Markoski MM, Garavaglia J, Oliveira A Molecular properties of red wine compounds and cardiometabolic benefits. Nutr Metab Insights. 2016; 9:51-57 https://doi.org/10.4137/NMI.S32909
Liao Y, Tong XT, Jia Y The effects of alcohol drinking on oral microbiota in the Chinese population. Int J Environ Res Public Health. 2022; 19 https://doi.org/10.3390/ijerph19095729
Robinson J, Harding J. The Oxford Companion to Wine, 4th edn. Oxford: Oxford University Press; 2015
Rees J, Hughes J, Innes C. An in vitro assessment of the erosive potential of some white wines. Eur J Prosthodont Restor Dent. 2002; 10:37-42
Wiegand A, Attin T. Occupational dental erosion from exposure to acids: a review. Occup Med (Lond). 2007; 57:169-176 https://doi.org/10.1093/occmed/kql163
George R, Chell A, Chen B Dental erosion and dentinal sensitivity among professional wine tasters in South East Queensland, Australia. ScientificWorldJournal. 2014; 2014 https://doi.org/10.1155/2014/516975
Boyle C, Lane R. Toothsome but tricky for tasters. Surgeons' News. 2022; 76-77
Felix J, Ouanounou A. Dentin Hypersensitivity: etiology, diagnosis, and management. Compend Contin Educ Dent. 2019; 40:653-657
Goodacre CJ, Eugene Roberts W, Munoz CA. Noncarious cervical lesions: morphology and progression, prevalence, etiology, pathophysiology, and clinical guidelines for restoration. J Prosthodont. 2023; 32:e1-e18 https://doi.org/10.1111/jopr.13585
Uhlen MM, Mulic A, Holme B. The susceptibility to dental erosion differs among individuals. Caries Res. 2016; 50:117-123 https://doi.org/10.1159/000444400
Silva NC, Ventura TMO, Oliveira BP Proteomic profile of the acquired enamel pellicle of professional wine tasters with erosive tooth wear. Eur J Oral Sci. 2021; 129 https://doi.org/10.1111/eos.12779
Oral and dental problems may be considered to be an occupational hazard of winetasters and others in the wine trade. These oral and dental problems are reviewed. Advice to members of the wine trade to prevent occupational oral and dental problems is presented, together with views on the management of such problems.
CPD/Clinical Relevance: Oral and dental conditions may be an occupational hazard among winetasters and others in the wine trade.
Article
The aim of this article is to provide an overview of the cause, presentation, prevention and management of oral and dental problems experienced by wine tasters and others in the wine trade.
Wine, an alcoholic beverage made from fermented grape juice, has been produced for thousands of years. Some of the earliest evidence of wine is from the Caucasus region in today's Georgia dating back to between 6000 and 5000 BC.1 Wine, apart from its use for personal consumption, has, among other things, long played an important role in religion2 and been considered to have both positive and negative health effects, largely depending on the amount consumed.3
Any one type of wine comprises several hundred compounds, many at very low concentrations. The major components of wine are, in general, water (86%); ethanol (12%); glycerol, polysaccharides, phenolic compounds and trace elements (1%); different types of acid (0.5%); and a variety of volatile compounds (0.5%). Many of these components have positive and negative effects on body organs, systems, cells, molecular mechanisms and commensals,4 including the oral microbiome.5 The pH of wine is largely between 3 and 4,6 as confirmed in a number of publications on the erosive potential of wines, for example, Rees et al.7
Globally, the wine business is huge (annual value of over US$300bn in 2022), with many different types, styles, varieties and vintages of wine. This market is expected to grow annually by >5%.8
Wine tasters
Professional wine tasters have existed since the 4th century BC,9 together with others in the wine trade, including producers, buyers, merchants and sommeliers, all of whom may taste many different wines in the process of going about their daily business: tasting, unlike wine drinking, involves swirling the wine around the oral cavity, while inhaling air to aerate the wine, subsequent to assessing the appearance (intensity and colour) and ‘nose’ (intensity and aroma characteristics) of the wine.10 While the number of wines tasted during the working day by individuals in different roles in the wine trade may vary widely, the number may, at least on occasion, be very large. For example, Liberty Wines, one of the largest wine companies in the UK, selling to retailers, restaurants and bars, holds a twice-yearly wine tasting in central London. In January 2023, they showcased circa 800 wines from over 300 producers to approximately 1000 customers. While it is unlikely that any delegates tasted all the wines showcased, it is possible that some delegates tasted up to 200 different winesd in a day. A further aspect of tasting is that it may be limited to certain times of the day, with, it is assumed, relatively short, well-spaced-out sessions posing less of a risk to the teeth and oral mucosa than long, protracted sessions, with brief breaks between sessions.
