Marcenes W, Kassebaum NJ, Bernabé E, Flaxman A, Naghavi M, Lopez A, Murray CJ. Global burden of oral conditions in 1990–2010: a systematic analysis. J Dent Res. 2013; 92:592-597
Freeman R. The psychology of dental patient care: strategies for motivating the non-compliant patient. Br Dent J. 1999; 187:307-312
Rosenstock IM. Historical origins of the health belief model. Health Edu Monogr. 1974; 2:328-335
Hochbaum G.Washington DC: Public Health Service Publication; 1958
Conner M, Norman P., 3rd edn. England, UK: Open University Press; 2015
Rogers R. A protection motivation theory of fear appeals and attitude change. J Psychol. 1975; 91:3-114
Ajzen I. The theory of planned behaviour. Organ Behav Hum Dec. 1991; 50:179-211
Fishbein M, Ajzen I.Reading, MA: Addison-Wesley; 1975
Ogden J., 4th edn. England, UK: Open University Press; 2007
Bandura A.NJ, USA: Prentice-Hall Inc; 1986
Prochaska J, DiClemente C. Stages and processes of self-change in smoking: toward an integrative model of change. J Consult Clin Psychol. 1983; 51:390-395
Chapple ILC, Hill K. Getting the message across to periodontitis patients: the role of personalised biofeedback. Int Dent J. 2008; 58:(S5)294-306
, 3rd edn. : Public Health England; 2014
Oral Health Promotion: General Dental Practice. 2015;
Tonetti MS, Chapple IL Biological approaches to the development of novel periodontal therapies – consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol. 2011; 38:114-118
Miller WR, Rollnick S., 3rd edn. New York: Guilford Press; 2013
Wilson GT, Schlam TR. The transtheoretical model and motivational interviewing in the treatment of eating and weight disorders. Clin Psychol Rev. 2004; 24:361-378
Bundy C. Changing behaviour: using motivational interviewing techniques. J R Soc Med. 2004; 97:43-47
Rollnick S, Miller WR. What is motivational interviewing?. Behav Cogn Psychoth. 1995; 23:325-334
Rubak S, Sandbaek A, Lauritzen T, Christensen B. Motivational interviewing: a systematic review and meta-analysis. Br J Gen Pract: the journal of the Royal College of General Practitioners. 2005; 55:(513)305-312
Providing dietary advice to our patients forms the cornerstone of prevention for many dental diseases. However, simply prescribing information is unlikely to bring about long-term behavioural change. This article explores the theory of health behaviour as well as ways in which we can ‘get the message across’.
CPD/Clinical Relevance: Prescriptive approaches to behaviour changes can be considered inconsistent and ineffective. This article explores more patient-centred methods of inducing behaviour change with regard to dietary advice in the general dental practice setting.
Article
Oral disorders affect 3.9 billion people worldwide,1 with it being well accepted that the majority of this disease is preventable. Primary prevention (preventing the onset of disease)2 forms the cornerstone of high-quality dentistry and, in primary dental care, there is an excellent opportunity to provide this owing to the generally healthy nature of patients seen. It is acknowledged that these ‘upstream approaches’ are cheaper and more effective compared with situations when disease onset has occurred.3,4
Diet has been closely linked to oral and general health. Within the dental setting, the vast majority of evidence has historically focused on its association with dental caries, although periodontal diseases and oral cancer are also linked to nutritional status.5,6
As well as taking a whole population approach by educating patients prior to the onset of their oral/general health diseases, susceptible patients must be identified early in the onset of their disease and given consistent, evidence-based information in a way in which the chance of initiating behaviour change is maximized.
This paper aims to explore:
Some models of behaviour change to exemplify the principles of basic health psychology;
What information is available to practitioners to help guide their delivery of dietary advice;
Ways in which we can effectively deliver dietary messages to our patients.
