Pazianas M, Miller P, Blumentals WA, Bernal M, Kothawala P. A review of the literature on osteonecrosis of the jaw in patients with osteoporosis treated with oral bisphosphonates: prevalence, risk factors, and clinical characteristics. Clin Ther. 2007; 29:1548-1558
Ruggiero SL, Dodson TB, Fantasia J, Goodday R, Aghaloo T, Mehrotra B, O'Ryan F. American Association of Oral and Maxillofacial Surgeons Position Paper on Medication-Related Osteonecrosis of the Jaw – 2014 Update. J Oral Maxillofac Surg. 2014; 72:1938-1956
Chrcanovic BR, Reher P, Sousa AA, Harris M. Osteoradionecrosis of the jaws – a current overview – part 1: Physiopathology and risk and predisposing factors. Oral Maxillofac Surg. 2010; 14:3-16
Patel V, Kelleher M, Sproat C, Kwok J, McGurk M. New cancer therapies and jaw necrosis. Br Dent J. 2015; 219:203-207
Haria S, Patel V, Sproat C, Kwok J, Ormondroyd L, McGurk M, Burke M, Reilly D, Lyons A, Cascarini L, Townley W. Is osteoradionecrosis evolving with improved radiotherapy delivery system?. J Oral Maxillofac Surg. 2016; 74
Crossman T, Herold J. Actinomycosis of the maxilla – a case report of a rare oral infection presenting in general dental practice. Br Dent J. 2009; 206:201-202
Gupta S, Sreenivasan V, Patil PB. Dental complications of herpes zoster: two case reports and review of literature. Indian J Dent Res. 2015; 26:214-219
Pogrel MA, Miller CE. A case of maxillary necrosis. J Oral Maxillofac Surg. 2003; 61:489-493
Lanigan DT, Hey JH, West RA. Aseptic necrosis following maxillary osteotomies: report of 36 cases. J Oral Maxillofac Surg. 1990; 48:142-156
Khan N, Memon W, Idris M, Ahmed M, Taufiq M. Post-traumatic near-complete aseptic necrosis of the maxilla: a case report and review of the literature. Dentomaxillofac Radiol. 2012; 41:429-431
Nguyen EV, Heggie AAC. Avascular necrosis of the midface secondary to disseminated intravascular coagulation. Int J Oral Maxillofac Surg. 2014; 43:1441-1444
Borle RM, Prasant MC, Badjate SJ, Patel IA. Sickle cell osteomyelitis of the maxilla: a case report. J Oral Maxillofac Surg. 2001; 59:1371-1373
Poghosyan YM, Hakobyan KA, Poghosyan AY, Avetisyan EK. Surgical treatment of jaw osteonecrosis in “Krokodil” drug addicted patients. J Craniomaxillofac Surg. 2014; 42:1639-1643
Alsufyani NA, Lam EW. Osseous (cemento-osseous) dysplasia of the jaws: clinical and radiographic analysis. J Can Dent Assoc. 2011; 77
Fenerty S, Shaw W, Verma R, Syed AB, Kuklani R, Yang J, Ali S. Florid cemento-osseous dysplasia: review of an uncommon fibro-osseous lesion of the jaw with important clinical implications. Skel Radiol. 2017; 46:581-590
Singer SR, Mupparapu M, Rnaggio J. Florid cementoosseous dysplasia and chronic diffuse osteomyelitis. Report of a simultaneous presentation and review of the literature. J Am Dent Assoc. 2005; 136:927-931
Barnes L, Eveson JW, Reichart P, Sidransky D. World Health Organization Classification of Tumours. Pathology and Genetics Head and Neck Tumours.Lyon: IARC Press; 2005
MacDonald-Jankowski DS. Fibro-osseous lesions of the face and jaws. Clin Radiol. 2004; 59:11-25
Kawai T, Hiranuma H, Kishino M, Jikko A, Sakuda M. Cemento-osseous dysplasia of the jaws in 54 Japanese patients. A radiographic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 87:107-114
