Langton S, Cousin GCS, Plüddemann A, Bankhead CR. Comparison of primary care doctors and dentists in the referral of oral cancer: a systematic review. Br J Oral Maxillofac Surg. 2020; 58:898-917 https://doi.org/10.1016/j.bjoms.2020.06.009
Cancer Research UK. Head and neck cancers statistics. 2020. https://tinyurl.com/yxfgppl2 (accessed October 2020)
Nutting C. Radiotherapy in head and neck cancer management: United Kingdom National Multidisciplinary Guidelines. J Laryngol Otol. 2016; 130:S66-S67 https://doi.org/10.1017/s0022215116000463
Liu C, Mann D, Sinha UK, Kokot NC. The molecular mechanisms of increased radiosensitivity of HPV-positive oropharyngeal squamous cell carcinoma (OPSCC): an extensive review. J Otolaryngol Head Neck Surg. 2018; 47 https://doi.org/10.1186/s40463-018-0302-y
Goodson AMC, Payne KFB, Brennan PA. Important oral and maxillofacial presentations for the primary care clinician.Faringdon: Libri; 2016
Paleri V, Roland N. Introduction to the United Kingdom National Multidisciplinary Guidelines for Head and Neck Cancer. J Laryngol Otol. 2016; 130:S3-S4 https://doi.org/10.1017/S0022215116000359
Amin M, Edge S, Greene F AJCC Cancer Staging Manual, 8th edn. : Springer International Publishing; 2017
Cocks H, Ah-See K, Capel M, Taylor P. Palliative and supportive care in head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J Laryngol Otol. 2016; 130:S198-s207 https://doi.org/10.1017/s0022215116000633
American Cancer Society. Surgery for oral cavity and oropharyngeal cancer. 2018. https://tinyurl.com/y75eykhr (accessed October 2020)
Woolgar JA, Triantafyllou A, Lewis JS Prognostic biological features in neck dissection specimens. Eur Arch Otorhinolaryngol. 2013; 270:1581-1592 https://doi.org/10.1007/s00405-012-2170-9
Kerawala C, Roques T, Jeannon JP, Bisase B. Oral cavity and lip cancer: United Kingdom National Multidisciplinary Guidelines. J Laryngol Otol. 2016; 130:S83-S89 https://doi.org/10.1017/s0022215116000499
Goodson AM, Kittur MA, Evans PL, Williams EM. Patient-specific, printed titanium implants for reconstruction of mandibular continuity defects: A systematic review of the evidence. J Craniomaxillofac Surg. 2019; 47:968-976 https://doi.org/10.1016/j.jcms.2019.02.010
Wu CC, Lin PY, Chew KY, Kuo YR. Free tissue transfers in head and neck reconstruction: complications, outcomes and strategies for management of flap failure: analysis of 2019 flaps in single institute. Microsurgery. 2014; 34:339-344 https://doi.org/10.1002/micr.22212
Kowalski LP. Results of salvage treatment of the neck in patients with oral cancer. Arch Otolaryngol Head Neck Surg. 2002; 128:58-62 https://doi.org/10.1001/archotol.128.1.58
Pompa G, Saccucci M, Di Carlo G Survival of dental implants in patients with oral cancer treated by surgery and radiotherapy: a retrospective study. BMC Oral Health. 2015; 15 https://doi.org/10.1186/1472-6831-15-5
Woods B, Schenberg M, Chandu A. A Comparison of Immediate and Delayed Dental Implant Placement in Head and Neck Surgery Patients. J Oral Maxillofac Surg. 2019; 77:1156-1164 https://doi.org/10.1016/j.joms.2019.02.007
Mouth Cancer: the Maxillofacial Surgeon's perspective Alexander MC Goodson Satyesh Parmar Prav Praveen Matthew Idle Timothy Martin Dental Update 2024 47:10, 707-709.
