initiating resorptive processes. Reports have demonstrated, however, that elimination of contact will swiftly lead to cementum deposition and full root recovery within a few weeks.65,66
Poggio et al suggested a 1 mm safety margin between a miniscrew and a root for both periodontal health and miniscrew stability. It could also therefore be recommended that miniscrews with a diameter of 1.5 mm or less are adequate for insertion into an inter-radicular bone of at least 3.5 mm.67 Unfortunately, the conclusions from these studies on safety are only based on small patient samples, and further work in this field is required.
Patient acceptability
For any orthodontic treatment to progress successfully, it is usually important for the patient to be co-operative and compliant. Patients' levels of compliance are affected by their experience of pain and discomfort. Oliver and Knapman reported that the fear of pain was a major factor in preventing patients from seeking orthodontic treatment, and that 39% of patients thought the worst aspect of treatment was the pain.68
Temporary anchorage devices seem to be well-tolerated by patients but scientific studies related to this subject are quite scarce in the literature.69 Placement of these temporary anchorage devices has been rated less painful compared to other orthodontic procedures or tooth extractions, even though patients tend to expect otherwise.46,70 Miniscrews placed without flap surgery are more acceptable for patients than miniplates or other devices which are surgically placed using flaps.45
A recently published randomized controlled trial by Baxmann et al71 compared pain ratings of patients who had had microimplant placement, tooth extraction and gingival tissue removal in preparation for implant placement. Their results showed that microimplant placement, especially the transgingival method, produced significantly lower pain levels than the other methods.
Conclusion
From the many case reports, case series and the few randomized clinical studies on the subject, we can suggest that temporary anchorage devices initially appear to be a safe and effective alternative to conventional methods of anchorage, such as headgear.
They may also turn out to be a more acceptable and more comfortable alternative for many orthodontic patients. These conclusions, however, need to be supported by further high quality randomized clinical trials before they can be accepted as absolute fact.