MacDonald-Jankowski DS. Florid cemento-osseous dysplasia: a systematic review. Dentomaxillofac Radiol. 2003; 32:141-149
Hochberg MC. Racial differences in bone strength. Trans Am Clin Climatol Assoc. 118:305-315
Chen L, Li T, Jing W, Tang W, Tian W, Li C, Liu L. Risk factors of recurrence and life threatening complications for patients hospitalized with chronic suppurative osteomyelitis of the jaw. BMC Infect Dis. 2013; 13:1-8
Almazrooa SA, Woo S. Bisphosphonate and nonbisphosphonate-associated osteonecrosis of the jaw: A review. J Am Dent Assoc. 2009; 140:864-875
Weldon D. The effects of corticosteroids on bone: osteonecrosis (avascular necrosis of the bone). Ann Allergy Asthma Immunol. 2009; 103:91-97
Patel V, McGurk M. Use of pentoxifylline and tocopherol in radiation-induced fibrosis and fibroatrophy. Br J Oral Maxillofac Surg. 2017; 55:235-241
Henien M, Patel V, Sproat C, McGurk M. Spontaneous osteonecrosis of the maxilla. Dent Update. 2016; 43:563-566
Allen MR, Burr DB. The pathogenesis of bisphosphonate-related osteonecrosis of the jaw: so many hypotheses, so few data. J Oral Maxillofac Surg. 2009; 67:61-70
Toffanin A, Benetti R, Manconi R. Familial florid cemento-osseous dysplasia: a case report. J Oral Maxillofac Surg. 2000; 58
Wray L. The diabetic patient and dental treatment: an update. Br Dent J. 2011; 5:209-215
Khamaisi M, Regev E, Yarom N, Avni B, Leitersdorf E, Raz I, Elad S. Possible association between diabetes and bisphosphonate-related jaw osteonecrosis. J Clin Endocrinol Metab. 2007; 92:1172-1175
Kajizono M, Sada H, Sugiura Y, Soga Y, Kitamura Y, Matsuoka J, Sendo T. Incidence and risk factors of osteonecrosis of the jaw in advanced cancer patients after treatment with zoledronic acid or denosumab: a retrospective cohort study. Biol Pharmaceut Bull. 2015; 38:1850-1855
Manfredi M, Mergoni G, Goldoni M, Salvagni S, Merigo E, Meleti M, Vescovi P. A 5-year retrospective longitudinal study on the incidence and the risk factors of osteonecrosis of the jaws in patients treated with zoledronic acid for bone metastases from solid tumors. Med Oral Patol Oral Cir Bucal. 2017; 22:e342-e348
Abstract: Osteonecrosis of the jaw (ONJ) is most commonly related to medications such as anti-resorptives and anti-angiogenics or head and neck radiotherapy. However, in addition to these, alternative causes of ONJ have also been reported including; infection, chemical toxicity, trauma and vascular ischaemia, but this list is not exhaustive.
It is well accepted that cemento-osseous dysplasia (COD) can increase the risk of infection, poor healing and osteomyelitis due to the reduced vascularity. However, necrotic and exposed COD has not been widely reported. This case report describes a patient with COD-related necrosis in the anterior mandible and hence provides an additional member to the ever growing list of potential predisposing factors for jaw necrosis
CPD/Clinical Relevance: Cemento-osseous dysplasia is a well recognized and benign condition commonly diagnosed from radiographs. The condition carries an increased risk of osteomyelitis and slow healing following oral surgery and, at its extreme, can cause osteonecrosis of the jaw, which remains an important condition of which the general dental practitioner (GDP) should be aware.