Consultant Head and Neck, Oral and Maxillofacial Surgeon, Department of Oral and Maxillofacial Surgery, Queen Elizabeth Hospital, Mindelsohn Way, Birmingham B15 2TH, UK
This article summarizes current practice according to UK guidelines for the management of oral cancer from the perspective of the oral and maxillofacial surgeon. The article discusses the patient pathway, starting with recognition of sinister features by the general dental practitioner in primary care and referral to specialist oral and maxillofacial surgery services, followed by the multidisciplinary approach to tumour staging, cancer treatment planning and delivery, and finally key issues in the ‘post-treatment’ phase of cancer care. Additional focus is provided for some of the surgical treatments and anatomical and physiological changes, of which the general dental practitioner should have some understanding.
CPD/Clinical Relevance: General dental practitioners play a key role in the detection and early management of oral cancer, referring approximately 40% of all cases to secondary care. It is therefore important to understand key milestones and technical elements of the patient's journey.
Article
Introduction
General dental practitioners play a key role in the detection and early management of oral cancer, referring approximately 40% of all cases to secondary care, as well as the post-treatment phase of cancer care.1 Head and neck cancer in general is the eighth most common cancer in the UK and is four times more common in men than in women. The incidence has increased in both sexes since the 1990s with a greater percentage increase among females, closing the gender difference in incidence over time.2 Late-stage disease is a more common presentation than early-stage disease (62% are stage III/IV at presentation versus 38% at stage I/II).3 In the case of oral cancer specifically (anterior to the hard/soft palate junction and tonsils), surgery is the commonest and most effective form of curative treatment, often requiring wide local resection of soft tissues with bone, if needed, ensuring a clinical margin of 1 cm. This can have significant consequences for oral function, dental rehabilitation and facial aesthetics. For advanced squamous cell carcinomas (SCCs), combined treatment modalities (surgery and radiotherapy with/without chemotherapy) offer the highest chance of cure.4 In some cases, typically because of patients' fitness for surgery, radiotherapy (with/without chemotherapy) may be the primary treatment modality for curative intent. For oropharyngeal and hypopharyngeal cancer (posterior to the hard/soft palate junction, tonsils and tongue base), treatments are more variable, with the use of radiotherapy, chemoradiotherapy and surgery to varying degrees, depending upon the patient, tumour and local resources. Oropharyngeal tumours are much more radiosensitive to radiotherapy, particularly if associated with human papilloma virus (HPV).5
Regardless of the anatomical site of the tumour, treatments are significant and almost always compromise patient's health-related quality of life. The general dental practitioner, therefore, has a crucial role in detection and early management of oral cancer because the consequence of delayed presentation to secondary care, leading to advanced tumour stage, can be catastrophic; both prognostically and because of treatment side-effects.
This article discusses the patient's journey following referral from primary care for a suspected head and neck cancer, including the clinical assessment in secondary care, diagnostics and the multidisciplinary approach to definitive management. Furthermore, we also touch upon post-cancer care including surveillance, dental rehabilitation and potential issues that may arise from radiation-related complications.
Receiving the referral and first presentation in the oral and maxillofacial surgery clinic
Most patients with head and neck cancer present to the oral and maxillofacial surgery (OMFS) team from primary care as an already-suspected cancer. Very few are detected through ‘routine’ referral pathways. Although there is local variation, cases referred as ‘suspected cancers’ are often benign pathologies, such as fibroepithelial polyps or aphthous ulcers, for example. Consequently, a large proportion are downgraded to a ‘routine’ pathway following either vetting of referrals in the office, or at initial presentation to the OMFS clinic. Therefore, in current practice, as well as investigating and managing head and neck cancer the oral and maxillofacial (OMF) surgeon often acts as a secondary-care gatekeeper to cancer diagnostics, ‘fast-tracking’ and ‘downgrading’ referrals accordingly. The history of the presenting complaint and examination findings in the referral letter are crucial. The recognition of the sinister features of oral cancer presentations has been promoted by the British Association of Oral and Maxillofacial Surgeons (BAOMS) and the Royal College of General Practitioners (RCGP) (Table 1), and such features, if included in the referral, will raise the suspicion for the receiving surgeon.6 For example, a referral for ‘a non-healing ulcer’ provides a bare minimum of information and could apply to multiple possible benign pathologies, as well as a possible cancer. However, ‘a non-healing ulcer, on the lateral border of the tongue present for more than 3 weeks with underlying firmness/induration and a strong smoking history’ is almost diagnostic of a tongue cancer and could help the patient obtain a quicker consultation, diagnosis and treatment.
