Helmi N, Bashir M, Shireen A, Ahmed IM. Thalassemia review: features, dental considerations and management. Electron Physician. 2017; 9:4003-4008 https://doi.org/10.19082/4003
Clevenger B, Kelleher A. Hazards of blood transfusion in adults and children. Cont Educ Anaesth Crit Care Pain. 2014; 14:112-118
Beck W.Cambridge, MA: MIT; 1998
Habibian N, Alipour A, Rezaianzadeh A. Association between iron deficiency anemia and febrile convulsion in 3-to 60-month-old children: a systematic review and meta-analysis. Iran J Med Sci. 2014; 39:496-505
Jankulovski N, Antovic S, Kuzmanovska B, Mitevski A. Splenectomy for haematological disorders. Pril (Makedon Akad Nauk Umet Odd Med Nauki). 2014; 35:181-187
Dave M, Loughlin A, Walker E, Davies J. Challenges in plain film radiographic diagnosis for the dental team: a review of the maxillary sinus. Br Dent J. 2020; 228:587-594 https://doi.org/10.1038/s41415-020-1524-8
Baldini M, Marcon A, Cassin R Beta-thalassaemia intermedia: evaluation of endocrine and bone complications. Biomed Res Int. 2014; 2014 https://doi.org/10.1155/2014/174581
Rossi F, Perrotta S, Bellini G Iron overload causes osteoporosis in thalassemia major patients through interaction with transient receptor potential vanilloid type 1 (TRPV1) channels. Haematologica. 2014; 99:1876-1884 https://doi.org/10.3324/haematol.2014.104463
De Sanctis V, Soliman AT, Elsedfy H Osteoporosis in thalassemia major: an update and the I-CET 2013 recommendations for surveillance and treatment. Pediatr Endocrinol Rev. 2013; 11:167-180
The craniofacial manifestations of beta thalassaemia are widely reported, and occur as a result of inadequate haematopoiesis leading to marrow space expansion. Secondarily, extramedullary haematopoiesis can occur throughout the body, although this is rarely reported in the paranasal sinuses. We discuss the systemic and craniofacial manifestations of beta thalassaemia major, with a focus on the radiological findings, as illustrated in a case of a 55-year-old male patient who was referred to the dental hospital as a result of complications of thalassaemia. This case report focuses on the effects of thalassaemia that may be encountered in a dental setting and highlights the radiological findings that clinicians should be aware of.
CPD/Clinical Relevance: Dental and craniofacial manifestations, and their management, are discussed for patients with beta thalassaemia.
Article
Thalassaemia is a genetic disorder involving abnormal haemoglobin formation.1 The haemoglobin molecule consists of both alpha and beta chains. In thalassaemia, the alpha or beta chains in the haemoglobin are defective as a result of mutation in the alpha or beta globin genes, resulting in a reduced oxygen-carrying capacity of the blood. This leads to overproduction of red blood cells and abnormal haemoglobin in the body. Thalassaemia can be described as either alpha or beta thalassaemia depending on which chains of the haemoglobin molecule are affected.2
There are several subtypes of the disease, including the minor, intermediate and major forms, which all present with varying severity. Beta thalassaemia is mainly found in Mediterranean, African and Asian populations.
Thalassaemias are a quantitative problem of haemoglobin synthesis where not enough ‘normal’ haemoglobin is produced to cope with the oxygenation demands of the body (ineffective erythropoiesis). In beta thalassaemias, there is also haemolysis of the defective circulating red blood cells. These phenomena together result in severe anaemia. The body may compensate for reduced oxygen carrying capacity through hyperplasia of bone marrow. Individuals with thalassaemia major often require regular blood transfusions to counteract the chronic anaemia that accompanies the disease.2
We present the case of a patient exhibiting marked craniofacial manifestations of beta thalassaemia major, illustrated with radiological imaging. In this case, the effects can be clearly seen on dental panoramic radiographs, as well as computed tomography imaging.
Case report
A 55-year-old Iranian male patient was diagnosed with transfusion-dependent beta thalassaemia during his childhood in Iran. He was subsequently treated in the UK, where he was referred to the dental hospital by his haematology team, with suspicion of osteomyelitis and bony expansion in the jaw. The patient complained of pain on eating and speaking while wearing his upper denture, which had been constructed 5 years previously in Iran.