Article
Osteonecrosis of the jaw (ONJ) is identified as ‘non-healing exposed necrotic bone in the maxillofacial region’.1 This broad definition has been expanded with specific detail for the two most common causes of ONJ; medication-related osteonecrosis of the jaw (MRONJ)2 and osteoradionecrosis (ORN).3 Specifically, MRONJ is defined as exposed bone or bone which can be probed through an intra- or extra-oral fistula in the maxilla or mandible, persisting for more than 8 weeks, having previous treatment with anti-resorptive or anti-angiogenic medications and without a history of radiotherapy or metastatic disease.2 In contrast, there remains no agreed definition for ORN but a theme amongst the many definitions proposed is the requirement of exposed, necrotic jaw bone in patients who have undergone head and neck radiotherapy.3 The exact duration required for the bone to be exposed to be deemed ORN remains under debate.
The drugs contributing to MRONJ includes bisphosphonates, denosumab, bevacizumab, sunitinib, sofarenib, cabozantanib, aflibercept, everolimus and radium 223, with the likelihood that future novel biologics will continue to populate this list.4 With so many drugs already implicated in MRONJ, with the prediction of more in the future, it remains no surprise to see why MRONJ is on the rise. A rise in ORN has also been seen, even with the introduction of new and advanced radiation delivery systems, with suggested causes related to increasing incidence of oropharyngeal tumours and increasing use of chemo-radiotherapy.5
Apart from MRONJ and ORN, a number of other causes of ONJ have been reported. These include infection (bacterial6, viral7 and fungal8), trauma (iatrogenic9 and traumatic injury10), acquired,11 congenital medical disorders12 and narcotic use.13
From the various identified causes of ONJ, cement-osseous dysplasia (COD) has not been routinely reported or hypothesized as a cause in the literature. Cemento-osseous dysplasia is accepted to carry an increased incidence of osteomyelitis, infection and delayed or poor wound healing.14,15,16 Even though osteomyelitis and ONJ can share some similarities, there are clear differences between them with regards to definition and pathophysiology, making them individual and distinct entities. The current report describes a case of ONJ in an area of COD.
Case report
A 68-year-old female patient of Arabic descent had been referred by her GDP regarding an area of exposed bone in the mandible. She attended the Oral Surgery department in February 2017 with a one-year history of exposed hard mass in the lower anterior region. She reported experiencing pain followed by self-exfoliation of her lower front tooth and subsequent recession of the soft tissue in the region, exposing the adjacent tooth and surrounding bone. Since its occurrence she reported no further pain or symptoms to date.
Her medical history revealed well controlled type two diabetes mellitus, low blood pressure and anaemia. She also reported a penicillin allergy. Her medication included metformin, folic acid and vitamin B. There was no history of anti-resorptive or anti-angiogenic medication use currently or in the past.
Extra-oral examination was unremarkable. Intra-oral examination revealed a hard tissue mass in the anterior mandible that was highly suggestive of exposed bone. The area extended from the right mandibular lateral incisor (LR2) to the mesial aspect of the left mandibular canine (LL3) (Figure 1). The exposed tissue was covered in plaque and the surrounding soft tissues showed no signs of inflammation or infection. The teeth within the exposed hard tissue were restored and non-mobile.
Figure 1. A bony dehiscence on the labial aspect of the oral mucosa between LR2 and LL3.