Presentation category
Sinister features
Oral ulcer
Not healing after 3 weeks, firm/indurated, high-risk site (lateral tongue, floor of mouth, anterior and base of tongue, retromolar, tonsil, oropharynx, attached gingiva, lip), painless, irregular edge, history of oral cancer, palpable neck nodes, near/associated loose teeth, risk factors (eg smoking, alcohol, betel nut chewing, previous oral/oropharyngeal cancer)
Fixed to underlying structures, firm consistency, multiple, rapidly enlarging, persistent for more than 3 weeks, hoarse voice/difficulty swallowing, irregular shape, nerve symptoms (numbness/weakness), risk factors
Nerve symptoms (altered sensation/pain)
Associated swellings/ulcers, palpable neck nodes, associated motor (orofacial/neck muscle) weakness, entire distribution of sensory nerve involved (not just in part), associated trismus (suggesting skull base/infratemporal fossa involvement), rapidly progressive symptoms, disturbance of vision/hearing/swallowing and other cranial nerve functions, risk factors
Once the OMFS consultant has seen the patient and a cancer diagnosis is suspected, this must be confirmed through biopsy; typically performed under local anaesthesia in the outpatient department. In many centres, a histological cancer diagnosis is confirmed before imaging investigations are requested to ‘stage’ the tumour. However, in some circumstances, it is wise to undertake imaging investigations beforehand. For example, if biopsy would cause significant artefact to subsequent staging scans (causing false-positive ‘upstaging’ of the tumour in the case of MRI scans, for example) or imaging will assist the biopsy process (eg ultrasound/CT-guided core biopsy or fine-needle aspiration). A biopsy before the scan may also upstage the neck and make it difficult to differentiate between inflammatory and metastatic nodes. The biopsy should ideally be performed after the treating consultant has seen the patient and therefore should not be undertaken in dental practice.
Tumour staging is a crucial process in modern cancer care. It provides a prognostic ‘code’ for each patient's tumour. In combination with evidence-based UK head and neck cancer guidelines and a local and/or regional multidisciplinary team (MDT) discussion, along with other patient-related factors such as comorbidity and performance status, the tumour stage will dictate the patient's treatment accordingly; curative or palliative, with treatment modality being operative (surgery), non-operative (eg chemoradiotherapy or best supportive care) or combinations thereof.7 The head and neck multidisciplinary team (MDT) meeting is typically a weekly occurrence where physicians (including surgeons and oncologists) present new cancer cases to the remainder of the team. Along with other doctors (radiologists and pathologists), hospital dentists, nurse specialists and allied professionals, such as speech and language therapists, dietitians, dental therapists and hygienists (to name but a few), cases are prognosticated and a treatment plan is tailored to the patient's biopsychosocial needs.
Clinical tumour staging (based on initial clinical and radiological findings) is currently conducted for all new head and neck cancer cases in the United Kingdom according to the Tumour, Node and Metastasis algorithm provided by the American Joint Committee on Cancer (AJCC) version 8 (TNM-8).8 Depending on the number and type of investigations required, as well as local resource availability, the staging process and MDT discussion can take days to weeks to complete, before any treatment is provided. For this reason, UK centres adhere to strictly enforced cancer pathway timeframes. NHS England follows the 2-week wait (2WW) policy for which the timeline from referral in primary care to a specialist consultation must be no greater than 2 weeks. Following this, a maximum period of 31 days is allowed from the date of ‘decision to treat’ (in agreement with the patient) to the patient receiving the actual treatment, with a maximum total of 62 days from referral in primary care to first treatment. The minimum expected standard in NHS England is 85% compliance for the 62-day overall timeframe (Figure 1). Similar policies exist for the rest of the UK where standards may differ slightly.9 It is apparent, therefore, from the OMF surgeon's perspective, there are numerous logistical elements to negotiate in providing high-quality evidence-based multidisciplinary cancer care, in addition to his/her job of performing cancer surgery itself. The general dental practitioner can greatly assist his/her local head and neck cancer centre by providing a clear rationale for urgent consultation and cancer diagnostics in the original referral letter. Where there is no clear rationale for an urgent cancer referral and no sinister features identified at initial presentation in the dental surgery, it is important to consider the most appropriate alternative referral route in order to ensure cancer resources are directed towards patients who need them the most.
