This article examines the key areas relating to interceptive orthodontics, ie crossbites, anterior and posterior; eruption problems and impaction (including incisors and canines); poor quality first permanent molars; infra-occluded primary molar teeth; non-nutritive sucking habits (digit and pacifier sucking) leading to anterior openbite, posterior crossbite and increased overjet; centreline shifts related to unilateral loss of primary teeth; and increased overjet and associated risk of trauma. It aims to provide information and recommendations.
Clinical Relevance: The GDP requires evidence to support the clinical management of common problems presenting in the mixed dentition.
Article
Interceptive orthodontics is a term that is used to encompass many treatments for different problems arising in the developing dentition. Studies have identified that between 26% and 39%1–4 of children have malocclusions that require treatment, depending on the age range investigated. Interceptive orthodontic treatment potentially reduces the need for complex orthodontic treatment5 and, therefore, may be of particular benefit to patients and clinicians in areas where there is limited access to specialist orthodontic services. The GDP plays a very important role in the identification and diagnosis of orthodontic problems presenting early, and assessing the potential for their development. It is believed that, if intercepted and correctly managed during the mixed dentition, many malocclusions can be eliminated or reduced in severity.6 The following areas, already mentioned, will be explored, highlighting current best practice recommendations:
Crossbites, anterior and posterior;
Eruption problems and impaction (including incisors and canines);
Poor quality first permanent molars;
Infra-occluded primary molar teeth;
Non-nutritive sucking habits (digit and pacifier sucking) leading to anterior open bite, posterior crossbite and increased overjet;
Centreline shifts related to unilateral loss of primary teeth; and
Increased overjet and associated risk of trauma.
Anterior crossbite
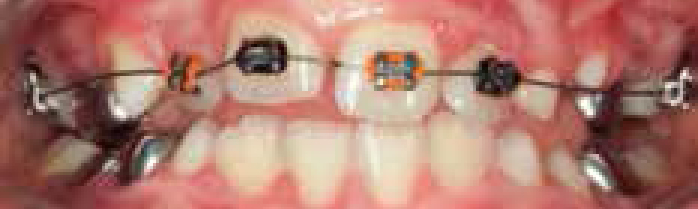
Anterior crossbite occurs when one, or more, lower incisor teeth occlude anterior to the upper incisor teeth. If left untreated, it may cause attrition to the labial surface of the upper incisor, fractures or mobility of incisor teeth or gingival recession. There is a variety of treatment options, including removable and fixed orthodontic appliances. A recent systematic review found little high quality evidence in this area and suggested that the evidence does not strongly support one treatment option over another.7 The evidence suggests that treatment involving modification to the upper or lower incisal edges, either in the form of a temporary crown or composite build-up (Figure 1), gives correction of a single tooth anterior crossbite in a few weeks, but this is only based on case reports. Fixed orthodontic appliances, in the form of a ‘2 x 4’ appliance appeared to correct the crossbite within six weeks to three months, based on cohort studies (Figure 2). Surprisingly, no studies investigated the use of an upper removable appliance in this situation.
Figure 1. Composite incisal build-up.Figure 2. A ‘2 x 4’ appliance.
Recommendation
Although there is no conclusive evidence as to the most effective overall option for correcting an anterior crossbite in the mixed dentition, a ‘2 x 4’ fixed appliance or modification to incisal edges appear to be most effective in terms of treatment time.
Posterior crossbite
Posterior crossbite can occur in the premolar or molar region, with one or more teeth involved. The purpose of treatment is usually to expand the maxillary arch, to correct the crossbite, and eliminate the mandibular displacement, as the aetiology is normally due to a narrow maxillary arch. A Cochrane review entitled ‘Orthodontic treatment for posterior crossbites’8 found that grinding of primary teeth to remove occlusal interferences or the provision of a quadhelix to provide maxillary arch expansion are effective treatment options.
Since the publication of this review, Petrén and co-workers9 have conducted a Randomized Controlled Trial (RCT). They concluded that, if unilateral posterior crossbite is planned to be corrected in the mixed dentition, treatment with a quadhelix is a more successful and quicker method of treatment than an Upper Removable Appliance (URA) expansion plate. The same authors have since published three-year follow-up results,10 and have shown that there is similar long-term stability regardless of appliance type.