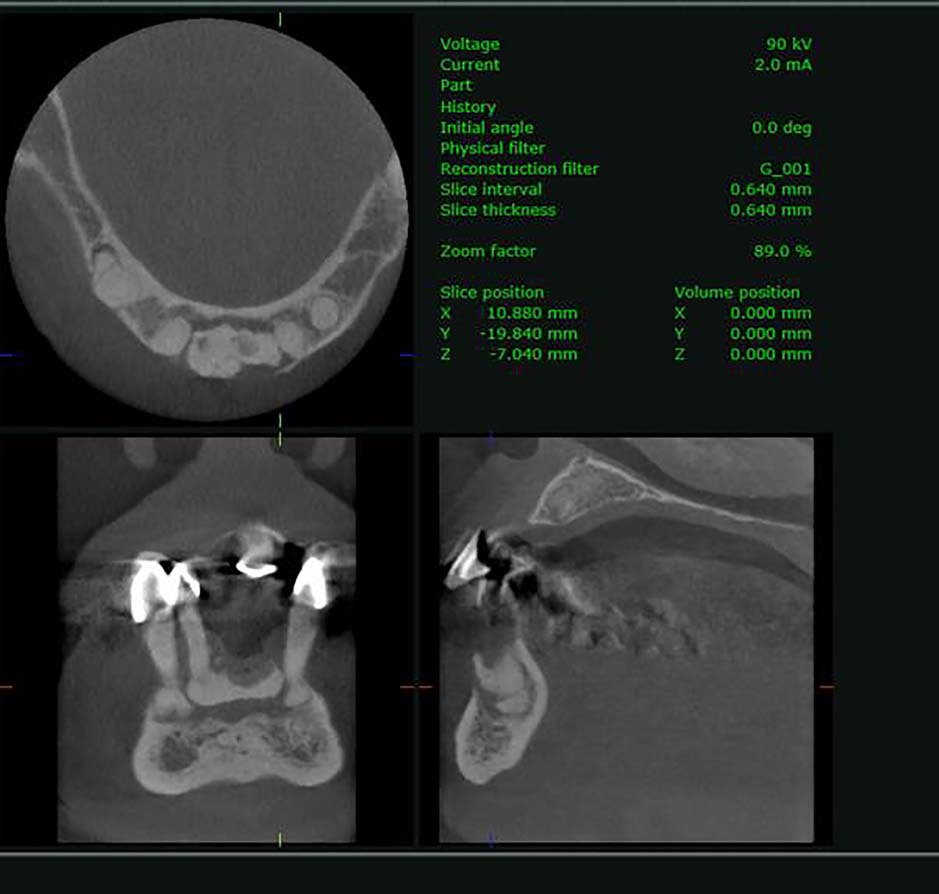
A dental panoramic tomograph (DPT) revealed a radio-opaque mass with well-defined margins in the anterior incisor region. This area appeared to have a circumferential radiolucency surrounding it. The apical third of the LR2 was located within the radio-opaque mass and appeared to fuse with it, making it indistinct. Further mixed radio-opacity with radiolucent halos were present at the apical portion of all the remaining mandibular teeth (Figure 2). A small volume cone beam computerized tomograph (CBCT) of the anterior mandible confirmed the presence of irregular radio-opacity surrounded by a zone of radiolucency suggestive of COD. The CBCT also showed the socket of the left mandibular lateral incisor, which remained completely unhealed. Furthermore, the imaging confirmed the area was sequestrating from the mandible and included the LR2 within the exfoliating segment (Figure 3). There appeared to be no periosteal reaction or thickening, as commonly seen in osteomyelitis. Blood assays (full blood count, liver function test, CRP, ESR, glucose and bone profile) did not show any secondary cause for the exposed and necrotic COD.
Figure 2. DPT revealing radio-opacities located in the mandibular central incisor region and periapical to LR5, LR3, LR2, LL2 and the lower left last standing molar. The radio-opacity anteriorly is surrounded by a radiolucent zone.Figure 3. CBCT imaging of the anterior mandible. The coronal plane view suggests that the bone in the anterior region of the mandible has sequestrated and includes LR2 within the segment. The sagittal and transverse plane views indicate loss of the labial cortical bone adjacent to the osseous lesion.