Figure 1. A typical head and neck cancer care pathway from referral to delivery of treatment (based on the head and neck multidisciplinary pathway at University Hospitals Birmingham, UK).
Treatments
Regardless of whether the aims of treatment are curative or not, all cancer care in the UK must be multidisciplinary. The fundamental ethical principles for provision of medical care include non-maleficence (doing no harm), beneficence, justice and respect for autonomy.10 Where cure is not feasible, either due to disease severity, or because curative treatment could be more harmful than beneficial to the patient (eg if the patient is unfit for major surgery or curative doses of chemo/radiotherapy), a palliative approach may be needed. Although palliation is chiefly led by consultants in palliative care medicine, other members of the MDT may still be required to make a significant contribution, for example: debulking of fungating tumours; delivery of palliative radiotherapy for symptom control; provision of gastrostomy tube feeding (where appropriate); oral care; pain management; and psychological counselling. The main targets for palliative care interventions in head and neck cancers include medical/surgical treatments (managing pain, hydration, nutrition, gastrointestinal symptoms, anxiety, agitation, dysphagia, dyspnoea, bleeding, the airway and hypercalcaemia), as well as holistic, psychosocial and complementary treatments (breaking bad news, dealing with patient aspirations/expectations, anxiety, counselling/psychological/emotional support and other complementary therapies).10 Dental professionals may play a key role in palliation by relieving dental/mucosal pain, providing prosthetic support to help the patient with eating, as well as psychosocial function: maintaining the patient's social life, and therefore something to enjoy living for.
Fortunately, with the developments in curative treatments for oral cancer, including the accessibility to major surgical resections aided by advanced reconstructions to preserve function and quality of life (such as composite free-tissue transfer with microvascular techniques incorporating osseointegrated dental implants), as well as improvements in the safety of general anaesthesia, even those with advanced stage disease (stage III/IV) are commonly suitable for curative surgery, and able to maintain a reasonable quality of life.11 Prognosis for cure depends on tumour characteristics and nodal status (the presence or absence of lymph node metastases), hence the importance of the TNM-8 staging system. For early tumours (T1/2) specifically, lymph node involvement is crucial: the presence of a single lymph node metastasis reduces survival by half.12 It is therefore extremely important for cancer patients to be referred before nodal spread occurs.
Surgery with curative intent
For oral cavity tumours in general, surgery is usually the primary treatment modality, although some factors (most commonly patient rather than disease related) may favour the use of external-beam intensity-modulated radiotherapy primarily. Surgery can vary from simple wide local excision to major resections (typically requiring additional procedures, such as neck dissection, temporary tracheostomy and free-tissue reconstructions using microvascular techniques).
