Arankalle VA, Chobe LP. Retrospective analysis of blood transfusion recipients: evidence for post-transfusion hepatitis E. Vox Sang. 2000; 79:72-74
Deuffic-Burban S, Delarocque-Astagneau E, Abiteboul D Blood-borne viruses in health care workers: prevention and management. J Clin Virol. 2011; 52:4-10
Pruss-Ustun A, Rapiti E, Hutin Y. Estimation of the global burden of disease attributable to contaminated sharps injuries among health-care workers. Am J Ind Med. 2005; 48:482-490
Werner BG, Grady GF. Accidental hepatitis-B-surface-antigen-positive inoculations. Use of e antigen to estimate infectivity. Ann Intern Med. 1982; 97:367-369
Komatsu H, Inui A, Sogo T Tears from children with chronic hepatitis B virus (HBV) infection are infectious vehicles of HBV transmission: experimental transmission of HBV by tears, using mice with chimeric human livers. J Infect Dis. 2012; 206:478-485
Petersen NJ, Bond WW, Favero MS. Air sampling for hepatitis B surface antigen in a dental operatory. J Am Dent Assoc. 1979; 99:465-467
Kew MC. Possible transmission of serum (Australia-antigen-positive) hepatitis via the conjunctiva. Infect Immun. 1973; 7:823-824
Fattovich G, Bortolotti F, Donato F. Natural history of chronic hepatitis B: special emphasis on disease progression and prognostic factors. J Hepatol. 2008; 48:335-352
Puro V, De Carli G, Cicalini S European recommendations for the management of healthcare workers occupationally exposed to hepatitis B virus and hepatitis C virus. Euro Surveill. 2005; 10:260-264
Zuckerman JN. Protective efficacy, immunotherapeutic potential, and safety of hepatitis B vaccines. J Med Virol. 2006; 78:169-177
Struve J, Aronsson B, Frenning B Seroconversion after additional vaccine doses to non-responders to three doses of intradermally or intramuscularly administered recombinant hepatitis B vaccine. Scand J Infect Dis. 1994; 26:468-470
Kubba AK, Taylor P, Graneek B, Strobel S. Non-responders to hepatitis B vaccination: a review. Commun Dis Public Health. 2003; 6:106-112
Pfaender S, von Hahn T, Steinmann J prevention strategies for blood-borne viruses-in the era of vaccines, direct acting antivirals and antiretroviral therapy. Rev Med Virol. 2016; 26:330-339
Huang DQ, Lim SG. Hepatitis B: who to treat? A critical review of international guidelines. Liver Int. 2020; 40:5-14
UK Health Security Agency. Integrated guidance on health clearance of healthcare workers and the management of healthcare workers infected with bloodborne viruses (hepatitis B, hepatitis C and HIV). https://tinyurl.com/2p8rsncb (accessed December 2021)
Lampertico P, Agarwal K, Berg T EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J Hepatol. 2017; 67:370-398
Westin J, Aleman S, Castedal M Management of hepatitis B virus infection, updated Swedish guidelines. Infect Dis (Lond). 2020; 52:1-22
Choo QL, Kuo G, Weiner AJ Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science. 1989; 244:359-362
Smith BD, Beckett GA, Yartel A Previous exposure to HCV among persons born during 1945-1965: prevalence and predictors, United States, 1999–2008. Am J Public Health. 2014; 104:474-481
Nainan OV, Alter MJ, Kruszon-Moran D Hepatitis C virus genotypes and viral concentrations in participants of a general population survey in the United States. Gastroenterology. 2006; 131:478-484
Kemp L, Clare KE, Brennan PN, Dillon JF. New horizons in hepatitis B and C in the older adult. Age Ageing. 2019; 48:32-37
Pradat P, Voirin N, Tillmann HL Progression to cirrhosis in hepatitis C patients: an age-dependent process. Liver Int. 2007; 27:335-339
Tong MJ, el-Farra NS, Reikes AR, Co RL. Clinical outcomes after transfusion-associated hepatitis C. N Engl J Med. 1995; 332:1463-1466
Kallwitz ER, Layden-Almer J, Dhamija M Ethnicity and body mass index are associated with hepatitis C presentation and progression. Clin Gastroenterol Hepatol. 2010; 8:72-78
Poynard T, Ratziu V, Charlotte F Rates and risk factors of liver fibrosis progression in patients with chronic hepatitis C. J Hepatol. 2001; 34:730-739
Åberg F, Helenius-Hietala J, Meurman J, Isoniemi H. Association between dental infections and the clinical course of chronic liver disease. Hepatology Res. 2014; 44:349-353
Guggenheimer J, Eghtesad B, Close JM Dental health status of liver transplant candidates. Liver Transpl. 2007; 13:280-286
Cruz-Pamplona M, Margaix-Munoz M, Sarrion-Perez MG. Dental considerations in patients with liver disease. J Clin Exp Dent. 2011; 3:e127-e134
