Hamdan AM, Al-Omari IK, Al-Bitar ZB Ranking dental aesthetics and thresholds of treatment need: a comparison between patients, parents, and dentists. Eur J Orthod. 2007; 29:(4)366-371
Keene HJ Distribution of diastemas in the dentition of man. Am J Phys Anthrop. 1963; 21:437-441
Richardson ER, Malhotra SK, Henry M, Little RG, Coleman HT Biracial study of the maxillary midline diastema. Angle Orthod. 1973; 43:438-443
Gelgor IE, Karaman AI, Ercan E Prevalence of malocclusion among adolescents in Central Anatolia. Eur J Dent. 2007; 1:(3)125-131
McVay TJ, Latta GH Incidence of the maxillary midline diastema in adults. J Prosthet Dent. 1984; 52:809-811
Steigman S, Weissberg Y Spaced dentition. An epidemiologic study. Angle Orthod. 1985; 55:167-176
Angle EH, 7th edn. Philadelphia: SS White Dental Manufacturing Company; 1907
Andrews LF The six keys to normal occlusion. Am J Orthod. 1972; 62:296-309
Becker A The median diastema. Dent Clin North Am. 1978; 22:685-710
Oesterle LJ, Shellhart WC Maxillary midline diastemas: a look at the causes. J Am Dent Assoc. 1999; 130:85-94
Broadbent BH Ontogenetic development of occlusion. Angle Orthod. 1941; 11:223-241
Weyman J The incidence of median diastema during the eruption of the permanent teeth. Dent Pract Dent Rec. 1967; 17:276-278
Huang WJ, Creath CJ The midline diastema: a review of its etiology and treatment. Pediatr Dent. 1995; 17:(3)171-179
Taylor JE Clinical observations relating to the normal and abnormal frenum labii superians. Am J Orthod. 1939; 25:646-660
Sanin C, Sekiguchi T, Savara BS A clinical method for the prediction of closure of the central diastema. ASDC J Dent Child. 1969; 36:415-418
Baum AT The midline diastema. J Oral Med. 1966; 21:30-39
Gass JR, Valiathan M, Tiwari HK, Hans MG, Elston RC Familial correlations and heritability of maxillary midline diastema. AmJ Orthod Dentofacial Orthop. 2003; 123:35-39
Nainar SM, Gnanasundaram N Incidence and etiology of midline diastema in a population in south India (Madras). Angle Orthod. 1989; 59:277-282
Shashua D, Artun J Relapse after orthodontic correction of maxillary median diastema: a follow-up evaluation of consecutive cases. Angle Orthod. 1999; 69:257-263
Schmitt E, Gillenwater JY, Kelly TE An autosomal dominant syndrome of radial hypoplasia, triphalangeal thumbs, hypospadias, and maxillary diastema. Am J Med Genet. 1982; 13:63-69
Isaacson KG, Reed RT, Muir JDOxford: Wright; 2003
Kaimenyi JT Occurrence of midline diastema and frenum attachments among school children in Nairobi, Kenya. Indian J Dent Res. 1998; 9:67-71
Adams CP The relation of spacing of the upper central incisors to abnormal labial frenum and other features of the dento-facial complex. Dent Pract Dent Rec. 1954; 74:72-86
Sicher H, 2nd edn. St Louis: CV Mosby Co; 1952
Edwards JG The diastema, the frenum, the frenectomy: a clinical study. Am J Orthod. 1977; 71:489-508
Popovich F, Thompson GW, Main PA Persisting maxillary diastema: indications for treatment. Am J Orthod. 1979; 75:(4)399-404
Tait CH The median frenum of the upper lip and its influence on the spacing of the upper central incisor teeth. Dent Cosmos. 1934; 76:991-992
Koora K, Mutthu MS, Rathna PR Spontaneous closure of midline diastema following frenectomy. J Indian Soc Pedod Prev Dent. 2007; 25:23-26
James GA Clinical implications of a follow-up study after fraenectomy. Dent Pract Dent Rec. 1967; 17:299-305
Nielsen IL Vertical malocclusions: etiology, development, diagnosis and some aspects of treatment. Angle Orthod. 1991; 61:(4)247-260
Gellin ME Digital sucking and tongue thrusting in children. Dent Clin N Am. 1978; 22:(4)603-619
Curzon ME Dental implications of thumb-sucking. Paediatrics. 1974; 54:(2)196-200
Jian XC Surgical management of lymphangiomatous or lymphangiohemangiomatous macroglossia. J Oral Maxillofac Surg. 2005; 63:(1)15-19
Little RM Stability and relapse of dental arch alignment. Br J Orthod. 1990; 17:235-241
Miller WB, McLendon WJ, Hines FB Two treatment approaches for missing or peg-shaped maxillary lateral incisors: a case study on identical twins. Am J Orthod. 1987; 92:249-256
Counihan D The orthodontic restorative management of the peg-lateral. Dent Update. 2000; 27:(5)250-256