Squamous cell carcinoma is the commonest type of oral cancer and tumour resection in the form of wide local excision, aiming for a 10-mm peripheral and deep tissue margin (soft tissue or bone), is the treatment of choice for the primary tumour. Elective (prophylactic) treatment of the clinically/radiologically node-negative neck must be offered to all patients (be it in the form of elective neck dissection, radiotherapy or sentinel node biopsy as a staging technique). For patients with known or suspected neck node metastases, a modified-radical or radical neck dissection is needed, and typically in combination with adjuvant radiotherapy or chemoradiotherapy (depending on number/size of involved nodes and the presence/absence of extracapsular extension where the cancer ‘bursts’ out of an involved node into the surrounding tissues). Similarly, for the greatest chance of survival, adjuvant treatments should be considered for advanced tumour stage (T3/T4) and other unfavourable tumour characteristics (such as perineural invasion).13
Major surgery for oral cavity cancers
As mentioned above, many, if not the majority of, oral cancers present at a late stage, typically as large primary tumours or in the presence of nodal metastases. Consequently, surgery with curative intent requires aggressive resection with wide margins, in combination with neck dissection and airway protection with a covering tracheostomy. For small tumours (T1 and some T2 tumours), primary closure of the defect or secondary-intention healing (leaving the wound open to granulate) may be achievable without significant functional compromise. However, tumours of the floor of mouth, tongue and any other oral cavity tumours greater than T2 stage commonly indicate formal reconstruction. Reconstructive strategies have generally moved away from the use of obturators (although still used for some good indications) and regional flaps (such as the pectoralis major myocutaneous flap). Instead, free-tissue transfer using microvascular anastomosis techniques (suturing of arteries and veins from a free-tissue flap, to corresponding vessels in the head and neck) has now become the gold standard; providing an immediately vascularised piece of tissue within the tumour resection defect. This not only reinstates integrity of the oral cavity/alimentary tract as a barrier to ingress of bacteria and infection, but also aids aesthetic functional rehabilitation, be it through maintaining tongue mobility for adequate speech and swallow, or through providing vascularised bone for the subsequent (or even immediate) placement of dental implant fixtures. The incorporation of virtual surgical planning and computer-aided design and manufacturing into major composite (bone and soft tissue) free-flap jaw reconstructions has further expanded aesthetic and functional capabilities, as well as shortening surgical duration.14
