Benington IC, Lappin C, Linden GJ, Thompson R. The clinical success and periodontal evaluation of patients rehabilitated with light-cured obturators. J Oral Rehabil. 1996; 23:135-138
Daley T, Darling M. Nonsquamous cell malignant tumours of the oral cavity: an overview. J Can Dent Assoc. 2003; 69:577-582
Macfarlane GJ, Boyle P, Sculley C. Rising mortality from oral cancer of the tongue in young Scottish males. Lancet. 1987; 2
Macfarlane GJ, Boyle P, Sculley C. Oral cancer in Scotland: changing incidence and mortality. Br Med J. 1992; 305:1121-1123
Gordon DS, Blair GA. Titanium Cranioplasty. Br Med J. 1974; 2:478-481
Winder J, Cooke RS, Gray J, Fannin T, Fegan T. Medical rapid prototyping and 3D CT in the manufacture of custom made cranial titanium plates. Med Eng Technol. 1999; 23:26-28
Prosthodontic rehabilitation of patients with orofacial defects Ian C Benington C Andrew Burnett Tom J Clifford Dental Update 2024 39:4, 707-709.
Authors
Ian CBenington
BDS, FDS RCS, FFD, RCSI, FDS, RCPS, MRD RCS
Emeritus Professor/Consultant in Dental Prosthetics and Materials Science, School of Dentistry Queen's University Belfast and The Royal Group of Hospitals, UK
In 2007 in the UK, 5410 people were diagnosed with an oral cancer. It is therefore imperative that all dentists, medical practitioners and dental care practitioners are vigilant when examining the oral cavity so that any suspicious ulcers, swellings or changes in colour of the mucosa are referred at the earliest stage. To give the patient the best prognosis with an orofacial defect following tumour removal or trauma, it is most important to have the appropriate skills in a multidisciplinary team. The management of patients comprises pre-surgical, surgical and post-surgical phases.
Clinical Relevance: The management of patients and clinical techniques described have proved to provide satisfactory outcomes for patients with orofacial defects.
Article
In 2007, in the UK 5410 people were diagnosed with an oral cancer.1 This is an important statistic since it indicates that those who examine the mouth regularly may encounter tumours. Early diagnosis is therefore of great importance in relation to the management of patients with these lesions. It is imperative that all dentists, medical practitioners and dental care practitioners are vigilant when examining the oral cavity so that any suspicious ulcers, swellings or changes in colour of the mucosa are referred at the earliest stage.
Tumours that occur in the upper jaw include:
Squamous carcinoma of the maxilla antrum;
Adenoid cystic carcinoma of the minor salivary glands;
Pleomorphic salivary adenoma which, although benign, may result in a permanent defect on removal.
Tumours that occur in the lower jaw include:
Squamous carcinoma of the tongue;
Squamous carcinoma of the floor of the mouth and the alveolar mucosa;
Sarcoma of mandibular bone;
Secondary tumours.
Figure 1 shows an example of an adenoid cystic carcinoma in the palate.
Figure 1. Adenoid cystic carcinoma of the palate.
The team approach
To give the patient the best prognosis with an orofacial tumour it is most important to have the correct skills in a multidisciplinary team. This should include the general dental practitioner, who may well be the first to have diagnosed the tumour, an oral and maxillofacial surgeon, an oncologist and an ENT surgeon or plastic surgeon, whose role it will be to plan the surgery. The responsibility for restoration lies with the prosthodontic or restorative specialist who has been trained to care for patients with such disability, along with a maxillofacial technician, dedicated dental nurse, therapist, hygienist and speech therapist. The team should also include a dietician since the patient will require specially prepared food in the post-operative phase and may require a gastric tube for a short time.
Planning management of the patient
It is most important that the management of the patient is clearly seen as:
Pre-surgical;
Surgical;
Post-surgical.
The pre-surgical phase will include the referral of the patient with a suspicious lesion to a specialist oncology unit where a diagnosis will be confirmed. Once the exact location and size of the tumour has been identified the rest of the multidisciplinary team should confer with the surgeon to discuss the best management strategy for the patient. If the tumour is in the upper jaw, then it is probable that during surgery a communication will be made from the mouth into the nasal cavity/antrum and, depending on the size of the tumour, this may involve the removal of part of the alveolus, including the antral floor or a radical hemi-maxillectomy. At this stage, once the extent of the surgery has been outlined, the prosthodontist will design an appropriate immediate obturator to be inserted in theatre after the resection of the tumour. Selecting teeth of a suitable mould and shade will ensure the maintenance of a natural appearance.