Health behaviour: the theory
Three types of health-related behaviour are described:7
Health behaviour: Any activity undertaken by a person believing him/herself to be healthy for the purpose of preventing disease (eg eating healthy food);
Illness behaviour: Behaviour aimed at seeking remedy (eg seeing a dentist for toothache);
Sick-role behaviour: Any activity aimed to get better once disease is established (eg taking medication).
There are many theories that help us understand, predict and guide health behaviours. Those that will be discussed briefly are:
Knowledge–Attitudes–Behaviour (KAB) Model;
The Health Belief Model (HBM);
Protection Motivation Theory;
Theory of Reasoned Action and Planned Behaviour;
Social Cognitive Theory;
The Transtheoretical Model of Change.
Knowledge–Attitudes–Behaviour (KAB) Model
Traditionally, health promotion/education has been delivered as clinician-led advice that is assumed to increase a patient's knowledge on risk factors/disease.
The KAB model is considered outdated and simplistic. Knowledge does not necessarily lead to a change in attitude and, further down the line, just because patients have the positive view to reduce their sugar intake, for example, they may still continue with their current routine and thus behaviour does not change.8
A prescriptive approach to dietary advice can also be seen as critical and intrusive, particularly on a topic that can already be very delicate to address. This may result in a defensive stance where resistance to change increases as does persistence of an unhealthy diet.9
The Health Belief Model (HBM)
This was first described by Rosenstock in 197410 following Hochbaum's work on uptake of tuberculosis screening in 1958.11 It is one of the older models in health psychology and is based upon two aspects of a patient's belief:
Perception of the threat of illness – This consists of an evaluation of perceived susceptibility or severity of the disease;
Evaluation of the behaviours that can counteract the threat – This consists of the perceived barriers and benefits associated with the behaviour change.12
Combining the above beliefs is said to dictate the likelihood of a behaviour change. It suggests that there is an increased probability of behaviour change if patients consider themselves at high risk of a condition and that the benefits of the specific behaviour change outweighs the costs.
Protection Motivation Theory
This was first described in 1975 by Rogers as a development of the HBM and has been expanded over the years.13 It states protection motivation (the intention to follow behavioural advice) is determined by two appraisal processes:
Threat appraisal: This considers susceptibility to an illness and its severity (in a similar way to the HBM). The role of fear has also been incorporated, taking into account the emotional response to education/information on a disease;
Coping appraisal: This involves considering the response effectiveness (carrying out the behaviour change removes the threat) as well as self efficacy (the belief that an individual is capable of carrying out the behaviour change).12
Theory of Reasoned Action and Planned Behaviour
The theory of planned behaviour (TPB), proposed by Ajzen in 1991,14 was an expansion on the earlier theory of planned behaviour, described by Fishbein and Ajzen in 1975.15
The TPB is based on predicting behavioural intentions and considers three main factors that contribute to this:
Attitude towards the behaviour: This involves an evaluation of the particular behaviour (either positive or negative) and the beliefs about behaviour outcome;
Subjective norm: This is an individual's belief that important others should wish them to engage in a particular behaviour and then assessing whether the individual is motivated to comply;
Behavioural control: This consists of the belief that an individual can carry out a behaviour based on internal (eg skills, information, emotions) and external (eg opportunities, prices) factors.16
It is important to note that the TPB focuses on the intention to change and that may not always translate across to behaviour change itself.
Social Cognitive Model
Developed by Bandura in 1986,17 the social cognitive model outlines a number of core factors influencing behaviour change. These are:
Perceived self-efficacy: This involves the individuals' belief that a particular behaviour is within their control. It relates to the confidence that an individual has to perform the behaviour in the presence of barriers, similar to behavioural control in the TPB.
Outcome expectancies: This considers the consequences of one's actions in three aspects:
Physical outcome expectancies – This may include the expectation of symptomatic improvements (positive and negative) and can be considered in both the long- and short-term;
Social outcome expectancies – This covers the social response following behaviour change. It may include considering the reactions of friends/family as well as general social outcomes (eg finding a new job/partner);
Self-evaluation outcome expectations – This is the emotional experience of a behaviour, such as pride or satisfaction.12
Goals: These should be as specific as possible in order to guide action. The presence of a goal is, in itself, not sufficient to change behaviour but is a necessary prerequisite. A patient's self-efficacy will relate to the challenge associated with his/her goals as well as the persistence of the individual in pursuing a goal.
