Fett N. Scleroderma: nomenclature, etiology, pathogenesis, prognosis, and treatments: facts and controversies. Clin Dermatol. 2012; 31:432-437
Kraus V, Lawson EF, Scheven EV Atypical cases of scleroderma En Coup de Sabre. J Child Neurol. 2012; 29:698-703
Pope E, Laxer RM. Diagnosis and management of morphea and lichen sclerosus and atrophicus in children. Pediatr Clin North Am. 2012; 61:309-319
Christen-Zaech S1, Hakim MD, Afsar FS, Paller AS. Pediatric morphea (localized scleroderma): review of 136 patients. J Am Acad Dermatol. 2012; 59:385-396
Pace C, Ward SE, Pace A. A rare case of frontal linear scleroderma (en coup de sabre) with intra-oral and dental involvement. Br Dent J. 2012; 208:249-250
Demir Y, Karaaslan T, Aktepe F, Yücel A, Demir S. Linear scleroderma “en coup de sabre” of the cheek. J Oral Maxillofac Surg. 2012; 61:1091-1094
El-Kehdy J, Abbas O, Rubeiz N. A review of Parry-Romberg syndrome. J Am Acad Dermatol. 2012; 67:769-784
Jun JH, Kim HY, Jung HJ Parry-Romberg syndrome with en coup de sabre. Ann Dermatol. 2012; 23:342-347
Scolozzi P, Herzog G. Total mandibular subapical osteotomy and Le Fort1 osteotomy using piezosurgery and computer aided designed and manufactured surgical splints: a favourable combination of three techniques in the management of severe mouth asymmetry in Parry-Romberg syndrome. J Oral Maxillofac Surg. 2012; 72:991-999
El-Kehdy J, Abbas O, Rubeiz N. A review of Parry-Romberg syndrome. J Am Acad Dermatol. 2012; 67:769-784
Pekiner FN, Yücelten D, Gümrü B, Sinanoğlu EA. Frontal linear scleroderma (en Coup de Sabre): a case report. J Dent Child (Chic). 2012; 73:175-178
O'Flynn S, Kinirons M. Parry-Romberg syndrome: a report of the dental findings in a child followed up for 9 years. Int J Paediatr Dent. 2012; 16:297-301
Fayad S, Steffensen B. Root resorptions in a patient with hemifacial atrophy. J Endod. 2012; 20:299-303
Kokich V. Orthodontic and nonorthodontic root resorption: their impact on clinical dental practice. J Dent Educ. 2012; 72:895-902
‘En coup de sabre’ or morphea, is a linear scleroderma that typically affects the frontoparietal region of patients resulting in a band-like scar that looks like a sword cut across the face. This case report describes a 13-year-old male patient with a history of ‘en coup de sabre’ referred to a dental department because of facial and dental involvement. To the authors' knowledge this has only previously been described on one occasion. The clinical presentation, clinical findings and a brief discussion of management, including the complicating effects of ‘en coup de sabre’ are discussed.
CPD/Clinical Relevance: By describing the facial and dental features of this rare condition to the dental community, the authors wish to increase awareness of the condition.
Article
The term scleroderma encompasses a rare group of fibrosing disorders that affect the skin and underlying tissues.1,2 In recent years, the classification of scleroderma has changed and the subtypes now described include localized scleroderma (or morphea), limited cutaneous systemic sclerosis, diffuse cutaneous systemic sclerosis and systemic sclerosis sine scleroderma.1 Localized scleroderma differs from systemic sclerosis in the absence of systemic involvement and is reported to have an incidence of 0.4 to 2.7 per 100,000 and is more commonly seen in females.1,2,3
‘En coup de sabre’ skin lesions are located in the head region and are characteristically fibrotic hyperpigmented plaques, like areas which are permanently hairless that resemble the stroke of a sword.2,3,4,5 These lesions can affect underlying bone, eye tissue and brain parenchyma, although rarely cross the midline.2,5 Lesions are benign in nature and typically start to develop at a young age in patients, progress over a number of years and then remain stationary into adult life.5 ‘En coup de sabre’ scleroderma mainly affects children, with over 90% of patients presenting aged between 2 and 14 years of age.2,3 Lesions are classically found in the frontoparietal region, involve the scalp and often can extend into ocular and nasal tissue in a vertical vector pattern.5
Studies have linked ‘en coup de sabre’ lesions to follow Blaschko lines, which may reflect the embryological migration of skin cells in certain characteristic patterns.4,6 Blaschko lines were thought to describe the distribution of certain skin conditions, such as epidermal naevus, sebaceous naevi, lichen striatus and linear lichen sclerosis.4,6
The aetiology and pathogenesis of ‘en coup de sabre’ is not entirely understood, although it is believed that it involves a complex association between autoimmunity and environmental factors (eg trauma and infection) that lead ultimately to the synthesis and deposition of excess collagen in skin and underlying tissue.3,4