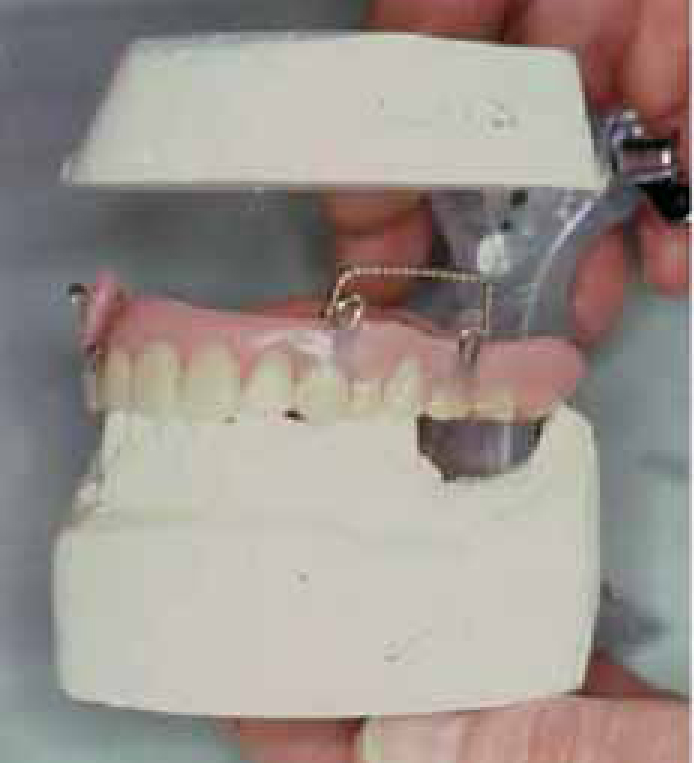
The immediate obturator (Figure 2) serves the following purposes:
Figure 2. An upper partial immediate obturator, on the articulator, with cleats for maxillary fixation and a stainless steel loop to retain the obturator material.
It restores the vital oral functions post-operatively;
It restores aesthetics to the patient post-operatively;
It restores the patient's morale;
It preserves the surgical cavity and facial form.
Factors which contribute to the retention of the immediate obturator.
Dental status;
Planned excision of tissue at time of operation;
Optimum design of the appliance;
The use of undercuts within the surgical defect;
Employing circum-zygomatic wires or a palatal screw for fixation.
If the patient is partly dentate then obviously the remaining teeth on the unaffected side are useful to provide direct retention. Conversely, if the patient is edentulous, there are potentially more problems with retention of the immediate and any subsequent obturators (Figure 3).
Figure 3. An immediate obturator showing where obturator material has engaged buccal and palatal undercuts.
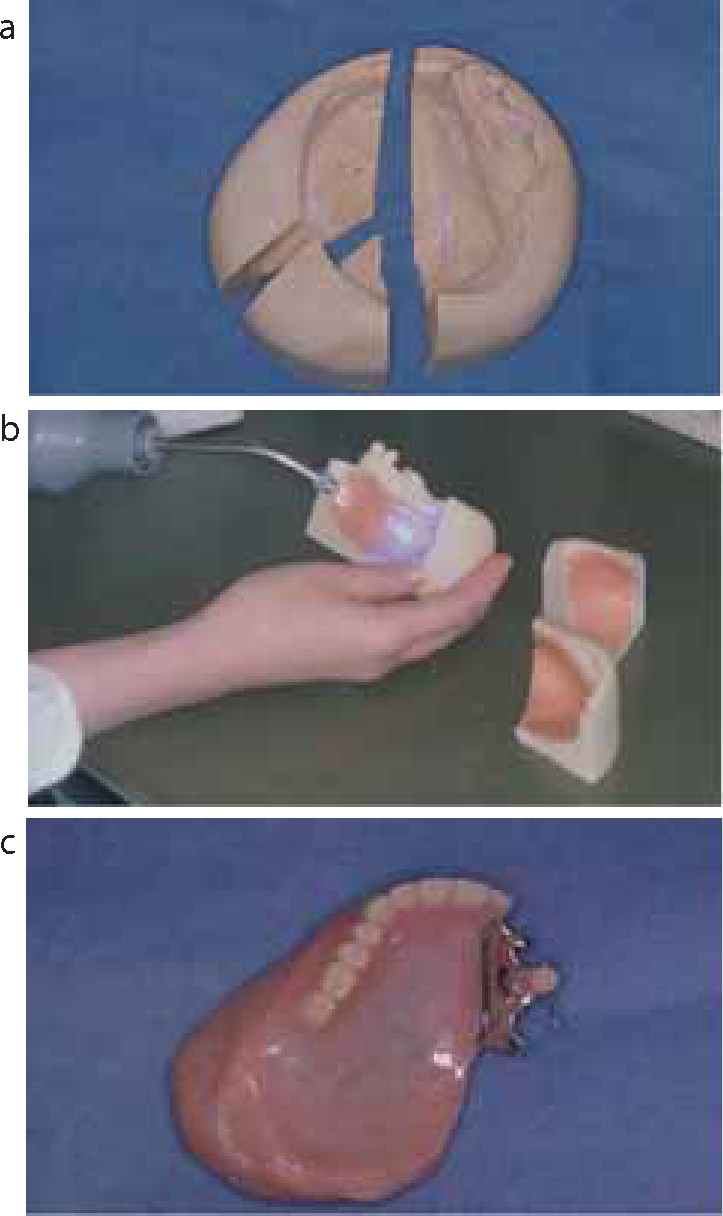
It is important at the pre-surgical planning stage to emphasize that any area that may provide natural undercuts, and is not involved with the tumour, should be retained to provide optimal retention and support for the appliance within the surgical defect (Figures 4 a–c).
Figure 4.
(a) Extensive melanoma of palate. (b) Immediate obturator using only premaxillary segment of teeth for retention. (c) Post-operative defect.
If the surgical defect is large, the immediate obturator will be heavier and more difficult to retain, whereas if the defect is small the obturator will probably retain without any additional fixation.
The importance of the co-operation between team members cannot be overemphasized since the retention of a segment of teeth in an otherwise total hemi-maxillectomy may be the key to the patient being able to retain a properly designed immediate obturator and to perform all the normal oral functions which are so important to the patient's wellbeing, both physically and psychologically. (Figure 5).