Sykaras SN Mesiodens in primary and permanent dentitions. Report of a case. Oral Surg Oral Med Oral Pathol. 1975; 39:870-874
Ferres-Padro E, Prats-Armengol J, Ferres-Amat E A descriptive study of 113 unerupted supernumerary teeth in 79 pediatric patients in Barcelona. Med Oral Patol Oral Cir Bucal. 2009; 14:E146-E152
Garvey MT, Barry HJ, Blake M Supernumerary teeth – an overview of classification, diagnosis and management. J Can Dent Assoc. 1999; 65:612-616
Zhu JF, Marcushamer M, King DL, Henry RJ Supernumerary and congenitally absent teeth: a literature review. J Clin Pediatr Dent. 1996; 20:87-95
Liu JF Characteristics of premaxillary supernumerary teeth: a survey of 112 cases. ASDC J Dent Child. 1995; 62:262-265
Russel KA, Folwarczna MA Mesiodens – diagnosis and management of a common supernumerary tooth. J Can Dent Assoc. 2003; 69:362-366
Van Buggenhout G, Bailleul-forestier I Mesiodens. Eur J Med Genet. 2008; 51:(2)178-181
Bishara SE, Jakobsen JR Individual variation in tooth size-arch length changes from the primary to permanent dentitions. World J Orthod. 2006; 7:145-153
Beasley WK, Maskeroni AJ, Moon MG, Keating GV, Maxwell AW The orthodontic and restorative treatment of a large diastema: a case report. Gen Dent. 2004; 52:(1)37-41
Thilander B Orthodontic space closure versus implant placement in subjects with missing teeth. J Oral Rehab. 2008; 35:64-71
Chasens AI Periodontal disease, pathologic tooth migration and adult orthodontics. NY J Dent. 1979; 49:40-43
Sutton PR, Graze HR The blood-vessel thrust theory of tooth eruption and migration. Med Hypotheses. 1985; 18:289-295
Lee JW, Lee SJ, Lee CK, Kim BO Orthodontic treatment for maxillary anterior pathologic tooth migration by periodontitis using clear aligner. J Periodontal Implant Sci. 2011; 41:(1)44-50
Melsen B Tissue reaction to orthodontic tooth movement – a new paradigm. Eur J Orthod 2001;. 23:671-681
Hussels W, Nanda RS Effect of maxillary incisor angulation and inclination on arch length. Am J Orthod Dentofacial Orthop. 1987; 91:(3)233-239
Serra GS, Aytes LB, Escoda CG Erupted odontomas: a case report of three cases and review of literature. Med Oral Patol Oral Cir Bucal. 2009; 14:299-303
Frank C Treatment options for impacted teeth. J Am Dent Assoc. 2000; 131:623-632
Neville BW, Damm DD, Brock T Odontogenic keratocysts of the midline maxillary region. J Oral Maxillofac Surg. 1997; 55:340-344
Hadi U, Younes A, Ghosseini S, Tawil A Median palatine cyst: an unusual presentation of a rare entity. Br J Oral Maxillofac Surg. 2001; 39:(4)278-281
Manzon S, Graffeo M, Philbert R Median palatal cyst: case report and review of literature. J Oral Maxillofac Surg. 2009; 67:(4)926-930
Lamberton CM, Reichart PA, Triratananimit P Bimaxillary protrusion as a pathologic problem in the Thai. Am J Orthod. 1980; 77:(3)320-329
Kokich VG, Nappen DL, Shapiro PA Gingival contour and clinical crown length: their effect on the esthetic appearance of maxillary anterior teeth. Am J Orthod. 1984; 86:59-94
Diwan AH, Graves ED, King JA, Horenstein MG Nuchal-type fibroma in two related patients with Gardner's syndrome. Am J Surg Pathol. 2000; 24:1563-1567
Tabbaa S, Guigova I, Preston CB Midline diastema caused by tongue piercing. J Clin Orthod. 2010; 28:426-428
Durbin DD Relapse and the need for permanent fixed retention. J Clin Orthod. 2001; 35:(12)723-727
Bearn DR Bonded orthodontic retainers: a review. Am J Orthod Dentofacial Orthop. 1995; 108:(2)207-213
Maxillary midline diastema is a common aesthetic complaint of patients. Treating the midline diastema is a matter of concern for practitioners, as many different aetiologies are reported to be associated with it. The appearance of midline diastema as part of the normal dental development makes it difficult for practitioners to decide whether to intervene or not at an early stage. The aim of this article is to review the possible aetiology and management options which will help the clinician to diagnose, intercept and to take effective action to correct the midline diastema. The available data shows that an early intervention is desirable in cases with large diastemas. Treatment modality, timing and retention protocol depends on the aetiology of the diastema. Therefore, priority needs to be given to diagnosing the aetiology before making any treatment decisions.