Socio-structural Factors: These include those opportunities or barriers in the political, environmental and health systems.12
The Transtheoretical Model of Change
The Transtheoretical Model (TTM) was first proposed by Prochaska and DiClemente in the 1980s.18 It is most renowned for its application to smoking cessation but can be extended to other health behaviours. Part of the model describes ‘stages of change’ in five steps:
Pre-contemplation: No intention of making change.
Contemplation: Considering making a change.
Preparation: Making small changes.
Action: Actively engaging in new behaviour.
Maintenance: Sustaining the behaviour change over time.12
It is acknowledged that patients may not move through the stages in a linear fashion and relapse can be common, with multiple attempts before successful behaviour change is achieved (Table 1).19
Health Behaviour Model
Possible Application to Dietary Advice
The Health Belief Model
Perceived susceptibility: I am at high risk of dental decay.Perceived severity: If I suffer from dental decay this may lead to loss of my teeth or pain.Perceived benefits: By reducing sugar frequency I will be reducing the risk of losing my teeth.Perceived barriers: I enjoy sugary foods too much.
Social Cognitive Model
Perceived self-efficacy: I believe that I am able to increase the amount of fresh fruit and vegetables I eat during the day even if it means more regular shopping trips.Outcome expectancies: This will be much healthier for my body and will lead to weight loss, as I will cut down on my refined sugar consumption. My partner will be impressed by my improved appearance.Goals: Starting from tomorrow I will add an extra portion of fruit and vegetables to a meal and gradually increase from there.Socio-structural factors: I will use the sugar-smart app to ensure that I am monitoring my refined sugar intake. I will also have to budget weekly for the extra fruit and vegetables I will be buying.
The Transtheoretical Model of Change
Pre-contemplation: I have no intention of decreasing the amount of sugar I put in my teaContemplation: I feel like I want to improve my dietary habits but I am not sure how.Relapse: The last three times I tried to stop putting sugar in my tea I failed so I am put off trying again.