Figure 5. Intermediate obturator for partially dentate patient. Cobalt chromium base with direct retainers.
Occlusion of the immediate obturator
Nasal intubation on the unaffected side is the anaesthetic route of choice as an oral anaesthetic tube will prevent the immediate obturator being fitted in correct occlusion with the lower arch. For the patient to function comfortably, the correct occlusion must be established at the time of assessment of the immediate obturator in theatre (Figure 6).
Figure 6. Correct occlusion established.
The surgical procedure
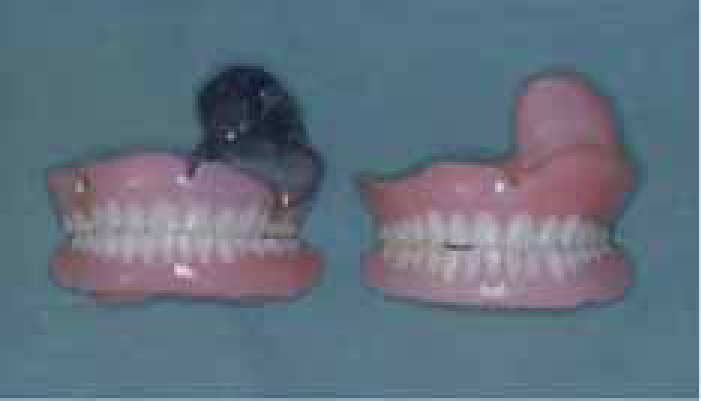
In theatre the normal procedure is for the surgeon to complete the agreed resection of the tumour, preserving any tissues which may be helpful in retaining the prosthesis. The immediate obturator is fitted by the prosthodontist using, preferably, silicone putty or soft black gutta-percha, which is more porous and difficult to use (Figure 7). Once the obturator is fully seated and the obturator material has been moulded to support the cheek flap to provide its normal contours, the fixation of the obturator may proceed. Where circum-zygomatic wiring and fixation are employed it has been found that it is useful to use a circum-zygomatic wire and a secondary loop from that wire to the cleat on the obturator, either unilaterally or bilaterally, as the case may require. This permits ready removal of the obturator for early post-operative examination by simply removing the secondary loops and leaving the circum-zygomatic wires in situ, in the interest of patient comfort. It also facilitates removal and replacement of the immediate obturator for examination and cleansing of the cavity during the immediate post-operative healing period. Retention may also be gained using surgical bone screws. Whilst their insertion is relatively easy, replacement is difficult without anaesthetic.