He had also been seen by ENT, as he complained of chronic, left-sided facial pain. This had been investigated historically with plain imaging and the patient had undergone a Caldwell-Luc procedure in Iran to investigate an opacified sinus where chronic sinus disease was suspected. The cause of the opacified sinus was later found to be thalassaemia-related on three-dimensional imaging carried out in the UK following the procedure, which had caused ongoing symptoms since it had been carried out.
He reported having multiple facial reconstructive surgeries in Iran as a child to correct facial deformities resulting from his history of beta thalassaemia.
Medically, the patient had transfusion-dependent beta thalassaemia major, with sequelae including an enlarged heart, shortness of breath and anaemia. He was taking iron chelation therapy, to reduce the level of iron in his blood, which was high as a result of regular blood transfusions. He developed osteoporosis as a complication of the thalassaemia, and had a severe pathological fracture as a child. He had been taking anti-resorptive medications since 1990, which included weekly oral bisphosphonates until 2015, and annual denosumab injections from 2018 onwards prescribed by his rheumatology team. He had well-controlled type II diabetes mellitus. Socially, the patient had never smoked or chewed tobacco, and drank no alcohol.
On examination, he presented with a suppurating fistula in the upper left premolar region and he had an enlarged maxillary alveolar ridge. This area was consistent with medication-related osteonecrosis of the jaw (MRONJ).
From a dental perspective, the patient was treatment planned for provision of upper dentures, and conservative management of the localized MRONJ in the upper left quadrant, which included regular irrigation of the area with chlorhexidine mouthwash.
Imaging
The patient had interval CT scans of the paranasal sinuses and facial bones carried out, as well as a dental panoramic tomograph for investigation of sinus pathology and the source of facial pain (Figures 1–5)
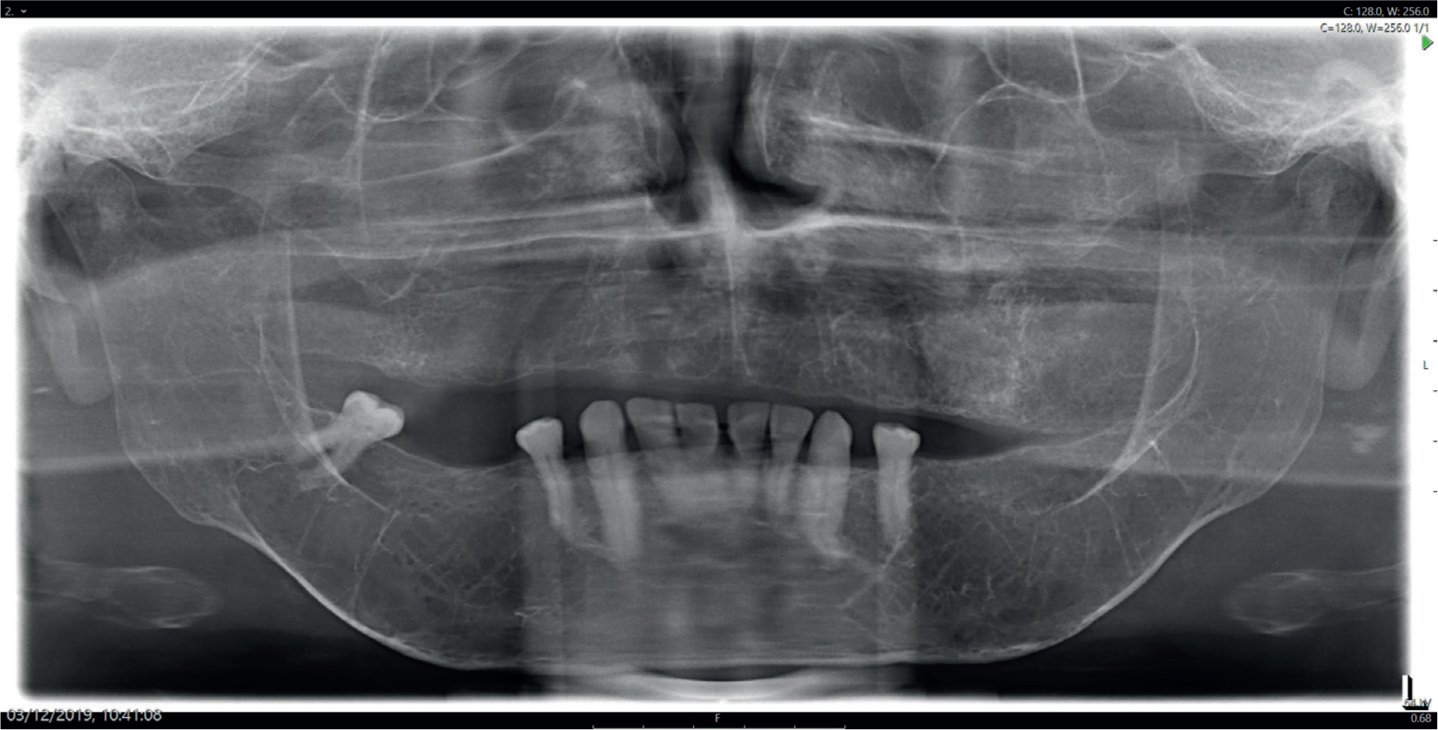
Figure 1. A dental panoramic radiograph showing a generalized osteopenic appearance of the visualized facial bones. There was significant thinning of the bony cortices making it difficult to trace the outline of the ID canal bilaterally, and the maxillary sinus floor was not detectable. The lamina dura surrounding the remaining teeth was not identifiable and the inferior cortex of the mandible was markedly thinned. Where the air space of the maxillary sinuses is expected, there was opacification.Figure 2.