Clinical Relevance: This article aims to determine and evaluate the aetiology and possible treatment options of midline diastema.
Article
Aesthetics and function are the two most important goals of modern-day dentistry.1 An attractive well balanced smile and a confident speech are valuable personal assets. Maxillary midline diastema is one of the most frequently seen malocclusions and its incidence ranges from 1.6% to 25.4% and is inversely proportional to age.2,3,4,5,6
Angle7 described the midline diastema as a common form of incomplete occlusion characterized by a space between the maxillary and, less frequently, mandibular central incisors. In his classical article, Andrews8 stated that interdental diastemas should not exist and all contacts should be tight so that the patient has ‘straight and attractive teeth as well as a correct overall dental occlusion’.
Maxillary anterior spacing or diastema is considered unaesthetic and unacceptable by the general population.
Treating the midline diastema is a problem for the dental practitioner as many different aetiologies are reported to be associated with it.9,10 Many researchers, like Broadbent,11 consider midline diastema as an ‘ugly duckling stage’ and explain this phase as a transitional phase in the dental development. He also describes the closure of the diastema with the complete eruption of lateral incisors and canines as a normal stage in dental development.12 However, the persistence of the midline diastema, even after the eruption of the permanent canines, in some cases requires investigation into the underlying causes and possible preventive and corrective treatment options.13 The aim of this review article is to determine and evaluate the possible aetiology of the midline diastema and consider the management options which may help the clinician to diagnose, intercept and take effective measures to correct the unaesthetic diastema.
To intervene or not to intervene
A major problem for the dentist in dealing with the midline diastema is the decision to intervene or not to intervene during the early mixed dentition period. As it is widely stated and presumed that the midline diastema during the ‘ugly duckling stage’ is a normal phenomenon and is self-correcting, it is tempting for the dentist to suggest to the parents of the child to wait until the permanent canines erupt.
After a study on midline diastema, Taylor14 concluded that 98% of six-year-old children presented with a midline diastema. As age increased, the percentage significantly decreased. The 10–11 year-old group showed a midline diastema in 48.7% and, in the sample of 12–18 year-old students, the figure dropped to 7%. As per the literature and our personal experience, in 90% of the cases the diastema is self-correcting. The problem arises in the remaining 10% or so of the cases where the reassured patients return with disappointment that the unpleasing space between their central incisors has not closed, even after the eruption of the permanent canines; as suggested earlier by the dentist.
Prediction of the fate of midline diastema
The decision to intervene early during the mixed dentition period depends on knowing whether the diastema will close on their own as age increases. Sanin et al15 developed a method that could predict whether the space would close spontaneously in the developing dentition. This method is based on millimetre measurements in the early mixed dentition and is claimed to have an accuracy of 88%. As the size of the diastema increases the possibility of space closure without treatment reduces.
Sanin's prediction is as follows:
For a 1 mm space in the early mixed dentition the possibility of spontaneous space closure is 99%;
For a 1.5 mm space the possibility is 85%;
For a 1.85 mm diastema it is 50%;
For a 2.7 mm space the possibility of closure without treatment is only 1%.
The measurement should be made after the eruption of the lateral incisors. Hence it is advisable to intervene early if the midline diastema is more than 1.85 mm after the eruption of the permanent lateral incisors.
Aetiology and effective treatment options
To treat the midline diastema effectively, an accurate diagnosis of the aetiology and an intervention relevant to the specific aetiology is necessary. Timing of the treatment is important to achieve satisfactory results. Most of the researchers do not recommend tooth movement until the eruption of the permanent canines.16 But in certain cases, where very large diastemas exist, treatment can be initiated early.
The following are the well established and narrated causes and treatment options for the midline diastema in the literature.