What are the dietary messages?
There are numerous guidelines that the dental practitioner can consult explaining what information should be relayed to our patients regarding dietary advice. Individual guidelines will vary in their content depending upon what aspect of oral health they are focusing on. However, it is important that guidance does not contradict, as consistency of the message within the dental team is essential in order to avoid confusion amongst patients. Below is a list of guidance documents available to dental professionals referencing dietary messages as part of oral health promotion, with Table 2 summarizing a few:
Guideline
Summary of Information Relating to Dietary Advice
Delivering Better Oral Health: An evidence-based toolkit for prevention
Key messages for healthier diets:
Base meals on starchy foods;
Eat lots of fruit and vegetables;
Eat more fish;
Cut down on saturated fats;
Reduce frequency and amount of sugary food intake;
Eat less salt (no more than 6g/day);
Main messages for eating healthier:
Eat the right amount of food relative to how active a person is;
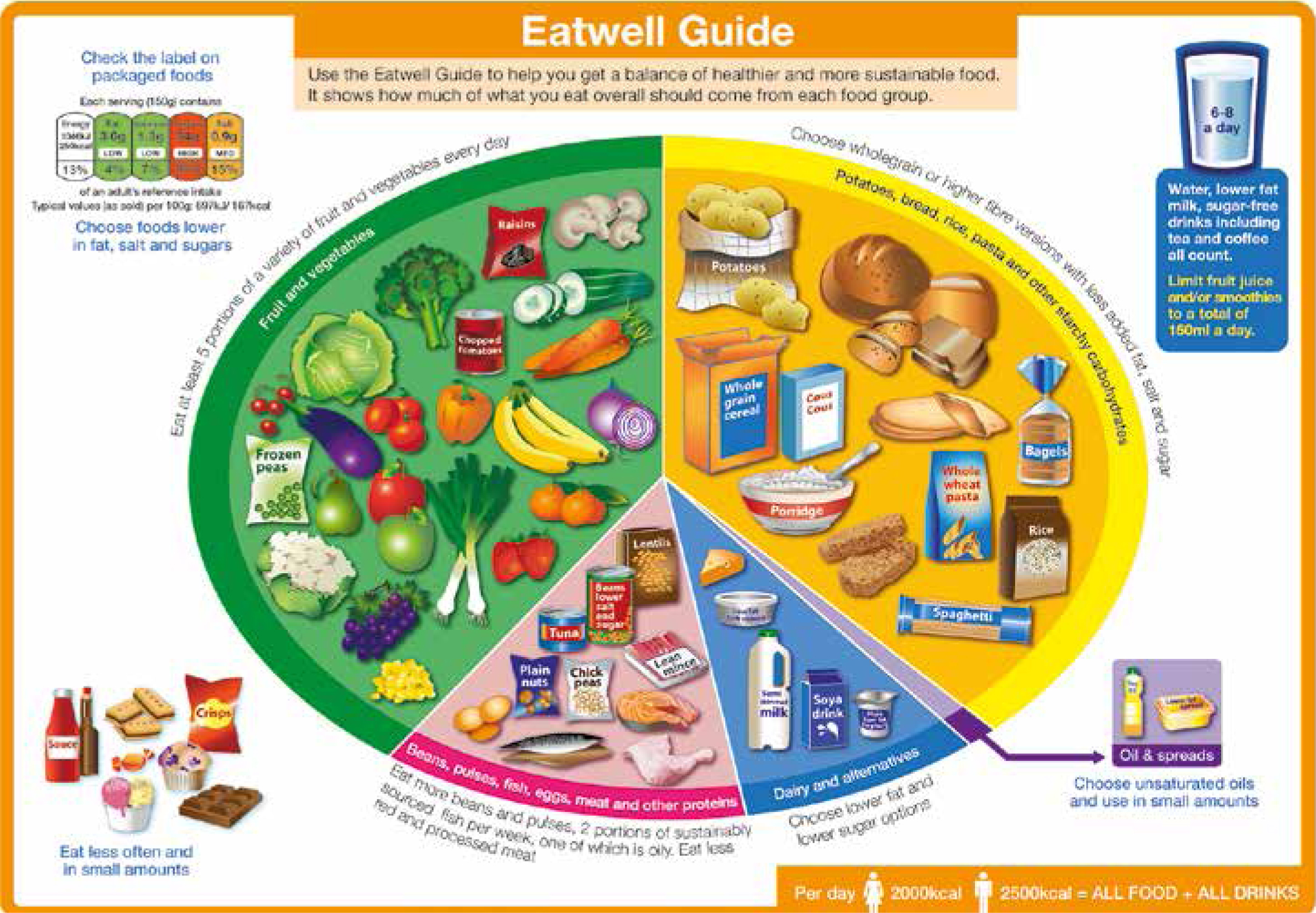
Eat a variety of food in line with the ‘Eatwell Guide’ (Figure 1).20
Consensus of the 7th European Workshop on Periodontology
Discussed the following advice as part of general health promotion and the potential for periodontal disease prevention/treatment:
Increase dietary intake of fibre, fish oils, fruit, vegetables and berries;
Reduce intake of refined sugars;
In obese patients advise restriction of caloric intake.22
Oral Health Promotion: General Dental Practice (NICE guidance)
All patients should be given dietary advice based on the ‘Delivering Better Oral Heath Guidance’.Advice should be tailored to each individual.Consider a variety of formats and the use of different media for different patient groups.21
Figure 1. The Eatwell Guide. Source: Public Health England in association with the Welsh government, Food Standards Scotland and the Food Standards Agency in Northern Ireland.