Figure 7. Assessment of immediate obturator prior to moulding material.
The surgeon will wish to review the patient after one week to inspect the surgical defect. This may require sedation as removal of the obturator may be painful. It also provides an opportunity to debride the defect with an antiseptic solution. Employing the double loop technique facilitates easy removal and re-attachment of the obturator. This must be repeated weekly by the dental team until the patient is able to remove and replace the obturator and cleanse the cavity using a syringe, if necessary. Routine oral hygiene instruction and monitoring forms an integral part of the aftercare management.
Post-surgical management
This is a key stage in the treatment of a patient with an orofacial surgical defect. It is generally composed of:
A physical aspect; and
A psychological aspect.
These are interdependent as a successful operation and obturation will produce a marked psychological advantage to the patient, in that his/her appearance, speech, ability to eat and drink are all satisfactory. The patient will accommodate to wearing the obturator over the next two months and both the physical and psychological aspect are fulfilled when their relatives visit and are unable to identify any significant disturbance in aesthetics or function. In these circumstances, the patient's ability to speak, eat and drink normally is of prime importance. Ocular prostheses retained by implants have revolutionized this aspect of rehabilitation. (Figure 8 a–d).
Figure 8. (a–c) Patient following left hemimaxillectomy awaiting ocular prosthesis. Note normal facial contours. (d) Patient restored with implant retained ocular prosthesis.
The intermediate hollow obturator
It is essential after the initial healing period of six to eight weeks that the immediate obturator is replaced by an intermediate hollow one. This is because the surgical tissues around the area of the incision will have partially healed and the immediate obturator will become loose and less effective. The aim of this procedure is to develop a stable and comfortable intermediate prosthesis re-establishing the fit, thus maintaining the intra-oral seal, retention and support of the facial tissues and providing continued normal oral functions. The intermediate obturator and the subsequent definitive obturator should be hollow in form to provide the patient with a lighter, more resonant and comfortable appliance. The laboratory technique originally used to form the obturator bulb was cumbersome, employing pumice and sand around which the wax, and ultimately the acrylic, were formed, so that the pumice and sand had to be washed out of the obturator. A new technique is now employed using a light-cured denture base material (Triad®).2,3
The immediate obturator is duplicated using a silicone mould and is carried out whilst the patient is in the clinic (Figure 9). The technique employs a wash impression of the defect on the immediate obturator, with a low viscosity silicone or polysulphide rubber impression material, which is duplicated to provide the base for a well-fitting intermediate obturator (Figure 10). In partially dentate patients it is necessary to record a locating impression with the partial obturator in situ. This must be accomplished within a one and a half hour appointment so that the new intermediate obturator is inserted before the healing mucosa of the cavity has time to contract and create any insertion problems.
Figure 9. Duplicate silicone moulds.Figure 10. Final wash impression in duplicate of the immediate obturator.
Choosing the duplication technique to provide a new master cast, the intermediate or definitive obturator may be constructed using the Triad® light-cured hollow obturator technique (Figure 11).
Figure 11. Immediate and intermediate obturators.
This procedure requires no special flasks but instead employs sections of 2 mm thick sheet of Triad® light-cured material, formed on a sectioned stone mould, which are joined on the master cast to provide an eggshell-like obturator which has the following advantages over conventional prostheses (Figure 12 a–c):
Figure 12.
(a) Sectioned stone mould. (b) Triad® sheets adapted to stone mould and light cured. (c) Completed Triad® hollow obturator.
Comfortable for patient;
Simple technique;
Versatility of technique;
Light weight;
Simple to adjust/repair;
Impermeable to oral fluids.
An assessment of a patient using or having been treated using the Triad® light-cured obturator indicated the following:4
Ease and repeatability of technique;
Versatility of technique;
A light, accurate smooth-surfaced obturator;
Ease of repair or addition;
Impermeablity to oral fluids;
Well tolerated.