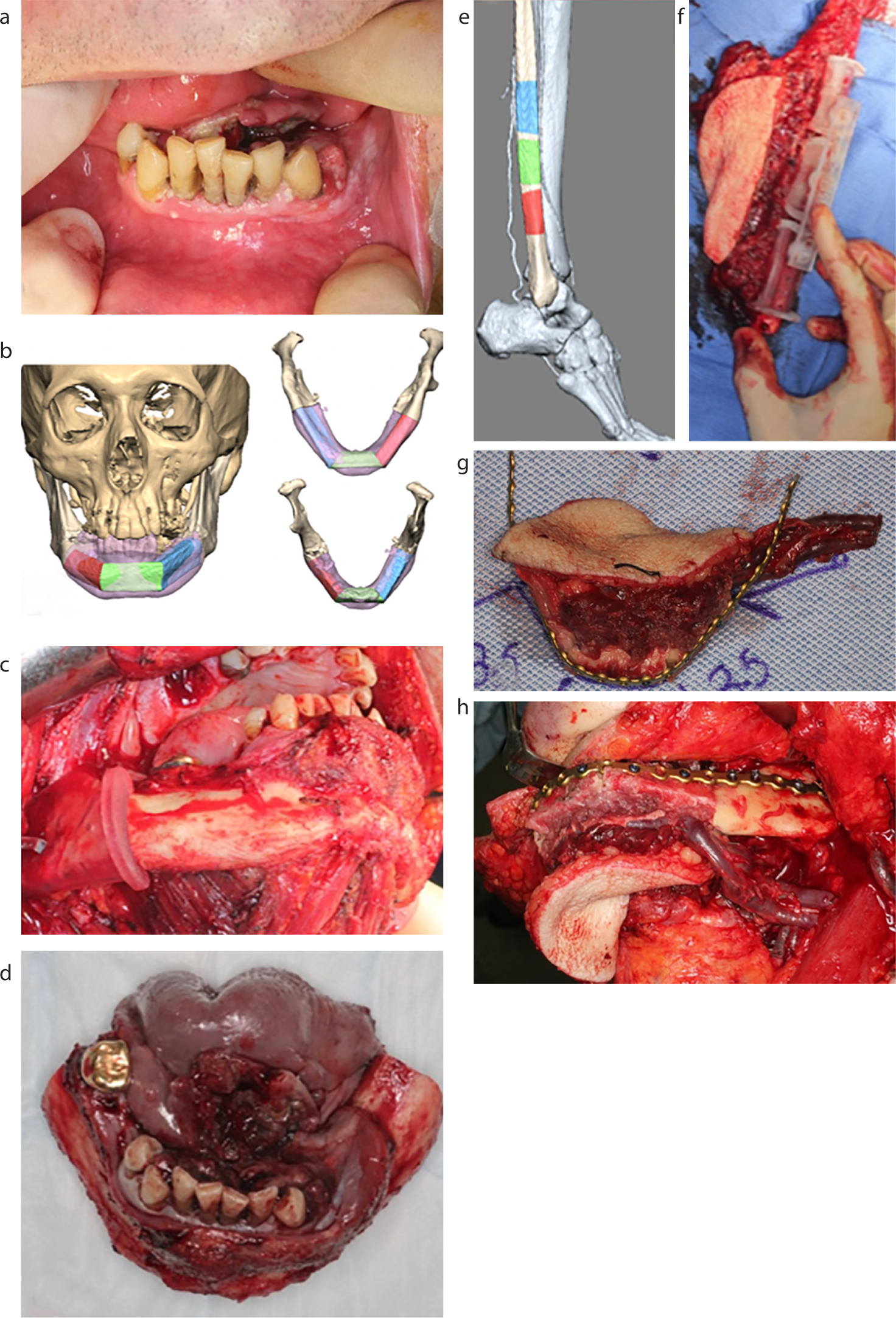
Many types of free-flaps are available for use, providing the donor site tissue, vessels and recipient site vessels are healthy (unaffected by peripheral vascular disease, for example). Patient comorbidities can be a limit to the use of these advanced reconstructive techniques because the risk of complications (both flap failure and systemic morbidity) may become unacceptably high. Fortunately, widespread training in these techniques means that many surgeons are able to keep free-flap failure rates below 5%.15 Free-flap reconstructions may include soft tissue-only flaps, such as the radial forearm flap and anterolateral thigh flap, or composite flaps, such as the fibular flap (Figure 2), which is ideal for mandibular reconstruction with implant-based dental rehabilitation (Figure 3). Other common composite flaps used include the scapular and deep circumflex iliac artery (DCIA) flap (Figure 4). Nevertheless, in some situations, alternative strategies such as regional pedicled flaps (such as the pectoralis major, temporalis muscle or nasolabial flaps), obturators (Figure 5), or no formal reconstruction (accepting associated deformity and functional impairment) may be more appropriate.
Figure 2. (a) Anterior mandibular squamous cell carcinoma; (b) virtual surgical planning of mandibulectomy and fibular free flap reconstruction; (c) right side margin of mandibular resection with cutting guide in situ; (d) mandibulectomy specimen; (e) planned fibular flap harvest; (f) positioning of cutting guide for osteotomies of fibular flap; (g) assembled fibular flap before implantation; (h) fibular flap inset into final position with microvascular anastomoses of pedicle to neck vessels.Figure 3. (a) Orthopantomogram (OPG) of fibular flap reconstruction of the mandible prior to implant-based dental rehabilitation; (b) virtual surgical planning of position and angulation of fixtures; (c) OPG after fixture placement; (d) implant retained prosthesis in situ with underlying fibular flap skin paddle intra-orally; (e) final dentofacial aesthetics.Figure 4. (a) model of left maxillary tumour; (b) virtual plan of deep circumflex iliac artery (DCIA) flap reconstruction; (c) post-resection defect of maxilla; (d) harvested DCIA flap with vascular pedicle ready for microvascular anastomosis; (e) OPG following DCIA flap reconstruction of left maxilla and dental implant fixture placement; (f) occipitomental view of orbital implants and DCIA flap; (g) facial aesthetics with implant-retained orbital prosthesis.Figure 5. (a) right maxillectomy defect; (b) obturator and (c) obturator in situ.