Genetics and midline diastema
Gass et al,17 after a study on 30 extended families, came to the conclusion that genetics has a possible role in the presentation of midline diastema. Heritability was estimated at 0.32% for a white and 0.04% for a black population. Nainar and Gnanasundaram18 noted in their study of midline diastemas on 9774 Southern Indian individuals, that there was a relatively increased frequency of familial occurrence and hence proposed the presence of a genetic factor in the expression of midline diastema. Shashua and Artun,19 after a study about the causes of midline diastema, concluded that the family tree of the diastema was one of the two important risk factors for diastema relapse. The other factor was diastema size before treatment. Many other authors, like Gardiner20 and Schmitt et al,21 also consider genetics as a main cause for the midline diastema. Treatment methods include orthodontic correction with a fixed or removable appliance and prosthetic correction with composites and crowns (Figure 1). If the diastema is large, it is advisable to close the space using orthodontic appliances. In most cases, simple removable appliances incorporating finger springs or a split labial bow can give good results.22
Figure 1.
(a) A case with midline diastema. (b) Closure of midline diastema with composite restoration.
Superior labial frenum
A hypertrophic labial frenum may be considered as a major aetiological factor for midline diastema.23,24 In a thick and fleshy labial frenum, the fibro-elastic band crosses the alveolus and inserts into the incisive papilli, preventing the approximation of the maxillary central incisors (Figure 2).
Figure 2. Midline diastema due to high frenal attachment.
Most of the researchers, like Angle,7 Sicher,25 Gardiner,20 and Edwards,26 are of the opinion that superior labial frenum causes midline diastema. Some researchers, like Popovich et al, believe that there is an inverse relationship between high frenal attachment and midline diastema.27 According to them, labial frenum persists owing to the existing diastema and, as the dentition applies little or no pressure on the tissues, there is little or no atrophy of the frenum.28 But most of the researchers agree that removal of the high bulbous labial frenum is important for the stability after the closure of the midline diastema.29
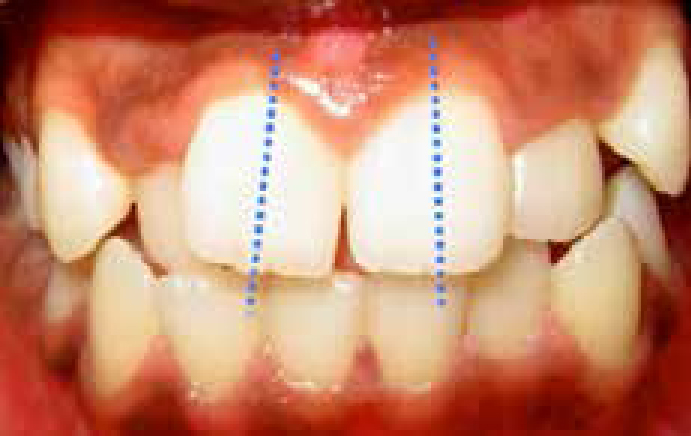
The blanching test (Figure 3) is a simple diagnostic test to predict whether the frenum will unfavourably influence the development of the anterior occlusion. It is performed by applying intermittent pressure on the frenum by elevating the lip. If a heavy band of tissue with a broad fan base is attached to the palatine papilla, and if it blanches on applying pressure, it can be concluded that the frenum is at an unfavourable position for the existence of a normal tight contact between the central incisors.29
Figure 3. Blanching test.
There is also confusion as to whether to carry out a frenectomy (Figure 4) before or after orthodontic space closure. As one study has shown, in some cases, some midline space closure is seen after a frenectomy without orthodontic treatment.21 This makes it tempting for the dentist to advise patients to undergo this procedure before the orthodontic space closure. However, another author advises a frenectomy procedure after the correct positioning of the central incisors when the diastema is closed.30 The basis behind this thought is that, if the excess tissue is removed after the teeth have been squeezed together, the healing and the scar tissue will be formed around the closed teeth. If a frenectomy is done prior to the orthodontic space closure, the scar tissue is formed between the teeth, increasing the risk of relapse.
Figure 4. Post frenectomy.
Anterior traumatic bite
Excessive anterior overbite is another major contributing factor for midline diastema.10 As a result of trauma to the maxillary anteriors from the mandibular incisors, the maxillary incisors procline. This results in an increase of the upper arch circumference, leading to a diastema (Figure 5). Practitioners should not fail to identify deep bite as an aetiology for the diastema. Any attempt to close the midline spacing without correcting the deep bite and anterior traumatic bite will lead to a speedy relapse of the condition.