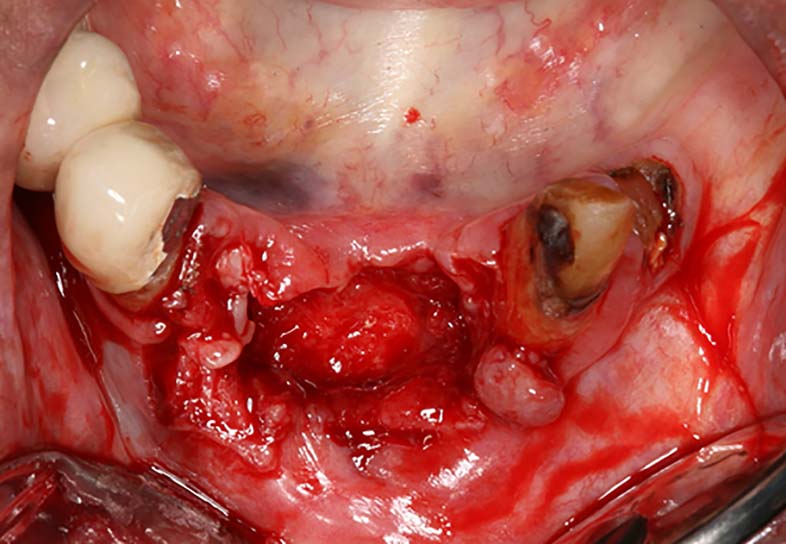
The patient was keen for surgical intervention and the treatment was performed under local anaesthesia (lignocaine 2%, 1:80,000 adrenaline) where the sequestrating exposed bone was elevated intact, including LR2 (Figure 4) revealing a fully granulated mucosal base (Figure 5) with no further exposed bone evident. Soft tissue closure was achieved with 4−0 resorbable sutures. Both the bone and tooth tissue samples were sent for histopathological analysis (Figure 6). Histopathology results indicated the bone in the lower incisor region to be non-vital dense cemento-osseous mineralized tissue. The marrow space contained bacterial plaque. The tooth tissue present in the biopsy showed hypercementosis and a necrotic pulp. The definitive histopathological diagnosis was consistent with a large mandibular necrotic sequestrum arising in COD.
Figure 4. The hard mass removed with LR2 anchored within the lesion immediately post surgery.Figure 5. The site immediately post–sequestration removal showing evidence of granulation at the base and lateral margins with no evidence of exposed bone.Figure 6. Histological features of the sequestered mass. (a) Whole mount view of a representative serial slice demonstrating a fused mass of sclerotic non-vital cemento-osseous tissue. (b) Medium power view of an area demonstrating fused round to ovoid zones of mineralization and empty lacunae. (c) Medium power view of degenerate soft tissue space occupied by mixed bacterial flora (black arrow) and adjacent infiltrate of neutrophils (yellow arrow); formic acid decalcification, haematoxylin and eosin, scale bars = 200 μm).
At review one-month post-surgery, the site had maintained full mucosal coverage and the patient reported no symptoms. Unfortunately, the patient failed to attend for subsequent review appointments.
Discussion
Fibro-osseous lesions encompass a large array of benign conditions in which, histopathologically, there is a continual process by which the normal bone is replaced by a mixed form of fibrous and osseous tissue.17 Cemento-osseous dysplasia is one such condition, classed under the fibro-osseous group and compared to fibrous dysplasia and fibro-osseous neoplasms, which is limited to the dento-alveolar segments of the jaw. Cemento-osseous dysplasia lesions are diagnosed by radiographic presentation and their extent results in sub-categorization via prefix terms. Periapical COD commonly occurs in the anterior mandible and may present as localized radiolucencies, opacities, or a mixture of the two. Their presence around the periradicular region is often confused for infective or inflammatory cysts, however, vitality testing of the involved teeth proves their normal pulpal status and response. Focal COD is commonly seen in the posterior region and limited to only a few teeth. It often has a mixed radiolucent and opaque pattern with it being a sole and isolated lesion in the patient's jaw. The florid type of COD is of much more extensive form and manifests as large radio-opacities over various sites and possibly in both jaws simultaneously.