Recommendations
Although a quadhelix appliance (Figure 3) corrects a posterior crossbite more quickly in the mixed dentition, a URA provides an equally stable method. In selected cases, the crossbite may be eliminated through careful grinding of the primary canines.
Figure 3. A quadhelix.
Impacted maxillary permanent central incisors
Maxillary permanent central incisors usually erupt around the age of six to seven years, and prior to the eruption of maxillary permanent lateral incisors. Any delay in eruption or abnormality in eruption sequence should be viewed with suspicion and investigated. The two main causes for non-eruption of the permanent incisors are trauma to the primary dentition, or supernumerary teeth blocking the path of eruption for the permanent teeth.11 It is emphasized that radiographic examinations of all children who present clinically with evidence of delayed permanent tooth eruption, or temporary tooth displacement (with or without a history of trauma), should be performed.12
The Royal College of Surgeons of England (RCSEng) has published guidelines on the management of unerupted maxillary incisors,13 which are summarized in Table 1. These are based on the available evidence, which consist of no controlled trials, 23 retrospective case studies and 4 epidemiological studies, and other low grade evidence. Nonetheless, they give a recommendation for management of the child, and are clearly divided into different stages of development of the central incisor. It is also important to stress the importance of maintaining space, awaiting the eruption of the central incisor, following the loss of the primary central incisor, something that is not obvious from the guidelines.
Age of child/Stage of development of incisor
Recommendation
Children up to nine years of age with incomplete root development of permanent incisor
Remove the obstruction;
Do not uncover bone from the unerupted incisor – maintain integrity of the follicle;
Create space if required;
Monitor eruption for 18 months (80% erupt spontaneously);
If exposure is required, expose minimally to eliminate soft tissue obstruction;
If the tooth is still high, expose and bond bracket.
Children above nine years of age, with complete or nearly complete apex
Remove the obstruction;
Create space if required;
If the permanent incisor is high monitor eruption for 12 months;
If the tooth is still unerupted at 12 months, expose and bond bracket as required.
Children referred late (over 10 years of age)
Remove the obstruction, expose and bond bracket at first operation.
The aetiology of impacted maxillary permanent canines appears to be multifactorial, including links to small or developmentally absent lateral incisors,14 family history,15 and Class II division 2 malocclusion.16
A Cochrane review investigating the effect of extraction of primary canines on ectopic permanent canines17 identified two RCTs. It stated that there is ‘a suggestion from the literature that extraction of the primary canine may help eruption of the permanent canine.’
Since the publication of the Cochrane review, there have been several studies investigating the interceptive management of ectopic maxillary canines looking at the effect on the position of the canine following creating space.18–21 Despite these studies having some methodological flaws, they suggest that space creation increases the chance of eruption of the canine.
Two further studies have examined the idea of space creation and the effect of extraction of the primary canine plus primary first molar, compared with extraction of only the primary canine.22,23 Both of these studies appear to support the favourable effect of space creation in facilitating the eruption of the canine, but fail to mention any long-term effect this has on crowding or any child-centred outcomes.
Recommendations
Consider creating space in the mixed dentition for the ectopic canine to increase its chance of eruption, whether that is by primary extractions, or by arch expansion, or a combination of both.
First permanent molars with poor prognosis
First Permanent Molars (FPMs) have the poorest long-term prognosis of all permanent teeth owing to their susceptibility to caries in childhood, and their association with Molar Incisor Hypomineralization (MIH).24,25 Ideal timing of extraction of FPMs with poor prognosis can lead to an acceptable occlusion,26,27 with successful mesial migration of the second permanent molars.