Parry-Romberg syndrome, a rare degenerative condition characterized by the development of hemifacial atrophy of the skin, soft tissues and underlying bone structure, has been linked to ‘en coup de sabre’.5,7,8 Both conditions have similar clinicopathological features, although the debate remains as to whether they remain as two separate entities. It has also been said that linear scleroderma may act as a precursor in the development of Parry-Romberg syndrome, which may develop after several years.7,8
The diagnosis of ‘en coup de sabre’ is based on the clinical history and typical appearance of skin findings seen in patients.2 Laboratory investigations and imaging findings are non-specific.2 Imaging modalities, such as Magnetic Resonance Imaging (MRI), can provide further information in patients presenting with neurological symptoms.2
There remains no definitive treatment for ‘en coup de sabre’ largely due to the rarity of the condition and a lack of evidence of outcome measures for individual therapies for localized scleroderma.1,3,5 Topical therapies for localized plaques of morphea include corticosteroids, vitamin D3 analogues and tacrolimus.3 Local phototherapy (UVA and UVB) has also been described for treatment of superficial lesions.3 Systemic treatment with the use of medicaments such as corticosteroids or methotrexate are indicated for lesions with the potential for functional or cosmetic disfigurement.3 Treatment with these regimens can last several years and overall success rates remain low.3,5 The resulting facial deformity in these patients can often require corrective surgery.3,9 Targeted augmentation of defects has been directed to treat the soft tissue deficit on the affected side, although extensive craniofacial and orthognathic procedures have reportedly been used for surgical correction of skeletal discrepancies, particularly in cases of hemifacial atrophy/Parry-Romberg syndrome.9 Due to their asymptomatic nature, there is often a delay in seeking medical expertise for ‘en coup de sabre’ lesions, resulting in a delay in diagnosis and treatment for patients.3 The atypical presentation of ‘en coup de sabre’ can also result in patients attending various medical departments in the search for formal diagnosis, again resulting in delay of treatment.2
Case report
A 13-year-old male patient was referred from specialist practice to the dental hospital with a Class 1 malocclusion complicated by isolated shortening of the root to an upper right lateral incisor.
Extra-oral
The patient presented with a mild Class 2 skeletal relationship due to mandibular retrognathia (Figure 1). There was no gross vertical discrepancy but there was a mild facial asymmetry with the chin point off to the right-hand side.
The main extra-oral feature was an interrupted linear soft tissue defect running from the patient's forehead through the lateral aspect of the nose and the upper lip (Figure 2). This defect appeared to be mildly oblique and there was a suggestion of it affecting the right mental region.
Figure 2. Pre-treatment extra-oral anterior view of patient showing an interrupted linear soft tissue defect running from the patient's forehead through the lateral aspect of the nose and the upper lip.
Intra-oral
The patient presented with an essentially Class 1 incisor relationship (Figure 3) with the overjet found to be within average limits (3 mm). The overbite was slighty increased but complete with the lower incisor tips just occluding with the cingulum plateau of the upper incisors. The molar relationship was Class I bilaterally and both the upper and lower dental centre lines were off to the patients' right-hand side. The upper and lower incisors appeared slightly upright.
Figure 3. Pre-treatment intra-oral anterior view of the Class 1 malocclusion with anterior crossbite and mild centreline discrepancies.
The upper right lateral incisor was palatally positioned with the history of a recent exfoliation of a retained upper right deciduous lateral incisor. The upper and lower right canines were both distally angulated and the incisal edge of the upper right central incisor was positioned 2 mm above to the contralateral central incisor.
Radiographic findings
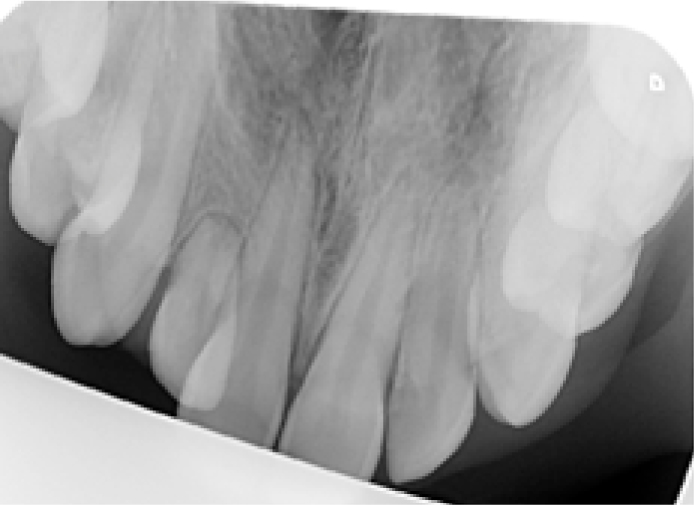
A panoramic radiograph (Figure 4) indicated that the upper right lateral incisor had an abnormally shortened root (approximately a third of the length of the contra-lateral tooth). This finding was confirmed by a maxillary occlusal radiograph (Figure 5). The lower right canine root also appeared shortened but this was less dramatic, being approximately two-thirds the length of the lower left canine
Figure 4. Pre-treatment panoramic radiograph showing shortened roots of UR2 and LR3.Figure 5. Pre-treatment maxillary occlusal radiograph confirming significant shortening of UR2 root.