Oral and dental effects
The common oral and dental effects of wine tasting include pathological, mainly erosive tooth wear (Figure 1), dentine hypersensitivity and staining. Also, there may be changes to the oral mucosa and oral microbiome,5 with an increased risk of, among other conditions, oral cancer.11 The presentation of these conditions may be complex (Figure 1) and highly variable, specifically in the presence of, for example, smoking or other tobacco use, bruxism or gastro-oesophageal reflux disease (GORD). There is no evidence of a typical, let alone diagnostic presentation of the oral effects of wine tasting. Also, there are no data available on BEWE (Basic Erosive Wear Examination) scores in winetasters and others in the wine trade, let alone data on the incidence and severity of the other oral and dental effects reported.
Figure 1. Maxillary arch of a mature adult, male patient who had held various positions in a lifelong career in the wine trade. The erosion of the remaining tooth tissues, leaving margins of the amalgam restorations with positive ledges, and causing exposure of the pulp in the upper right canine – the reason for the patient seeking emergency dental care – was considered to have been aggravated by bruxism, linked to occlusal interferences, and gastro-oesophageal reflux disease (GORD) believed to be associated with chronic, high levels of alcohol consumption. Also, the patient had a passion for smoking cheroots when not wine tasting.
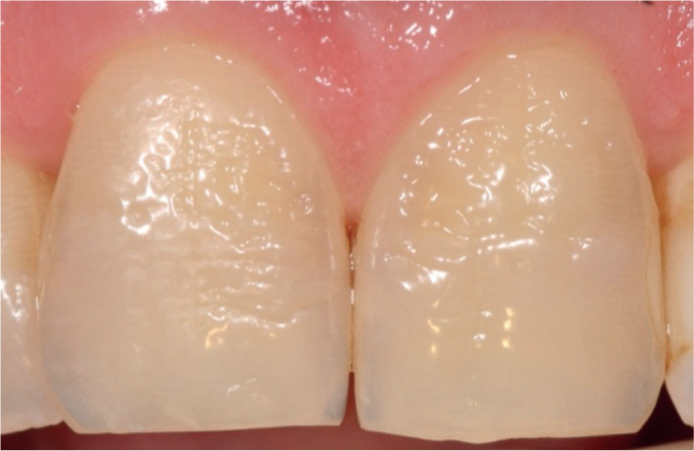
Pathological erosive tooth wear has been reported and commented on in wine tasters and others in the wine trade, by a number of authors.12,13,14,15,16,17,18 These reports confirm the highly variable presenting signs and symptoms of the condition. Also, these reports lend support to the anecdotal information that many individuals working in the wine trade experience dentine hypersensitivity – another condition that tends to have a complex, multifactorial aetiology,19 specifically if associated with non-carious cervical lesions (NCCLs) (Figure 2), which have complex aetiologies also,20 or atypical tooth surface loss of uncertain origin (Figure 3).
Figure 2. Non-carious cervical lesions in teeth with dentine hypersensitivity in a wine taster. Courtesy of Professor Andrew Eder.Figure 3. Atypical tooth surface loss of uncertain origin giving rise to hypersensitivity in the upper central incisors of a wine taster. Courtesy of Professor Andrew Eder
Susceptibility to pathological erosive tooth wear and dentine hypersensitivity among wine tasters and others in the wine trade would, however, appear to vary, with 30–50% not developing clinically significant erosive wear or dentine hypersensitivity.21 This variation in susceptibility, which, in the case of erosive tooth wear, has been described as a ‘classic gene-environmental model’22 may, among other things, be associated with differences in acquired enamel pellicle proteomic profiles,22 or minimal acidic challenge being able to cause damage to the hard tooth tissues in certain individuals.21
Staining may occur in winetasters, specifically if oral hygiene is not well maintained. Extrinsic staining, specifically staining of calculus and other deposits on teeth is normally readily managed, and recurrence largely prevented by achieving and maintaining a good standard of oral hygiene. Imperfect margins in tooth-coloured direct and indirect restorations and surfaces of resin composite and glass-ionomer restorations lacking good finish may be susceptible to wine-related staining, as may teeth that have suffered some surface damage from, for example, non-proprietary tooth bleaching agents. Such staining, which may be difficult to manage, may encourage excessive, inappropriate brushing, which, according to the Australian Wine Research Institute, may cause ‘premature gum recession.’23
Changes to the oral mucosa, if any, may vary from different forms and extents of desquamation or keratinization to, in exceptional cases, pre-cancerous and cancerous lesions.5,11 As with the anecdotal reporting of a high incidence of dentine hypersensitivity among those in the wine trade, there is anecdotal reporting of problems with oral mucosa. Such problems, some of which may be unrelated to wine tasting, may be aggravated by, for example, wine tannin or other forms of xerostomia, which compromise a wine taster's discrimination, and smoking, or other tobacco use which dulls a taster's ‘palate’ and ‘nose’.