Dwyer JP, Jayasekera C, Nicoll A. Analgesia for the cirrhotic patient: a literature review and recommendations. J Gastroenterol Hepatol. 2014; 29:1356-1360
Chandok N, Watt KD. Pain management in the cirrhotic patient: the clinical challenge. Mayo Clin Proc. 2010; 85:451-458
Lewis JH, Stine JG. Review article: prescribing medications in patients with cirrhosis – a practical guide. Aliment Pharmacol Ther. 2013; 37:1132-1156
Andrade RJ, Tulkens PM. Hepatic safety of antibiotics used in primary care. J Antimicrob Chemother. 2011; 66:1431-1446
Helenius-Hietala J, Meurman JH, Hockerstedt K Effect of the aetiology and severity of liver disease on oral health and dental treatment prior to transplantation. Transpl Int. 2012; 25:158-165
Shah NL, Caldwell SH. Assessing the risk of bleeding and clotting in cirrhosis. Clin Liver Dis (Hoboken). 2016; 7:26-28
Flores B, Trivedi HD, Robson SC, Bonder A. Hemostasis, bleeding and thrombosis in liver disease. J Transl Sci. 2017;
Tripodi A, Primignani M, Chantarangkul V Thrombin generation in patients with cirrhosis: the role of platelets. Hepatology. 2006; 44:440-445
Hong CH, Scobey MW, Napenas JJ Dental postoperative bleeding complications in patients with suspected and documented liver disease. Oral Dis. 2012; 18:661-666
Hepatitis B, Hepatitis C and Liver Disease: A Review for the Dental Practitioner Iain Macpherson Paul N Brennan John F Dillon Dental Update 2024 49:1, 707-709.
Authors
IainMacpherson
MBChB, MRCP(UK)
Clinical Research Fellow, Division of Clinical and Molecular Medicine, University of Dundee, Ninewells Hospital and Medical School, Dundee
Professor of Gastroenterology and Hepatology, Division of Clinical and Molecular Medicine, University of Dundee, Ninewells Hospital and Medical School, Dundee
The prevalence of chronic liver disease continues to rise, and important causes include viral infections, such as hepatitis B and hepatitis C. Both of these viruses can be contracted by healthcare workers through an inoculation injury and can lead to liver cirrhosis and cancer. In addition, chronic liver disease can result in disorders of liver function, including coagulopathy and abnormal metabolism of drugs widely used in dentistry. This article reviews current prevalence, transmission rates and treatment of hepatitis B and hepatitis C, as well as particular considerations for dental patients with liver disease.
CPD/Clinical Relevance: Viral hepatitis remains a risk to all healthcare workers, and patients with liver disease provide various challenges when providing dental treatment.
Article
Blood borne viruses (BBVs) are transmitted through the transfer of blood or other virus-containing bodily fluids between individuals. Hepatitis B virus (HBV), hepatitis C virus (HCV) and human immunodeficiency virus (HIV) account for the majority of such infections, while there is evidence that hepatitis E virus (HEV), usually transmitted through the faecal–oral route, can also be transmitted through blood to blood transfer.1,2
Globally, healthcare workers (HCWs), including dentists, are at risk of contracting such infections. Routes of transmission include inoculation injury, and blood or saliva entry through a wound. In 2000, it was estimated that HCWs contracted 66,000 HBV and 16,000 HCV infections through percutaneous injuries (PIs).3
HBV, HCV and HEV often result in acute, self-limiting illnesses, but can lead to chronic infection, resulting in chronic inflammation of the liver (hepatitis). Chronic viral hepatitis can cause liver fibrosis, cirrhosis, and hepatocellular carcinoma (HCC), and in some countries is the leading cause of liver transplantation.4
The incidence and prevalence of chronic liver disease (CLD) has been rising over the past few decades. Globally, liver disease results in 2 million deaths per year, as a result of liver cirrhosis (around 1 million) and viral hepatitis and HCC (around 1 million).5 This is likely to be a significant underestimate, given the lack of accurate mortality information in many developing countries, including those in which there is a significant burden of viral hepatitis. The Scottish Public Health Observatory (ScotPHO) estimates liver disease accounted for 16.3 deaths per 100,000 population in Scotland in 2018.6 Liver disease is the leading cause of death in the 35–49-year-old age group, and the third leading cause of death in under 65s.7 Deaths from HCC have risen by two-thirds in the past decade, and HCC now ranks as the ninth most common cancer death, occurring almost exclusively in patients with chronic liver disease.
