
Article
Approaches to management of third molars in the UK has changed since the introduction of the NICE guidelines in 20001 and prophylactic removal of third molars has been mostly discontinued. Where removal is indicated, the risk of morbidity with the procedure, notably ID nerve damage, can be of concern to clinicians and patients alike.2
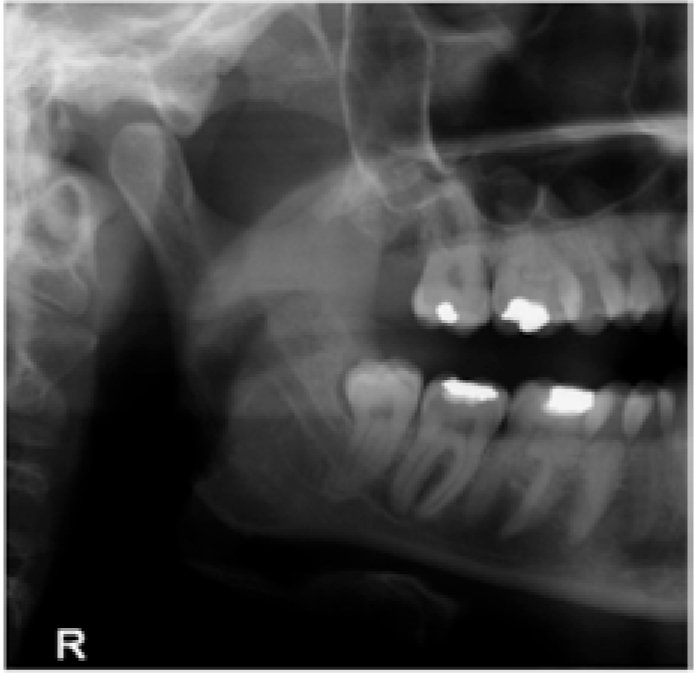
A 43-year-old female patient attended following a referral from her general dental practitioner for re-assessment of both lower third molars. The patient was previously seen in early 2012 regarding discomfort associated with these teeth which had both developed multiple episodes of pericoronitis. Figure 1 shows the position of LR8 and the high degree of risk of ID nerve damage which could have been present with extraction of this tooth. Coronectomy was proposed for LR8, however, owing to the absence of symptoms, the patient declined treatment.
At repeat presentation in late 2015, the patient reported that the lower right third molar had changed position and had ‘grown’ to be in an ‘awkward’ position. Clinical examination at repeat assessment identified that the lower right third molar had erupted considerably, to the extent that it was now an occlusal interference. Radiographs taken to assess the position of the tooth (Figure 2) in relation to the ID canal showed a considerable change from initial presentation (Figure 1); the tooth had moved to become a routine extraction with a reduced risk to the inferior dental nerve. The LR8 was removed with forceps and no alteration of sensation to the area supplied by the inferior dental nerve was reported.

Though multiple indications could lead a clinician to propose surgical intervention, this case suggests that, when risk of ID nerve damage is high, retention and monitoring over a longer period of time could be entirely appropriate, if the patient's oral hygiene is optimized and the tooth is not mesio-angular in orientation. In this scenario, caries development around the second molar is less likely and the potential morbidity associated with extraction was entirely avoided. It would generally be anticipated that a lower third molar would remain in its position with the risk of paraesthesia remaining if extraction were considered at a later date. This degree of movement of a third molar seems highly unusual and no reports of third molars erupting in this manner could be identified. Regardless of this case being isolated, clinicians must consider that, even if removal of a tooth complies with NICE guidelines, it may not be necessary to remove at that stage in the absence of symptoms. For motivated patients with good oral hygiene, monitoring should always be considered as a treatment option.