Management
A detailed history taken confirmed that the patient was under the care of dermatology. Communication between specialties confirmed that the patient had been diagnosed with morphea (‘en coup de sabre’) and was being monitored with no active treatment recommended.
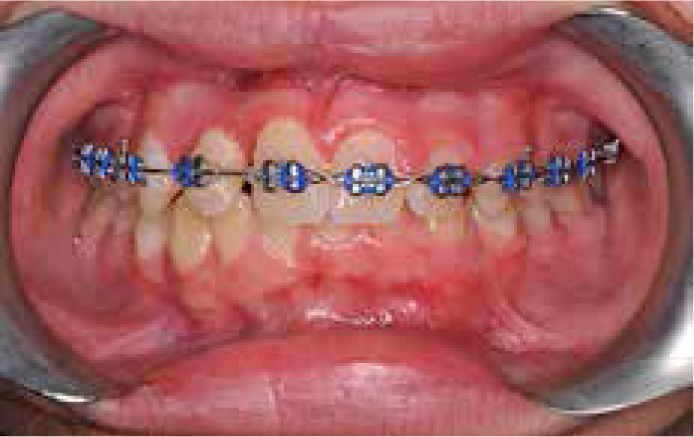
After a joint consultation with restorative colleagues, orthodontic treatment was commenced and the patient and his parents were warned of the risk of loss of the upper right lateral incisor due to further root shortening during tooth movement. Fixed appliance treatment was carried out with an upper fixed appliance initially and disclusion was provided to eliminate the anterior crossbite (Figure 6). This diagnosed a mild mandibular asymmetry and a lower incisor extraction was prescribed to enable transverse dento-alveolar camouflage. Treatment progressed routinely with no atypical resorption of the upper right lateral incisor seen at 6 months into treatment (Figure 7). An upper bonded retainer was placed at debond (Figure 8) because of the unfavourable crown-root ratio of the upper right lateral incisor. An acceptable occlusal result was achieved (Figures 9 and 10).
Figure 6. Mid-treatment intra-oral anterior view showing persistence of lower centreline discrepancy following elimination of anterior crossbite.Figure 7. Mid-treatment intra-oral periapical radiograph of the upper right lateral suggesting no gross orthodontic induced root resorption.Figure 8. Bonded retainer placed at debond.Figure 9. Post-treatment intra-oral anterior view.Figure 10. Post-treatment extra-oral anterior view.
Discussion
‘En coup de sabre’, as described in this clinical case, is a form of linear scleroderma.2 Linear scleroderma is a subtype of localized scleroderma in which collagen is excessively deposited in areas of skin, muscle and underlying tissue.2
Orthodontic assessment of this patient revealed a mild mandibular asymmetry that, after elimination of the anterior crossbite, was diagnosed as a skeletal discrepancy and not a functional displacement. It has to be questioned whether the mild mandibular asymmetry is related to the known ‘en coup de sabre’ diagnosis. The panoramic radiograph seems to show no gross condylar head changes or significant asymmetrical mandibular morphology. The presence of maxillary and mandibular deformities have been documented in patients affected by hemifacial atrophy/Parry-Romberg syndrome.10
Dental involvement of ‘en coup de sabre’ scleroderma is limited.5,11,12 Evidence of documented shortened roots has been published previously, although specifically related to cases of known hemifacial atrophy.13 In this case, the development of the root of the upper right lateral incisor tooth appears to have been restricted to approximately one third the normal length on radiographic assessment. Interestingly, there does not appear to be any significant bone loss around the tooth. If the altered root development in the upper right lateral and lower right canine are due to the scleroderma, then they are not chronologically matched with the lower canine affected later in the patient's dental development. This could be explained by the possibility that this linear defect progresses slowly along the line of the defect. It will be interesting to monitor the mild skin deformity in the right mental region to see if this becomes more obvious with time. Alternatively, what may have happened is idiopathic resorption of roots that previously developed to a normal length.
In contrast to a previous study,6 in this case, although the scar can clearly be seen to affect the right nasal alar, there does not appear to be extension into the oral mucosa or attached mucosa adjacent to the upper right lateral incisor tooth. It remains unclear as to the true underlying aetiology of the shortened roots, but with no history of significant dental trauma or previous orthodontic treatment, it could be related to the known ‘en coup de sabre’ diagnosis.
Summary
This case report describes the presentation of the relatively rare condition of ‘en coup de sabre’ and asks the question of whether dental and/or skeletal development can be affected by this condition. Our structured review of the literature suggests that the management of this condition is varied, but future studies may indicate that early intervention is beneficial to these patients and so their onward referral to a Consultant Dermatologist should not be delayed.
The patient described in this case report benefited from assessment in the multidisciplinary dental setting, followed by careful treatment by a consultant-led orthodontic service. Shortened roots may be retained and remain functional for decades,14 but future complex restorative dentistry remains a possibility. We propose that the early onset of the condition and its unpredictable progressive pathogenesis indicate it should be referred for a multidisciplinary team assessment. The possibility of an associated significant facial deformity, as well as dental anomalies, mean that patients affected by ‘en coup de sabre’ could benefit from treatment by specialist paediatric dental, restorative, orthodontic and maxillofacial clinicians.