The most frequent causes of liver disease in the UK are non-alcoholic fatty liver disease (NAFLD), alcohol-related liver disease (ARLD), and viral hepatitis, accounting for 90% of CLD. All are preventable, and chronic HCV is curable. It is estimated around one-third of adults in the UK have the early stages of NAFLD.
Advanced disease results in dysfunction of the liver. Blood clotting factor production can be reduced, primarily due to inability of the liver to make the factors, and secondarily due to the reduced absorption of vitamin K because of reduced bile production. Portal hypertension can result in thrombocytopenia due to increased platelet scavenging. Both of these issues can result in an excessive tendency to bleed. In addition, the diseased liver may struggle to metabolize a range of commonly prescribed antibiotics and analgesia.
Hepatitis B virus
HBV was identified in 1963 with the discovery of the ‘Australia antigen’ (now called surface antigen).8 It is a member of the Hepadnaviridae and is made up of a complex viron, involving double stranded-DNA capable of reverse transcription.9
The global prevalence of HBV is variable. In the WHO Western Pacific Region, the prevalence is highest, at 6.2%.The WHO European Region has a prevalence of 1.6%.10 Specifically, the UK is among the lowest affected countries, with an infection rate of 0.1–0.5%.11
HBV is contracted when contaminated body fluids, such as blood or saliva, penetrate the mucous membranes. As such, HCWs are at increased risk of transmission from inoculation injuries and blood splashes onto mucous membranes. The risk of transmission to non-vaccinated HCWs is 22–31% from an injury involving a hollow-bore needle.12 HBV has also been shown to be transmitted through the tears of an individual with HBV. HBV DNA is detectable in the saliva of those with HBV,13 suggesting the potential for transmission via saliva should be an important consideration for dental practitioners. There are no documented incidences of the spread of HBV, or any blood-borne pathogen, via aerosol droplets, such as those generated during clinical procedures. In particular, it has been shown that hepatitis B surface antigen is not detected in the air during procedures involving patients with HBV.14 However, transmission of HBV has been suspected via blood splatter onto conjunctivae, and so eye protection remains important during dental treatment.15 Other routes of transmission include needle-sharing in people who inject drugs (PWIDs), vertical transmission from mother to child during pregnancy and childbirth and sexual contact.
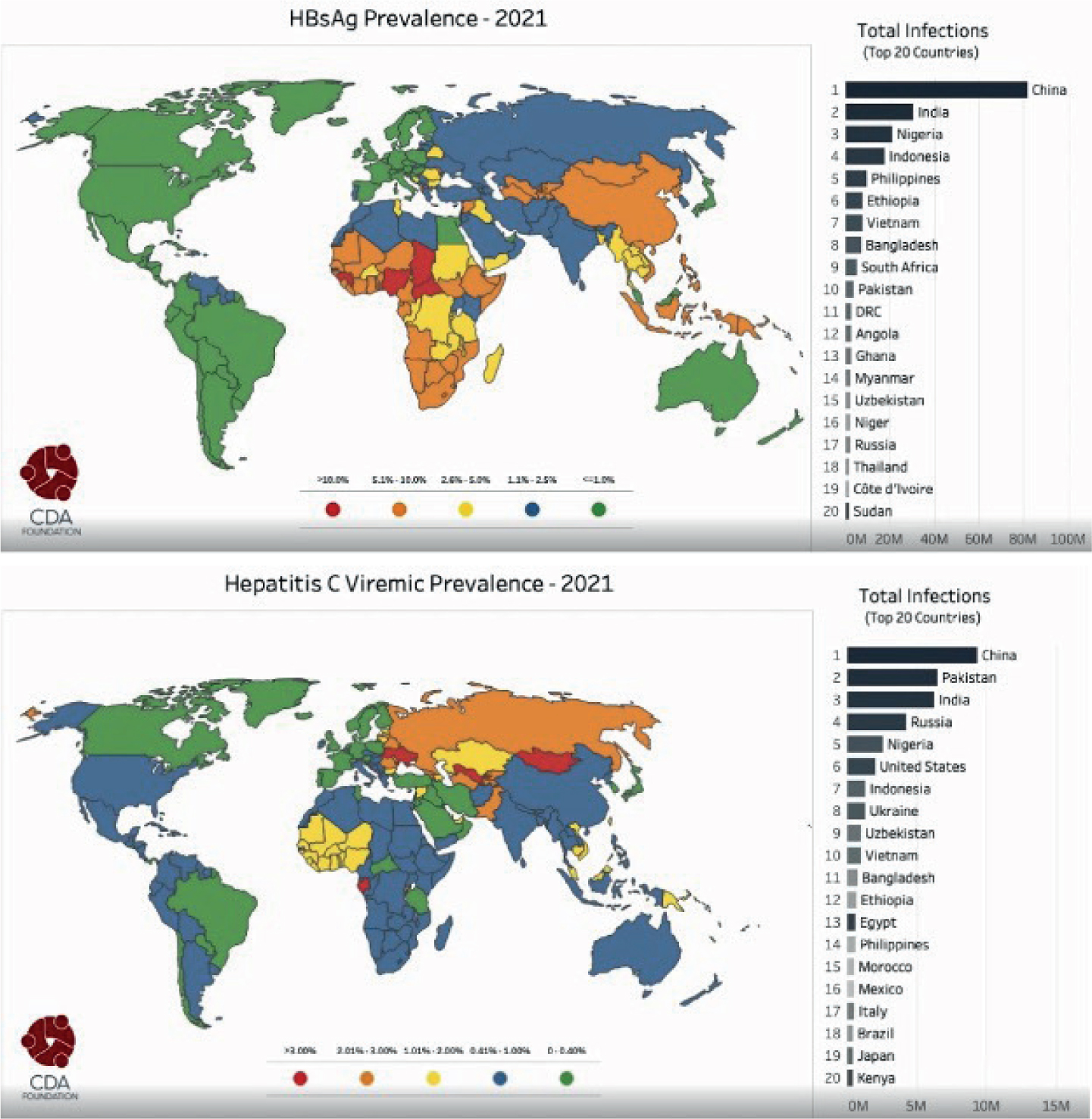
Figure 1. Forecast global prevalence of hepatitis C virus and hepatitis B virus in 2021.55
Historically, the performance of exposure-prone procedures (EPPs) came with such a high risk of contracting HBV that most HCWs showed markers of either previous or current infection after a few decades of professional practice, with oral surgeons having the highest prevalence.8
The majority of adults who acquire HBV experience an acute, flu-like illness, or have no symptoms at all. Approximately 95% of adults clear the infection during the acute phase, with only 5% progressing to chronic hepatitis.16 Infants and children are at a greater risk of developing chronic infection. Globally, around 240 million people have a chronic infection and there are approximately 780,000 HBV-related deaths annually.10