Figure 5. Proclination of maxillary anteriors and midline diastema due to anterior traumatic bite.
Possible causes underlying the deep bite can be excessive vertical alveolar development of the mandibular or the maxillary incisors, inadequate vertical dimension of posterior occlusion (molars) and skeletal conditions like increased ramal height.31 Proper orthodontic evaluation and apt treatment modalities, like intrusion of anteriors, extrusion of posteriors or even surgical intervention may be necessary.
Oral habits
Oral habits such as tongue thrusting and finger sucking can be other aetiological factors for the appearance of the midline diastema.32,33 According to Proffit and Fields,34 tongue position at rest may have a greater impact on tooth position than tongue pressure, as the tongue only briefly contacts the lingual surface of the anterior teeth during thrusting. The tongue pushes the anterior teeth to a forward position, increasing the circumference which results in spacing (Figure 6).
Figure 6. Diastema due to tongue thrusting.
An abnormal habit of the tongue can be detected by the tip of the tongue popping out through the anterior spacing when the patient is asked to swallow. In cases of anterior open bite, the tongue may be seen thrusting between incisal edges of the maxillary and mandibular incisors. Patients with tongue thrust often produce a snap sound on swallowing and also have hyperactivity of the orbicularis oris muscle.
An abnormal tongue size is a severe problem which may create difficulties in retaining the orthodontically corrected midline diastema. Macroglossia can be detected by simple observations. The patient can be asked to touch the tip of the nose with his tongue and, if he/she is able to do that, it is an indication of an extended tongue (Figure 7). In the same way, if tooth indentations are seen on the lateral borders of the tongue, it can be an indication of an enlarged tongue (Figure 8). In such cases, surgical trimming may have to be considered in order to attain stability in the dental occlusion.35
Figure 7. Extended tongue.Figure 8. Tooth indentations on the lateral borders of the enlarged tongue.
Deleterious habits have to be corrected by using habit-breaking appliances and by psychological approaches. The use of fixed tongue cribs are found to be effective in breaking the tongue-thrusting habit.36
Peg-shaped laterals
A common cause of tooth size discrepancy is the peg-shaped maxillary lateral incisors (Figure 9). The reduced size of the maxillary lateral incisor will allow the distal drifting of the central incisors, creating a midline diastema.
Figure 9.
(a, b) Distal drifting of centrals and midline diastema due to peg-shaped lateral incisors.
If the reason for midline diastema is peg laterals, the space between the central incisors is closed; respecting the midline and the space necessary for the prosthetic restoration of the peg-shaped lateral is created by moving the peg lateral into a position between the central incisor and the cuspid. The best contour and aesthetics will be achieved if the peg lateral is more mesial in space. This can be done by simple removable orthodontic appliances incorporating finger springs or split labial bows. Depending on the complexity of the occlusion, a fixed orthodontic appliance can also be considered.37.38
Supernumerary teeth/mesiodens
A mesiodens is a supernumerary tooth which is present in the midline between the two maxillary central incisors (Figure 10).39 A mesiodens accounts for 80% of all supernumerary teeth.40 It may erupt normally, remain impacted, appear inverted or take a horizontal position.41,42 The presence of a mesiodens can prevent the close approximation of the central incisors leading to a midline diastema and can also lead to several other complications, such as impaction, delayed and ectopic eruption of adjacent teeth, crowding, axial rotation, displacement, radicular resorption of adjacent teeth and dentigerous cyst.43 Russel and Folwarczna have suggested the extraction of a mesiodens in the early mixed dentition period. According to them this will help in better alignment of teeth and will also minimize the need for orthodontic treatment.44 Some authors, like Mitchell and Bennett, have advocated the late extraction of mesiodens when the adjacent permanent incisors have completed their root formation.45 If the mesiodens exists during the permanent dentition period, extraction of the mesiodens followed by space closure utilizing fixed orthodontic appliances will be the line of treatment.46
Figure 10. Mesiodens causing rotation of the maxillary right central incisor and midline diastema.