The pathogenesis of COD is currently unknown and there are conflicting theories that it may originate from the periodontal ligament, based on its close proximity and shared histopathologic features,15 however, Kawai et al showed normal periodontal ligament spaces in patients with COD, suggesting that these lesions could be of medullary bone origin19 with bone modelling defects as well as hypercementosis.15
Demographically, the Afro-Caribbean population have the highest incidence of COD (59%), followed by Orientals (37%) then Caucasians (3%).20 Afro-Caribbeans have higher bone mineral density compared to Caucasians and the rate of decline in bone mineral density is also lower.21 Interestingly, a female predominance has been shown, which may suggest that sex-linked factors play a part in the aetiology.18,20 Asymptomatic lesions do not require treatment, however, monitoring of the areas with routine radiographs is advised to assess for significant change or associated complications such as osteomyelitis.15 There is no agreed consensus. The general approach is that surgical intervention should be avoided except in infected cases.15
Osteomyelitis is broadly defined as an inflammatory condition of the bone, which begins as an infection of the medullary cavity, rapidly involving the haversian systems, and extends to involve the periosteum of the affected area.22 Sustained infection leads to involvement of the cortex, periosteum and soft tissue.23 Cemento-osseous dysplasia is recognized as a predisposing factor to the development of chronic osteomyelitis,24 with the pathophysiology largely due to compromised vascularity.16 Alsufyani and Lam conducted a study of 118 patients with COD where clinical and radiographic assessment revealed 11% of patients to have osteomyelitis, suggesting that the complication is common in this cohort of patients.14
Compromised vasculature or avascular necrosis leading to eventual bony infarction and subsequent death is a major factor in the development of ONJ.2,25 This theme is common to MRONJ and ORN through the anti-angiogenic effects of drugs4 and radiation-induced fibrosis,26 respectively. The vascularity theory is believed to be a plausible reason why ONJ has a higher incidence in the mandible compared to the maxilla. However, even with the rich blood supply in the maxilla, it remains vulnerable to spontaneous necrosis in the absence of causative medications and radiotherapy, as highlighted by Henien et al27 in a case report where the cause was suggested to be idiopathic vascular ischemia, diagnosed by exclusion.27 The idea of vascular ischaemia causing necrosis supports this hypothesis that the reduced vascularity in the COD lesion potentially leads to ONJ in the current case. Other hypotheses emphasize the role of infections, altered fat metabolism and toxic damage of the soft tissue.28
Historically, there has not always been a clear distinction between osteomyelitis and osteonecrosis, with the literature freely switching between terms incorrectly. More recently, this distinction has been defined and highlighted due to the rise of ONJ, and the two conditions have different definitions and criteria for diagnosis as well as management. Cemento-osseous dysplasia and osteomyelitis have been synonymous with one another, however, exposure and necrosis of COD and the surrounding bone appear to be less well known to date. There have not been reliable evidence or reports to suggest that COD has a link with ONJ. A case report which illustrated and discussed florid COD in a particular family reports that one of the members had been admitted to hospital due to ‘inflammatory and osteonecrotic processes that occurred after teeth extraction’.29 This was interpreted from the patient's medical records only and does not confirm exposed and necrotic bone, with the diagnosis appearing more in line with osteomyelitis.
Diabetes mellitus is recognized as a potential co-factor for delayed or poor healing,30 as well as an increased risk of infection.23 Furthermore, this vulnerability of infection again predisposes diabetic patients to potentially develop osteomyelitis under the immunocompromised category, however, in reality this is rarely seen. The role of diabetes in ONJ is well recognized as a co-factor. A study by Khamaisi et al reported 18/31 (58%) patients with MRONJ had diabetes or impaired fasting glucose.31 The link between diabetes and periodontal disease is also well established. Periodontal disease alone has also been considered to be a predisposing factor in ONJ. In MRONJ, periodic dentistry maintenance was found to lower the risk of MRONJ significantly,32,33 suggesting that poor oral hygiene in patients receiving anti-resorptive medications can increase the risk of MRONJ. In the current case, the patient had both periodontal disease and diabetes and the likelihood is that these factors compounded her risk of eventual necrosis and exposed COD.
In this case, it was proposed that COD-related osteonecrosis of the jaw, in a similar fashion to many other types of ONJ, has the ability to sequestrate. The advantage of delaying surgery appears to allow a slow process of sequestration to occur, with granulation under the affected area leaving no exposed bone leading to immediate resolution.
Conclusion
The case presented suggests that COD as another potential predisposing factor of ONJ. The additional risk factors of diabetes, poor oral hygiene and the reduced vascularity of the COD lesion may have increased the risk of the ONJ occurring in this case.