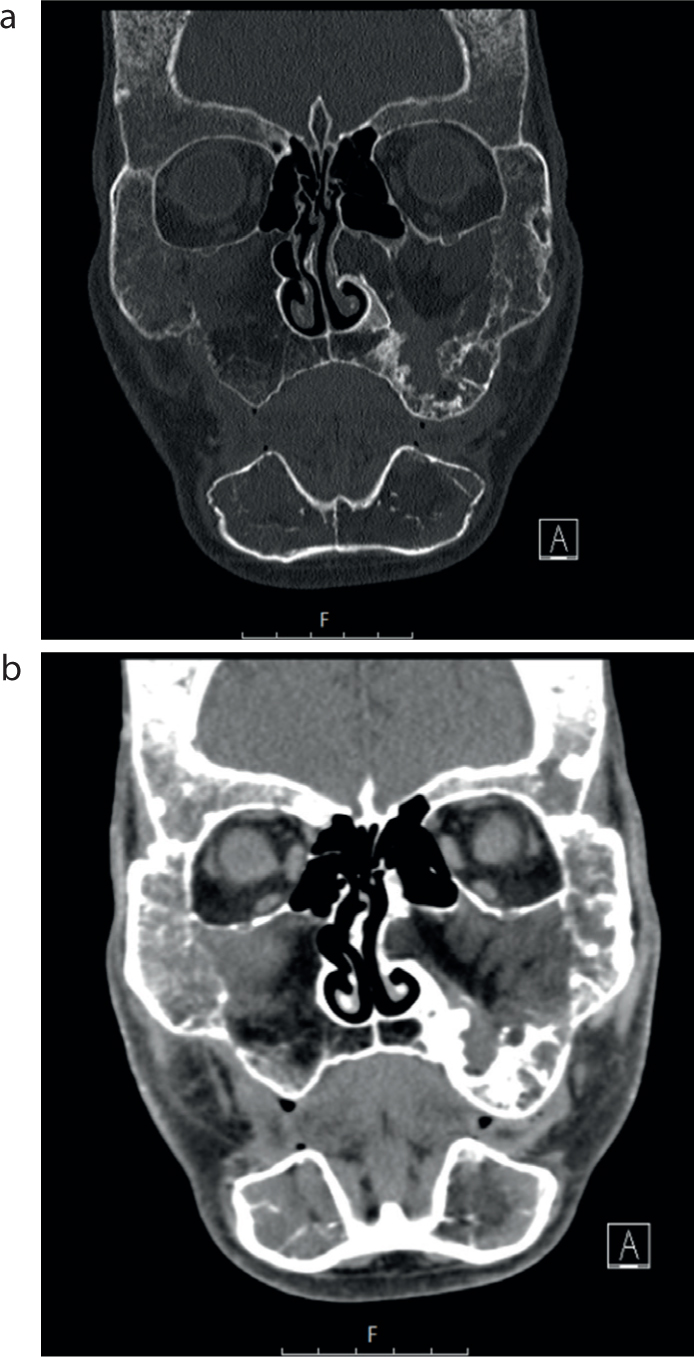
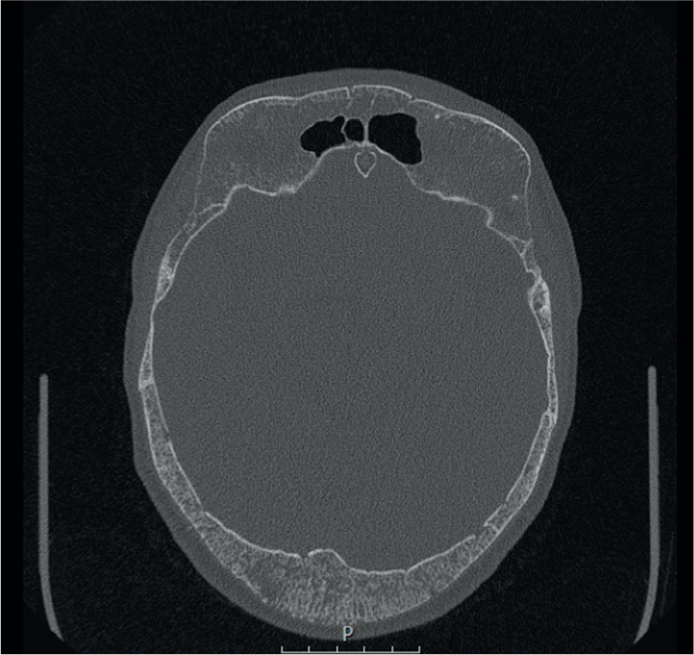
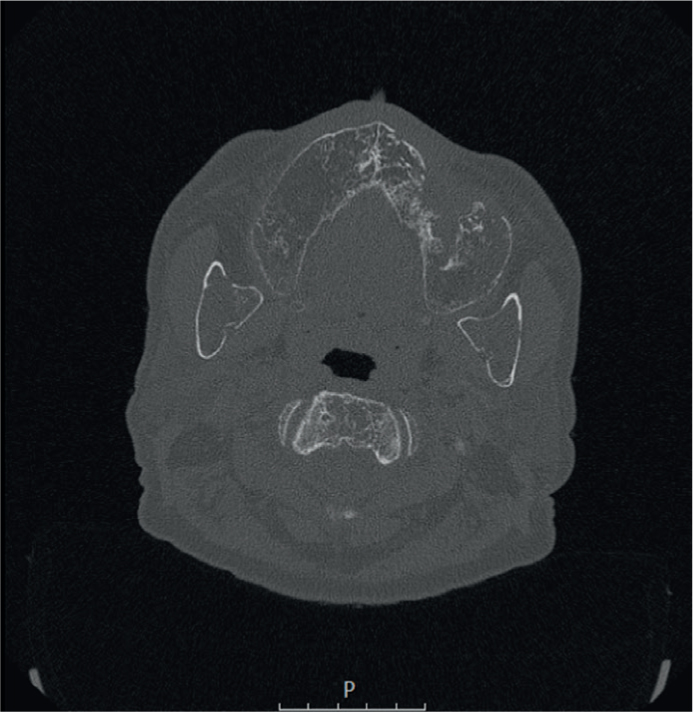
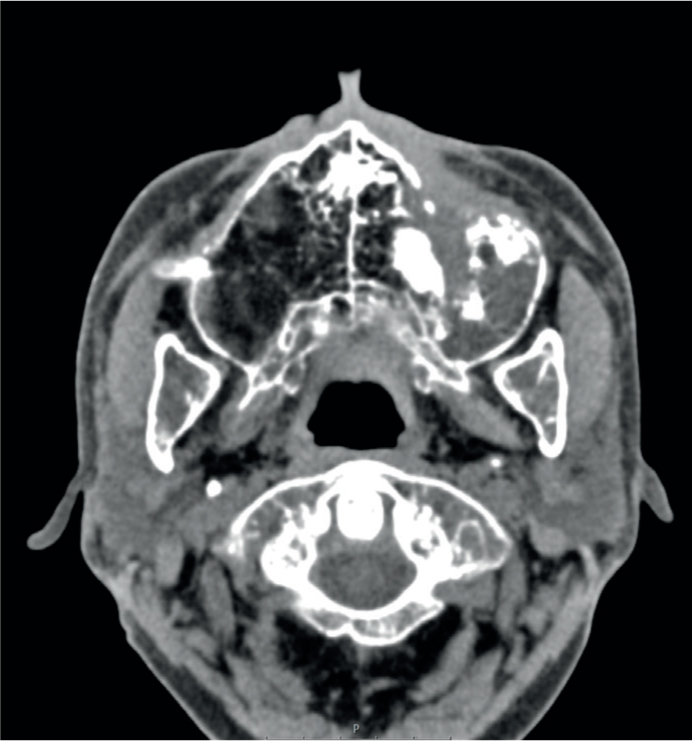
(a,b) Coronal slice at the approximate level of the ostiomeatal unit of an MDCT study (bony windows and soft tissue windows), which shows marked expansion of the facial bones with thinning of bony cortices and sparse trabeculation indicative of bone marrow hyperplasia. The cortices of the maxillary sinuses could not be identified and there was soft tissue occluding the bilateral maxillary sinuses (extramedullary haematopoiesis), this tissue extended into the left middle meatus.Figure 3. Axial slice at the level of the mid-cranium of an MDCT study (bony windows), which shows widening of the diploic space of the frontal and parietal bone with thinned cortices and the characteristic ‘hair-on-end’ appearance.Figure 4. Axial slice at the level of the mandibular foramen of an MDCT study (bony windows), which shows generalized osteopenia, thinning of the bony cortices and expansion of the maxillae and mandible. The historic surgical site of the left-sided Caldwell-Luc procedure was identifiable along the anterior wall of the left maxilla. There