HBV vaccination has been offered to all children as part of the UK vaccination schedule since 2017, as part of the ‘6-in-1’ vaccine, and is particularly recommended for babies born to infected mothers.17 Uptake of this vaccine is over 96% in Scotland and 93.1% in England.18,19
European guidelines recommend vaccinating all HCWs in contact with patients, blood or other body secretions.20 Vaccination is recommended early in the career, ideally before commencing training, as is commonplace across the UK. However, 5–10% of healthy adults fail to develop an antibody response to the vaccine.21 As a result, follow up blood tests are required to check for response, followed by booster doses of the vaccine, where necessary.22 Risk factors for non-response include male sex, obesity, smoking, and older age.23 Non-responders are at risk of developing HBV infection and should be regularly screened.2
In all cases of accidental contact with blood or body fluid from a patient known or suspected to have HBV, the source patient should be tested and the HCW should have baseline HBV serology performed. Post-exposure prophylaxis (PEP) for HCWs exposed to HBV depends on vaccination and response status. HCWs with full vaccination and known serological response do not require follow up or PEP.2 In vaccination non-responders, PEP with HBV vaccine and HBV immunoglobulin should be given as soon as possible, no later than 1 week after and ideally within 24 hours of exposure.24
HBV treatment has improved significantly. No treatment is necessary for acute infection, given the high proportion of patients who clear the virus spontaneously. The aim of chronic HBV treatment is to reduce viral load, in turn reducing viral transmission and reducing the rate of progression to advanced liver disease and HCC.25
There are two branches of treatment for chronic HBV: immunological and pharmacological. Treatment is generally recommended for individuals at high risk of disease progression, namely those with high alanine aminotransferase (ALT) levels, active viral replication and advanced fibrosis or cirrhosis.26 Dentists have an occupational requirement to have an HBV viral load of under 200 IU/ml and be HBV e antigen negative.27
The most potent pharmacological drugs are the nucleoside analogues (NAs), tenofovir and entecavir.28 These have a low side effect profile, come in a once-daily tablet form, and are safe even in renal failure. Both drugs are now off-patent and widely available. However, they do not cure HBV, meaning most patients must receive life-long treatment. Immunological treatment with interferon is poorly tolerated with high side effects. However, a sustained virological response is seen in around 30% of patients after 48 weeks of treatment, meaning life-long medication is not required.29
Hepatitis C virus
HCV is a positive-stranded RNA virus, distantly related to the Flaviviridae family.30 Similar to HBV, HCV is an important cause of chronic liver disease and can eventually result in liver cirrhosis and HCC. HCV is classified into six genotypes, with more than 50 further subtypes. In addition, the virus has a highly variable envelope protein, allowing evasion of traditional vaccine components, making vaccine development difficult.31