Delivering Better Oral Health: An Evidence-based Toolkit for Prevention.20
Oral Health Promotion: General Dental Practice (NICE guidance).21
Consensus of the 7th European Workshop on Periodontology.22
Oral Health and Nutrition Guidance for Professionals.23
Getting the message across
Changing behaviour in our patients should not, however, involve a purely prescriptive approach. Dental professionals should aim to empower and motivate patients to take control of their disease and oral health.
Developing a patient-centred approach to oral health promotion is not a new concept but is a focus of the recent NICE guidance, ‘Oral Health Promotion: General Dental Practice,’ published in December 2015.21 Guidance for individual approaches to behaviour have also been published in the NICE guidance ‘Behaviour Change: Individual Approaches’,24 and provide recommendations for groups who have a vested interest in behaviour change interventions, ranging from national bodies to staff working in health and social care services (Table 3).24 Whilst it is acknowledged that delivering dietary advice and making healthy eating easier for patients involves broader socio-economic factors, this article will discuss individual-level behaviour intervention.
Recommendation
Possible Incorporation to Dietary Advice in General Dental Practice
Ensure interventions meet individual needs:
Recognize times when people may be more open to behaviour change;
Discuss with the patient the impact of the behaviour change in terms of health and wellbeing;
Plan appropriate reviews during and after intervention with tailored follow-up support;
Tailor interventions to patients needs by assessing:
Current behaviour;
Physical and psychological capability to change;
Their socio-economic environment;
How motivated patients are to change.
Times when patients may be more receptive include significant events such as the birth of a child or sibling, after a recent health scare, loss of a tooth due to caries or periodontal disease, discovery of a white patch etc…Patient awareness and discussion can be raised by the use of waiting room displays and quizzes for children etc, eg focusing on the amount of sugar in common foodstuffs.
Deliver very brief, brief, extended brief and high intensity behaviour change interventions and programmes.
Dentists should be aware of local centres where patients can be ‘Signposted’ for further information, eg dietitians, general practitioners or local healthy eating clubs.The ‘One You’ website developed by Public Health England is an excellent patient education tool online with further links to healthy eating smart-phone apps that dental professionals can signpost to.25
Ensure behaviour change is maintained for at least a year:
Receive feedback and monitoring for at least a year after intervention to detect signs of relapse;
Have well rehearsed action plans if they do relapse;
Make the patient think about changes to physical environment to prevent relapse;
Help to develop routines that support new behaviour.
Good record-keeping is essential to monitor the advice given, highlight risk areas, and provide reminders to follow-up at regular intervals. Modern computer systems usually have the ability to produce ‘pop up’ reminder notes and to set recall periods in line with NICE guidance. Dentists/DCPs should regularly review the dietary status of patients at all recall appointments.26Leaflets and Apps are available helping patients develop new routines, eg the Easy Meals App.25
There are a variety of methods that dental professionals can utilize (in combination) to promote positive dietary habits effectively, in a way that motivates patients to take responsibility for their diet and improve their oral health. These methods include:
Dietary analysis and feedback;
Very brief/brief/high intensity intervention;
Motivational interviewing;
Smart-phone apps.
Dietary analysis and feedback
This is probably the most common form of evaluating a patient's dietary status and provides a snapshot of current behaviour. A six-step dietary counselling model has been described as:27
Identify high risk patients;
Take a detailed diet history;
Set goals;
Develop an action plan with realistic targets;
Monitor and review;
Refer if necessary.
As part of taking a diet history/analysis, a 3-day diet diary should be given to the patient to fill in. Reflecting on the patient's dietary habits and providing feedback allows for tailored advice and goal-setting for the individual, resulting in an increased likelihood for change.
Very brief/brief/high intensity intervention
The dental team is in an excellent position to deliver very brief, brief or extended brief advice. These are defined by NICE24 as:
Very Brief Intervention: Involves giving information and directing for further help. It follows an, ‘ask, advise, assist’ structure and can take from 30 seconds to a couple of minutes. Applying this to a nutritional model could include signposting to dietitians, general practitioners or local healthy eating clubs. Public health consultants will be able to provide details of which services are available locally. Providing very brief intervention helps identify which stage of the Transtheoretical Model our patients are at. For example, if a pre-contemplator is identified it is the duty of the clinician to ensure that he/she is aware of the impact of his/her dietary habit on oral health and to review him/her again when he/she may be ready to change (ie become a contemplator).