Acquired mandibular defect
Squamous cell carcinomas of the floor of the mouth or the lateral borders of the tongue may also involve the alveolar ridge unilaterally.5,6,7 Surgery involves either local resection of bone and mucosa leaving a rim of mandible intact being replaced by a skin graft or, in more extensive lesions, a partial or hemimandiblectomy. In cases where a whole section of the mandible has been removed, a bone graft using free tissue transfer to restore mandibular continuity and function will normally be used for the rehabilitation. The occlusion and tongue mobility are restored in an effort to maintain post-operative oral function. If, however, the patient is edentulous or partly dentate, a removable prosthesis will be used to rehabilitate the missing alveolar ridge and teeth. This will be retained conventionally on the dentate segment and, where appropriate, stabilized and retained by implants on the affected side. The implants may either be inserted into the remaining intact mandible or into the graft. Implant-supported dental rehabilitation aids restoration of a functional mastication, facial aesthetics and support of the lower lip. As with the upper jaw, the partially dentate is much easier to rehabilitate than the edentulous mandible.
Forehead flap plastic surgery technique
In edentulous situations, or when bone graft rehabilitation is contra-indicated, a full thickness forehead graft may be rotated through the cheek on the affected side to restore the missing mucosa and the lingual pouch area (Figure 13). This will permit the prosthodontist to provide a retentive and stable conventional lower complete denture (Figure 14). However, this technique, when combined with the use of osseointegrated implants, will provide an even more stable rehabilitation for the patient.
Where a patient has had a partial mandiblectomy without immediate bone grafting, support for the cheek and occlusion may be provided by a swing-lock prosthesis (Figure 15a, b). Its superior retention provides a stable lower appliance which allows the soft tissues of the cheek to be maintained in their normal position prior to secondary surgery and stabilizes both the occlusion and remaining mandible.
Figure 15.
(a) Partial hemimandiblectomy patient without bone grafting. (b) Swing-lock prosthesis in situ.
Cranioplasty
During the seventies and eighties in Northern Ireland gunshot injures to the head and neck were common. This often caused trauma to the skull with resulting comminuted bone fracture, which subsequently had to be surgically removed. These defects and those secondary to congenital and pathological lesions required cranioplasty.
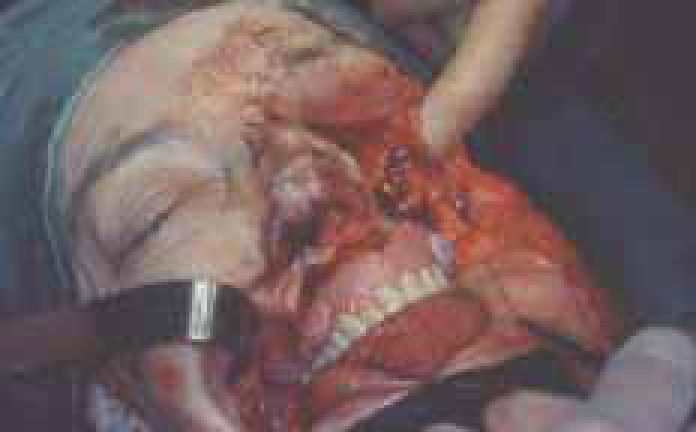
A new technique was developed at that time using titanium metal sheets to provide a cranioplasty.8 After the initial surgery had taken place to remove the comminuted cranial bone, the patient was referred to the prosthodontist, the surgical margins were shaved and the defect made good with silicone putty and an overall impression recorded in impression plaster (Figure 16a, b). A die was poured using this impression and a thin titanium plate was formed using a novel hydraulic technique, which has now become the technique of choice to form an accurately adapted titanium plate which is fixed to the bone using titanium screws around the periphery of the defect (Figure 17).
Figure 16.
(a) Post-operative cranial defect. (b) Impression of defect using silicone putty.Figure 17. Insertion of titanium cranioplasty.
Hence a titanium cranioplasty is screwed in place which forms a perfect cranial outline and restores aesthetics completely, protecting the underlying neural tissues (Figure 18). More recently, a new digital tomography technique has been used to assess the size and outline of the bony defect accurately.9 A die is formed from this computerized outline which gives an accurate base on which to form the titanium plate in the prosthetic laboratory. The cranioplasty service has for decades allowed many patients with both traumatic and pathological defects to assume a normal lifestyle.
Figure 18. Restored cranial contours.
Conclusion
Cancer of the orofacial region is relatively common and, if diagnosed early, patients should have a good outcome. For successful rehabilitation of the patient it is necessary to adhere to the following key principles:
Surgical maxillofacial management requires a skilled and experienced team.
Intimate understanding and co-operation between the team members.