Worldwide, approximately 71 million people have chronic HCV infection,31 with a yearly incidence of 3–4 million cases. In Europe, prevalence is higher in the south and east, for example prevalence in Belgium and Ireland is 0.1%, but 3.2% and 5.9% in Romania and Italy, respectively.32
In the USA, 80% of individuals with HCV were born during the ‘baby boom’ years (1946–1964) and are five times more likely to have chronic infection than other adults. This cohort was most likely to have acquired HCV between the 1960s and 1980s,33 during an era of novel pathways of HCV transfer via recreational drug use and a lack of knowledge in BBV prevention.
Acute HCV is usually asymptomatic or involves mild constitutional symptoms.34 A small proportion of patients may present with hepatitis or jaundice. After 8 weeks, seroconversion and development of non-protective antibodies occurs. A small percentage of patients (5–20%) spontaneously clear the virus, but the remainder go on to develop chronic infection. This mechanism is not understood, but is most likely to be multifactorial.
Chronic HCV is defined as the persistence of HCV RNA for 6 months after an acute infection. The often asymptomatic nature of HCV can allow significant hepatocellular destruction before diagnosis. Approximately 25–35% of patients with chronic HCV progress to liver fibrosis, cirrhosis and hepatocellular carcinoma, while 1–2% will develop extrahepatic manifestations, such as cryoglobulinemia, membranoproliferative glomerulonephritis and vitiligo.35 Therefore, it is imperative that cases are identified early and treated.
Approximately 10–20% of patients with progressive HCV will develop significant hepatitis in 5–10 years with cirrhosis evolving in 10–20 years and hepatocellular carcinoma after 20–30 years. Prolonged infection with HCV predicts progression to cirrhosis36 and consequently increased HCC risk.37 Early studies have suggested patients under the age of 30 are unlikely to have significant fibrosis or cirrhosis in the absence of an additional predisposing hepatotoxic insult.32 Risk factors for progression to CLD include alcohol consumption (>40 g ethanol/day), older age at time of infection, male gender, HIV/HBV co-infection and BMI >25.36,38,39
Transmission of HCV is predominantly by percutaneous exposure to infected blood, such as intravenous drug use. Other modalities include inadequate sterilization and re-use of medical equipment,35 sexual transmission, and vertical transmission. Prior to 1992, blood transfusion was the predominant cause of hepatitis C.40
HCV diagnosis is achieved by serological testing for anti-HCV antibodies. Antibody-positive individuals then undergo a nucleic acid test for HCV RNA. This determines whether there is active infection, or if the patient has achieved a sustained virological response, through spontaneous clearance or drug treatment. Genotype analysis can guide treatment. After the diagnosis is established, patients undergo assessment for CLD.
There have been enormous advances in the treatment of HCV, which is now curable, thanks to a number of pan-genotypic drugs that have revolutionized response rates and induction of a sustained virological response. There is a diminishing role for the use of treatments, such as pegylated interferon and ribavirin, although some circumstances where they may be used remain.