The national guidance document, produced by the RCSEng, assists with treatment planning when considering extraction of FPMs in children.28 It stresses the importance of timing of the extraction of the lower FPM, with the timing of the upper extractions being less crucial. It is advocated that the lower FPM should ideally be extracted when there is radiographic evidence of early dentine calcification within the second molar root bifurcation, usually occurring in children around 8–10 years.27,29
These guidelines discuss compensating extractions, and recommend extraction of the upper FPM if extraction of the lower FPM is required in Class I malocclusions to prevent the theoretical risk of the upper FPM overerupting and preventing the lower second molar from drifting forward. The work by Holm30 is used as the main source for supporting compensating extractions. He reviewed 1,119 cases involving loss of one or more FPMs over a 10-year period, and assessed the proportion of cases involving loss of FPMs, and the patterns of extraction. He reported that the poorest outcomes following orthodontic treatment were found in cases of uncompensated extraction of lower FPMs, but there were no data presented to support this.
More recently, Mejàre et al31 have reviewed 32 patients who had lost one or more FPMs in childhood due to MIH. Five patients had an uncompensated extraction of a lower FPM, and no-one had over eruption of the upper FPM noted. Jälevik and Möller,32 in a longitudinal study, reported no significant occlusal problems in children with uncompensated extractions of lower FPMs, and recommended against the need for compensating extractions.
An RCT is currently underway in Scotland to answer the question of the need to perform a compensating extraction when extracting a lower FPM, and the protocol has been published.33
Recommendation
Follow RCS guidelines until further evidence available.
Infra-occluded second primary molars
The term infra-occluded describes a tooth when it is situated below the occlusal plane and, commonly, the term ‘submerged’ has been used. Infraocclusion can occur whether or not there is a developing premolar. One recent study indicated that infra-occluded deciduous second molars could be an early marker for other dental anomalies, such as palatally displaced canines and tooth agenesis, both known to have a strong genetic component.34
Ideally, waiting for exfoliation of the primary molar is the best treatment, as early extraction can lead to space loss in the arch, but not all infra-occluded molars exfoliate naturally. In a longitudinal study35 looking at both upper and lower infraoccluded molars, 149 were monitored, and five required extraction. It concluded that extraction should only be performed if there is deep infraocclusion, severe tipping of adjacent teeth and space loss has already occurred. Also recommended was using the time of exfoliation on the ‘normal’ side of the arch as a guide. In a separate study, where there was aplasia of the successor, the infra-occluded tooth did not exfoliate within the normal time range, and the root resorption was found to be very slow, especially after 12–13 years of age.36
Likely that primary molar will exfoliate naturally (extraction not usually necessary). But monitor and if below the contact point consider extraction, particularly if there is tipping of adjacent teeth.
NO and primary molar submerging
If only 1–2 mm below occlusal plane, monitor, consider occlusal build-up. If below the contact point consider extraction, particularly if there is tipping of adjacent teeth.
NO and no primary molar submergence
If good root length and unrestored, consider long-term maintenance. If poor long-term prognosis, consider extraction of primary molar, but seek orthodontic opinion first as it may not be possible to close resulting space fully.
Malocclusion due to non-nutritive sucking habits
The term ‘non-nutritive sucking habit’ (NNSH) encompasses the use of pacifiers (dummies/soothers), blankets and digit sucking. Children with a history of a persistent NNSH are more likely to develop a malocclusion compared to children with no NNSH history.37–40 In addition, there is evidence that the more prolonged the duration of the habit, the more severe the developing malocclusion tends to be.41–43 If these problems are not diagnosed until the patient is in the permanent dentition, it can be complex, time-consuming and costly to correct the problem and, in severe cases, it can even require orthognathic surgery to correct the anterior openbite. There are six RCTs reporting on a range of interventions44–49 for cessation of digit sucking. They show the following treatments to be successful:
Psychological treatment, in the form of positive reinforcement;
Aversive taste treatment, applied to the digit; and
The provision of a fixed habit-breaker appliance.
All 11 patients who received a fixed habit-breaker stopped sucking their thumb.
Recommendation
A fixed habit-breaker is the most effective treatment option for stopping persistent thumb-sucking habits where behaviour management techniques have been unsuccessful.
Centreline loss due to unilateral loss of primary teeth
The loss of the maxillary dental centreline can have aesthetic consequences, and work by Johnston et al has shown that lay people notice a maxillary centreline shift of 2 mm or more.50 It is difficult once in the permanent dentition to correct a centreline discrepancy, with often a unilateral extraction required to create space. It has been suggested that loss of centreline can be prevented by extraction of the contralateral primary canine, around the time of loss of the first primary canine.