When obtaining informed consent from a patient for major head and neck cancer surgery, the surgeon will typically describe the procedure as a series of smaller operations, including a surgical tracheostomy for peri-operative airway protection, tumour resection, neck dissection and free-flap reconstruction (with/without immediate placement of dental implant fixtures). Dental implants may be inappropriate for some patients who may have difficulty maintaining oral hygiene. In some cases, perfectly reasonable prosthetic rehabilitation can be achieved with conventional dentures and, in other cases, prosthetic dental rehabilitation may not be needed at all; depending upon the patient's suitability and expectations.
Post-treatment care: surveillance and rehabilitation
Following definitive treatment with curative intent, head and neck cancer patients in the UK are followed-up for at least 5 years, using clinical surveillance (regular consultations and examinations with the surgeon/oncologist) with/without surveillance scanning of the head and neck and/or chest. Approximately 60% of oral cancer patients will survive 5 years or longer after treatment.16 Detection and treatment of tumour recurrence allows for salvage treatments, which may extend life expectancy, and possibly provide definitive cure for a few, although locoregional recurrence is a poor prognostic factor for the majority. For example, 50% of patients with neck node recurrence in oral cancer are typically not considered viable candidates for salvage therapies. The likely survival benefit of salvage surgery or radiotherapy to the neck depends on the type of previous neck dissection, previous radiotherapy and the interval free of recurrence.17 The 5-year surveillance period is typically, therefore, the surgeon's last opportunity in the patient's cancer journey to have an impact on overall survival. Furthermore, although a large topic in itself, and a detailed summary is beyond the remit of this article, management of treatment-related complications such as osteoradionecrosis (ORN) is another task that the oral and maxillofacial surgeon will frequently manage in combination with the general dental practitioner. Prevention and treatment of ORN ranges from simple oral hygiene measures, such as use of chlorhexidine rinses, avoidance of dental extractions and a very proactive policy for restoration of compromised teeth wherever possible, to secondary care interventions by the surgeon, such as the prescription of long-term drug therapies, superficial debridement or even segmental resection of bone with/without free-flap reconstruction for the most severe cases. Fluoride supplementation with high-concentration toothpastes and/or fluoride trays are generally recommended, not only because of the risk of ‘radiation-caries’ as a disease in itself (induced by impaired salivary production following radiotherapy), but also because of the potential consequence of osteoradionecrosis either spontaneously from periapical infection or after the extraction of a carious tooth.
Alongside ensuring adequate nutrition (be it orally or through enteral tube feeding, such as gastrostomy), and development of speech and swallow function with the dietitian and speech and language therapist, prosthetic dental rehabilitation is often a crucial part of the patient's recovery to ‘near normality’, not only for oral function, but also for aesthetics and psychosocial wellbeing. Generally, dental implant fixtures are either placed immediately at the time of the resection and free-flap reconstruction, or otherwise placed 1–2 years postoperatively once the patient has completed all adjuvant treatment (if needed) and survived the high-risk post-surgical period for locoregional recurrence. There is evidence to suggest that both the use of radiotherapy after placement of dental implants and early loading protocols significantly increase the risk of implant failure as does anatomical site.18 However, there is also evidence to the contrary, that immediate fixture placement is safe and effective.19 Consequently, practice varies among UK maxillofacial units according to local protocols.
Summary
Oral cancer is a challenging disease, frequently presenting at a late stage. Early detection and referral by the general dental practitioner, with clear documentation of the specific sinister features on history and examination can expedite diagnosis and treatment for patients, having a dramatic impact upon survival. Furthermore, because of the potentially aggressive nature of the treatments required for late-stage disease, detection of tumours early on will also impact upon health-related quality of life for cancer survivors. Major surgical resections and free-tissue reconstructions are the gold standard, and the general dental practitioner should have some understanding of surgical and medical techniques used to appreciate the normal changes in anatomy (eg the presence of intra-oral skin paddles, radiotherapy changes to the mucosa or autotransplanted bone visible on the orthopantomogram) to be comfortable and confident with providing general dental care following cancer treatment.