There is a range of direct-acting antivirals available to treat chronic HCV, given in combination to maximize effect and reduce resistance development. Drug choice is guided by previous treatments and the presence or absence of established cirrhosis, but cure rates in excess of 97% with first-line treatment for 8–12 weeks is the norm.41
Liver disease considerations for the dentist
Patients with CLD are immunocompromised and may have a higher bleeding risk, so should undergo regular dental check-ups to reduce the need for invasive treatments, extraction in particular.42 Additionally, patients with CLD are often prescribed diuretics. These cause hyposalivation and increase the risk of gingivitis, dental caries, and oral candidosis.43
However, liver dysfunction can result in impaired drug metabolism, abnormal haemostasis, and a higher risk of post-treatment infection.44
Drugs, such as antibiotics and sedatives, can potentially cause side effects in cirrhotic patients due to impaired metabolism. Patients with well-compensated liver disease can metabolize drugs similar to the general population; however, those with advanced or decompensated disease may require lower and less-frequent doses, particularly of analgesia.45 Drug toxicity can cause hepatic decompensation, resulting in encephalopathy, gastrointestinal bleeding, and hepato-renal syndrome.46
Paracetamol is tolerated in doses of up to 4 g per day, and is recommended as first line analgesia in patients with liver disease.46,47 However, non-steroidal anti-inflammatory drugs (NSAIDs) should be avoided, as their direct antiplatelet action increases bleeding risk, especially in patients with thrombocytopenia and oesophageal varices or portal hypertension.46 Furthermore, the reduced level of serum proteins found in liver disease means the drug exists in higher quantities, which can result in hepatotoxicity and renal failure.45
Opioids should be used with caution. A common side effect is constipation, which can cause hepatic encephalopathy. If prescribed opioids, patients should be co-prescribed laxatives.
Penicillins are considered safe in CLD, with low risk of hepatotoxicity, but clavulanic acid is associated with a significant risk of drug-induced liver injury.48 As a result, and also because of its association with Clostridium difficile infection, antibiotics such as amoxicillin–clavulanic acid should be avoided. Other antibiotics associated with liver toxicity include macrolides, although clindamycin is recommended for surgical prophylaxis in cirrhotic patients.42,49 Metronidazole is safe in liver disease, but its interaction with alcohol may need review in patients with ARLD to prevent side effects or non-compliance.
Haemostasis disorders can occur in patients with CLD as a result of reduced coagulation factor production in the liver and reduced numbers of platelets due to splenic sequestration in portal hypertension.
The haemostatic capability of a cirrhotic patient should be assessed prior to dental interventions using a full blood count (FBC) to review the platelet count, and a coagulation profile to review prothrombin time (PT) and/or international normalized ratio (INR).
A prolonged PT and/or INR alone does not indicate an increased risk of bleeding for a patient with liver disease, and is an inadequate measure of coagulation ability in these patients.50 The ability of clot formation in patients with liver disease is a complex mechanism, which depends on other factors such as protein C and the levels of individual coagulation factors.51
Conversely, a platelet count of <50 x 109/L is associated with increased risk of bleeding, particularly when found in conjunction with an elevated PT and/or INR.52 Routine dental procedures are safe in patients with a platelet count of >50 x 109/L, and a count of >100 x 109/L should be considered safe in surgical dental procedures that carry a higher bleeding risk, such as multiple extractions or bone surgery.53
It is recommended that the patient's general practitioner or specialist are consulted about the risk of bleeding and, if necessary, procedures may have to be performed in a hospital environment.54
Conclusion
As the prevalence of chronic liver disease rises, the need for up-to-date knowledge relevant to the dental management of such patients becomes more important.
HBV and HCV are important causes of chronic liver disease, and the risk of transmission from patient to dentist is very much a reality. All HCWs should be vaccinated against HBV and be aware of the local protocols for post-exposure prophylaxis and management of inoculation injuries. HBV progresses to chronic infection in only 5% of adults, but those patients may require treatment to prevent progression to cirrhosis and hepatocellular carcinoma. HCV is now curable.
The management of patients with advanced liver disease in the dental surgery requires thought and consideration, specifically regarding drug metabolism and haemostasis. Safety and efficacy are the key backbones to any prescriber's practice, in particular with antibiotics and analgesia, in these patients. Blood coagulation profiles alone do not indicate the risk of bleeding in cirrhotic patients. However, platelet count is a better indicator of bleeding risk and specialist advice should be sought regarding abnormalities in these complex medical patients.