The literature surrounding this topic is sparse. One paper reports that, out of approximately 200 children, 26 had a primary canine exfoliate due to the erupting lateral incisor.51 Centreline loss occurred in all of these patients, and 25 had a delayed balancing extraction of the remaining primary canine. Nine of the patients still had a centreline shift in adulthood.
One study has shown that centrelines in many unilateral extraction cases spontaneously correct.52 Another study showed that, in a non-extraction group of children, a centreline discrepancy was noted in 17% of them.53 A further study aimed to quantify the effect of unilateral extraction of primary molars on the position of the incisor centreline.54 The results showed that the degree of centreline shift was statistically significantly different between the balanced and unbalanced extraction groups, and also between the unbalanced and no extraction groups. This study supports the theory of balancing extractions, however, the evidence supporting balancing primary molar and canine extractions appears to be of poor quality.
Recommendation
If one primary canine is lost early (and the contralateral canine is firm), it is appropriate to extract the other to prevent the potential for centreline shift.
Increased overjet
Åltun et al reported that children with an increased overjet are more than twice as likely to have dental injuries than other children, with the incidence of traumatic dental injury highest among children aged six, and aged eight to ten years.55 Increased overjet and inadequate lip coverage increases the risk and severity of incisor trauma.56
A Cochrane review has been conducted with the aim being to assess the effectiveness of orthodontic treatment for prominent upper front teeth in two age groups; when the child is aged seven to nine, or when he/she is in early adolescence.57 The review identified and included eight trials. From the evidence, it would appear that providing early orthodontic treatment for children with prominent upper front teeth (a functional appliance), then providing the second phase of treatment (fixed appliances), when in the permanent dentition, is no more of an effective treatment than providing one course of orthodontic treatment when the child is in early adolescence (functional appliance followed by fixed appliances). One of the included studies showed that, at the start of the trial, 29.1% of the patients had already had some incisor trauma. During the trial, there was an increase in trauma in all three groups (a control group and two groups receiving functional appliances), but this was not significantly greater in the control group, for which treatment was delayed until the permanent dentition.
One circumstance which may encourage early intervention, for a patient with a large overjet, is when he/she is being teased. The literature has shown that early treatment with Twin block appliances resulted in an increase in self-confidence and a reduction of negative social experiences.58 Other studies have shown this link between increased overjet and teasing/low self-esteem.59,60 The literature supports the use of sports mouthguards for preventing trauma, particularly in patients with an increased overjet, and a detailed review of the literature61 also recommends custom-made mouthguards rather than shop bought ones.
Recommendation
Children with an increased overjet are at increased risk of dental trauma and should be provided with a custom-made sports mouthguard. Although orthodontic treatment can reduce the overjet, this is best started during early adolescence, unless the patient is being teased, where consideration should be given for early treatment.
Summary of recommendations
Having reviewed the often limited literature for the range of malocclusions where interceptive treatment is considered, it has been possible to make clinical recommendations. These are summarized in Table 3.
Condition
Recommended Treatment
Anterior crossbites
Modification to upper or lower incisor edges or’2 x 4’ fixed appliance
Posterior crossbites
URA with expansion screw or a quadhelix
Impacted upper central incisors
Maintain space for unerupted incisorFollow RCSEng Guidelines (Table 1)
Ectopic maxillary permanent canines
Consider space creation
Poor quality first permanent molars
Refer to RCSEng Guidelines and/or seek a specialist opinion
Infra-occluded primary molar teeth
Establish whether permanent successor presentFollow recommendations in Table 2
Non-nutritive sucking habits
Advise parents on the use of positive reinforcement techniques, and ‘paint’ for thumbIf unsuccessful, consider provision of a fixed habit-breaker appliance
Unilateral loss of primary canines
Extraction of remaining contralateral primary canine
Increased overjet and associated risk of trauma
Provide a custom-made mouthguard where necessary and refer patient to specialist once in permanent dentition If teasing occurring consider early referral