were no air spaces within the bilateral maxillae.Figure 5. Axial slice at the level of the odontoid peg of an MDCT study (soft tissue windows), which shows thinned bony cortices and expansion of the bilateral maxillae and visualized mandibular rami with fatty marrow tissue density. The historic surgical site of the left-sided Caldwell-Luc procedure was identifiable along the anterior wall of the left maxilla with associated scar tissue.
The CT sinus demonstrated marrow space expansion of the craniofacial bones, particularly affecting the maxilla, mandible and central skull base. Significant marrow space expansion of the maxilla combined with extramedullary haematopoietic tissue resulted in near complete obliteration of the maxillary sinuses, with additional extramedullary haematopoiesis present within the sphenoid sinuses. The ethmoidal air cells and frontal sinuses had been spared, and remained well pneumatized. In addition, there was an area of bony dehiscence inferiorly at the anterior wall of the left maxilla, consistent with a historical Caldwell-Luc procedure.
Further CT studies demonstrated similar appearances, with total opacification of the maxillary and sphenoid sinuses bilaterally, as well as the defect seen inferiorly at the anterior left maxilla (Figures 2 and 5).
A panoramic radiograph (Figure 1) showed enlargement of the edentulous maxilla, generalized osteopenia affecting all the imaged craniofacial skeleton. There were sparse, coarse trabeculae. The cortical outline of the mandible was significantly thinned (most evident along the inferior mandibular cortex) and the lamina dura around the mandibular teeth was not evident. The floor of the maxillary sinuses could not be identified and there was complete opacification of their expected air space.
Discussion
The effects of beta thalassaemia are widespread in the body, and depend on the severity of disease, as well as how well it has been managed, with patients with well controlled disease exhibiting fewer osseous manifestations.3 Patients with beta thalassaemia major develop symptoms from infancy, and subsequent management determines whether individuals will develop the severe symptoms of the disease. In addition to the primary effects of thalassaemia, this patient was diagnosed with a number of conditions directly related to his beta thalassaemia major and with conditions that occurred secondary to multiple blood transfusions.