Tooth size, arch size discrepancy
Tooth size, arch size discrepancy is another major cause for diastema.47 The combination of large jaws, normal or small teeth can be due to inherited characteristics. But in some cases it can be due to endocrine imbalances. Conditions such as acromegaly can cause abnormally large jaws relative to the teeth size. Normal-sized jaws and small teeth can also cause generalized spacing. One treatment option will be to retract the teeth in order to reduce the arch perimeter, considering a patient's profile as well as aesthetic and functional aspects. Another option will be to realign the teeth and close the spaces with a combination of orthodontic and prosthodontic approaches.48
Missing teeth
If the diastema is due to missing teeth, prosthetic replacement or a combination of orthodontic and prosthetic rehabilitation is the treatment option. If the absence of a lateral incisor is the cause of the diastema, there are two available options following midline diastema closure, ie mesial movement of the canine to the position of the missing lateral incisor or distalization of the canine to allow prosthetic replacement of the missing lateral incisor (Figure 11).48,49
Figure 11. Midline diastema due to missing lateral incisors.
Pathologic migration of teeth
Pathologic tooth migration is the displacement of teeth resulting from the imbalance of the tooth retention forces (Figure 12).50 Several factors such as destruction of periodontium, inflammation in the periodontal tissue, eruption force, oral habits and occlusal forces are reported to be responsible for pathological tooth migration. Inflammation in the periodontal tissue increases hydrodynamic and hydrostatic forces around relevant vessels and tissues, possibly resulting in tooth displacement.51 As extrusion is a common clinical feature of pathologic tooth migration, eruption force is also considered to be a contributing factor. Treatment options for pathological tooth migration include removal of aetiological factors and orthodontic treatment, depending on the severity of migration, available bone support and extent of extrusion of the teeth.52 Active orthodontic intrusion after basic periodontal therapy is reported to be an effective treatment option.53
Figure 12. Midline diastema due to pathologic migration of teeth.
Angulation of teeth
Distal crown inclination of the incisors can create an appearance of the diastema even though the incisors are in contact at the cervical region (Figure 13). With excessive distal crown inclination, the contact between the teeth will be limited only in the proximal gingival region, keeping the incisal tips farther apart, leaving what appears to be a diastema at the incisal edge of the teeth. The treatment option in such cases will be to change the crown angulations orthodontically so that the incisal edge of the incisors are in contact.54
Figure 13. Appearance of midline diastema due to the distal crown inclination of the central incisors.
Odontomas occurring in the maxillary midline
Odontomas are benign odontogenic tumours composed of enamel, dentine, cementum and pulp tissue. Odontomas are the most frequent odontogenic tumours, with an incidence of 22–67% of all maxillary tumours. They are usually asymptomatic, but often associated with tooth eruption disturbances.55 Odontomas can be present between the roots of erupted maxillary central incisors, preventing contact between their crowns and causing large diastemas. A radiographic examination of the site will be beneficial in cases of a large diastema to rule out the presence of any midline lesions such as odontomas, when the presence of other common aetiological factors are not observed. The treatment of choice is surgical removal of the tumour and closure of the midline diastema using composites, jacket crowns or orthodontic appliances, depending on the size of the diastema.56
Developmental cysts in the orofacial midline
An odontogenic keratocyst can appear in the maxilla and can displace teeth, leading to spacing in the anterior region.57 A median palatal cyst is another midline structure which is a rare cyst originating from the epithelium trapped along the line of fusion of the lateral palatal maxillary process during development.58,59
Flaccid lips
In patients with hypotonic lips the teeth may move and stay in a labial or buccal position due to the tongue pressure which will lead to wide ovoid arches without interproximal teeth contact.60
Other less commonly occurring factors
Other factors which can cause midline diastema include missing or fractured teeth due to trauma and fibromas in the maxillary midline.61,62 Rare incidents of development of midline diastema due to the habitual placing of a metallic tongue piercing stud between the maxillary central incisors have been reported.63
Stability after diastema closure
Relapse is a major concern in the correction of midline diastema. Exact diagnosis and removal of the aetiology is the key to obtaining a stable result. Long-term use of retainers or even permanent bonded lingual retainers are advocated, especially in cases with large diastema.64,65,66,67 Large pre-treatment diastema and the presence of at least one family member with a similar condition increases the risk of relapse.19
Conclusion
Midline diastema is usually a part of normal dental development and hence its presence during the mixed dentition period is not a matter of concern. However, if the diastema is more than 1.8 mm, even after the eruption of lateral incisors, an orthodontic intervention will be necessary.
Several aetiological factors are reported and discussed in the literature and no single aetiological factor is agreed upon for the development of a midline diastema. A radiographic examination of the site will be beneficial to rule out any multifactorial aetiology. To achieve an aesthetic and stable result, it is important to establish the underlying cause for the midline diastema. Retention protocol should depend on the size and the aetiology of the midline diastema.