Advice
The Australian Wine Research Institute provides detailed guidance for wine tasters and wine judges.24. Included in this guidance is the following abridged summary of preventive steps to reduce ‘tooth erosion and sensitivity’, compiled by the University of Adelaide Dental School.
Night before tasting
Brush teeth with a readily available fluoride toothpaste (1000 mg/L fluoride).
Apply by toothbrush a 1.5-cm GC Dental ToothMousse (casein phosphopeptide-amorphous calcium phosphate; GC Corporation, Tokyo, Japan) or high concentration sodium fluoride toothpaste and leave for 4 minutes (alternately use a custom-made dental tray). Spit out and avoid drinking for 1 hour.
Morning of tasting
Do not brush teeth the morning before tasting.
Apply 1.5 cm of GC Dental ToothMousse with your finger and leave for 4 minutes. Spit out and do not rinse.
During tasting
Drink still water to rinse mouth.
Eat cheese or drink milk.
Eat (plain) crackers to stimulate saliva production.
After tasting
Do not brush teeth for at least 2 hours after tasting.
Wash mouth with 0.2% fluoride mouth rinse. Spit (don't rinse) after 2 minutes.
Chew GC Dental Recaldent (calcium phosphopeptide; GC Corporation, Tokyo, Japan) or sugar-free gum to help stimulate saliva production.
In addition, it is advised that ‘longer-term preventive strategies include visiting a dentist at least once per year and having a preventive plan in place. Annual topical fluoride applications are also recommended.’
The authors of the present paper would add to this advice the need to carefully and systematically examine all aspects of the oral mucosa as part of the recommended annual recall, with instructions to seek an urgent appointment if any oral lesion develops and persists for more than 2 weeks.
In addition to the above, it is suggested that individuals planning to enter the wine trade, specifically those who have not been regular dental attenders, should be advised to make arrangements to optimise their oral and dental health. Individuals entering the wine trade with a previous history of pathological tooth wear and dentine hypersensitivity, or who have received extensive, let alone complex restorative care, including multiple restorations with margins that may be prone to staining or other deterioration when subjected to multiple exposes to acidic wine on a daily basis, may benefit from careful counselling to fully understand the potential negative oral and dental effects of their chosen trade.
Management
Wine tasters and others in the wine trade presenting with pathological erosive tooth wear, with or without dentine involvement, should, it is suggested, following any immediate palliative care and detailed consideration of possible non-wine-tasting causes of their oral and dental problems, be advised to adopt the Australian Wine Research Institute guidance, as set out above. Such patients should subsequently be reviewed, possibly initially after 1 month and at 3-monthly intervals thereafter. Where operative intervention is considered to be indicated, having controlled the erosive and related processes, state-of-the-art approaches to the management of dentine hypersensitivity and tooth wear19,25s should be adopted, subject to the informed consent of the patient.
Conclusion
It is suggested that, apart from providing an overview of the cause, presentation, prevention and management of oral and dental problems experienced by wine tasters and others in the wine trade, the present review reinforces the importance of taking a detailed social history from all patients. Failure to ascertain that a patient presenting with pathological erosive tooth wear and possibly associated dentine hypersensitivity is a wine taster or otherwise engaged in the wine trade, could lead to misdiagnosis, mismanagement, prolonged suffering by the patient, and unnecessary progression of oral and dental disease, with all the associated consequences. As stressed to students and trainees at all levels, ‘knowing your patients’ is an important aspect of effective oral healthcare care.