Chronic anaemia
Owing to the reduced oxygen carrying capabilities of the red blood cells, patients with thalassaemia often develop chronic anaemia. This may be clinically evident as weakness, fatigue, and shortness of breath. The oral presentation of chronic anaemia includes atrophic glossitis and mucosal pallor.2
Haemosiderosis
Haemosiderosis (iron build-up within the body) may occur secondary to multiple blood transfusions, as the body has no effective mechanism to excrete iron.4 This excess iron may be become deposited in organs such as the heart, liver and spleen. Within organs, excess iron may cause progressive tissue injury, cirrhosis, and cardiomyopathy.4 It is important for dentists to be aware of haemosiderosis and its effects on the major organs. Damage to cardiac tissue can result in abnormal heart rhythms, increased likelihood of myocardial infarction and heart failure.5,6,7 Compromised liver function can have effects on clotting systems and drug metabolism. Liver function tests and coagulation screens should be carried out prior to invasive treatment owing to the increased risk of bleeding.2
Splenomegaly
The spleen is involved in the breakdown of red blood cells. In thalassaemia, there is a high rate of red blood cell destruction that may lead to hypersplenism, which in turn, can result in splenomegaly.5,8 In addition, splenomegaly may occur in relation to haemosiderosis. Splenomegaly may be associated with hypersplenism, and also with low levels of white blood cells (resulting in increased risk of infection), and low levels of platelets (resulting in prolonged bleeding times).9 Splenectomy is sometimes carried out to treat an enlarged spleen, which can, in turn, lead to a high risk of infection. Antibiotic cover must, therefore, be considered prior to dental treatment.2
Bone marrow hyperplasia and extramedullary haematopoiesis
Owing to the insufficient oxygen-carrying capabilities of the abnormal haemoglobin, there may be compensatory bone marrow hyperplasia and extramedullary haematopoiesis (EMH), whereby blood cell formation occurs outside the bone marrow. EMH can be seen as a result of many haematological disorders, such as sickle cell disease,10 and can affect almost all sites of the body.
The expansion of marrow spaces causes enlargement of affected bones and reduced pneumatization of the sinuses, with the exception of the ethmoid sinuses, which lack haematopoietic marrow.3 Clinically, patients may display typical features of enlarged cheekbones, depressed nasal bridge and protruding maxilla with Class II malocclusions.11 The appearance of the maxilla is often described as rodent or chipmunk facies.12
On dental radiographs, marrow hyperplasia results in a generalized radiolucent (osteopenic) appearance of the bones, sparse trabecular pattern, thinned bony cortices (most notably a very thin inferior cortex of the mandible) and loss of the lamina dura.12
The skull bones may show a distinctive appearance caused by marrow hyperplasia widening the diploic space of the skull vault. When the diploic space expands, the bony trabeculae become thicker. In the skull vault, the trabeculae have a perpendicular orientation. This results in a distinctive ‘hair on end’ appearance.13 The occipital bone is typically spared as it lacks bone marrow.
In adults, the floor of the maxillary sinuses should normally lie at, or below, the level of the floor of the nasal fossa.14 In individuals with reduced pneumatization of the maxillary sinuses, the maxillary sinus floor may be higher than the level of the floor of the nasal floor or, potentially, not identifiable. There may be apparent opacification of the maxillary sinuses (as in this case); however, this represents increased haematopoietic tissue filling up the air spaces within the craniofacial skeleton.12
This can be difficult to determine on plain radiographs and even with CT imaging, and may require MR imaging to confirm the presence of hypercellular marrow as opposed to mucosal thickening and inflammatory sinus disease. Classically in thalassaemia, the ethmoid air cells remain aerated and the occipital bone is spared (such as in this case evidenced by CT imaging of the sinuses). This is due to the lack of haematopoietic marrow within the ethmoidal and occipital bones.12
Causes of maxillary sinus opacification are numerous and, in this case, misdiagnosis of an opacified sinus led to the patient undergoing an unnecessary Caldwell-Luc procedure. Sinus opacification causes include chronic sinusitis, mucosal polyps, mucous retention cysts, tumours and fluid within the sinus secondary to trauma.15
Extramedullary haematopoiesis as a result of haematological disease should be noted as a rare cause of sinus opacification, which may be identified on dental imaging.
Osteoporosis
Osteoporosis is multifactorial in beta thalassaemia. A combination of marrow hyperplasia resulting in reduced bony trabeculae and thinned bony cortices, increased circulating iron in the blood stream causing damage to osteoblasts, and hormonal imbalances including growth hormone deficiency, hypothyroidism and hypoparathyroidism increase individuals' risk of developing osteoporosis.16,17,18 Osteoporosis may be evident on dental imaging by a generalized osteopenic trabecular pattern and radiolucent lacunae in the inferior cortex of the mandible.13 Patients with osteoporosis may be treated with bisphosphonates (such as in this case study). Combining the risks associated with long-term bisphosphonate therapy and increased susceptibility to infection secondary to splenomegaly or splenectomy, thalassaemia patients have an increased risk of developing MRONJ.
Conclusion
It is important for dental professionals to be aware of the spectrum of presentations associated with thalassaemia and how these may impact on the care they provide.
Where patients present with a diagnosis of thalassaemia, care should be taken to assess the dental imaging for any signs of changes that could be indicative of disease progress.