Brief Intervention: This involves oral discussion and encouragement as well as possible delivery of written advice. An example leaflet is ‘Diet and my teeth,’ produced by the Oral Health Foundation. It may also involve referral for further intervention or intensive support and typically takes no longer than a few minutes for basic advice.
Extended Brief Intervention: Similar to brief intervention but will last more than 30 minutes and involves an individually focused discussion. It can either be delivered over one session or multiple sessions. This could involve utilizing DCPs and nursing staff trained in oral health promotion to deliver one-to-one sessions providing tailored dietary advice following initial dietary analysis chairside.
Depending on the setting and competency of the dentist or DCP, any of the above interventions can be provided in primary care.
Motivational interviewing
Motivational interviewing (MI) is a patient-centred technique, first described by Miller in 1983.28 Whilst its initial application was for the treatment of substance abuse, in particular alcoholism, it is gaining interest in other areas of health promotion and prevention. This section aims to give an overview of the concepts behind MI and is by no means a comprehensive guide to the technique. A further source of information is the online resource.29
MI is simply described as a ‘collaborative conversation style for strengthening a person's own motivation and commitment to change.’30
Relating back to health behaviour therapy, MI has been closely linked with the TTM (Stages of Change model) as it is thought that MI can deliver the motivation to advance individuals through the various stages. Furthermore, whilst it can be seen as useful for patients at any point along the cycle, it is postulated that MI is a good technique to use with those who are at the precontemplation or contemplation stage where prescriptive techniques are known to be ineffective.30,31
Expressing empathy: This involves not only actively listening to a patient's predicament but also intense, non-judgmental reflection by the practitioner to develop a real understanding of an individual's situation and barriers.
Avoiding argument: Patients will be persuaded by what they hear themselves say. Challenging an individual's position and creating a defensive stance whereby the patient develops arguments against change goes against what MI aims to achieve.
Support self-efficacy: An extremely important aspect as outlined in Bandura's Social Cognitive Theory.17 Practitioners should encourage patients to voice self-motivational statements and support patients when they are ready to change.
Rolling with resistance: This relates to the principle of avoiding arguments and therefore not to argue with resisting statements but to explore them with the patient. It can also be seen as a point at which to offer different strategies.
Developing discrepancy: This involves identifying current behaviour and desired outcomes. Patients should ideally generate and voice their goals, in order to give the practitioner an idea of the priorities and whether they are realistic for the individual. Once discrepancy is established the dental professional can start to explore which beliefs are responsible and start the patient along the cycle of change.
The concept of MI extends beyond a series of core principles however. The ‘spirit’ of MI has been described by its pioneers and reinforces the need for an open patient-professional relationship. The key aspects to the spirit of MI are summarized in Table 4.33,34
Motivation to change comes from the patient
It is the patient's task to identify and resolve his/her conflicting thoughts (eg wanting to eat healthily but enjoy food)
Direct persuasion is not an effective way of resolving conflicting thoughts
The counselling style is generally quiet
The practitioner's responsibility is directive in helping the patient change behaviour
The readiness to change is not a patient trait but rather a fluctuating product of interpersonal interaction
The patient-professional relationship should be seen as a partnership, respecting the patient's autonomy
Smart-phone apps
Access to smart-phone technology has been on the rise for the last decade and the majority of the western population is now well versed in its use. Delivering dietary advice as well as monitoring nutritional intake is now possible to aid individuals in maintaining or even instigating behaviour change.
The ‘Sugar Smart’ app developed by Public Health England allows you to scan the barcodes of different foods/drinks and translates the sugar content to the equivalent number of sugar cubes.35 This visual tool can be an effective way of motivating the consumer to pursue healthier alternatives. Dental practices can also use the app to develop waiting room displays and quizzes, raising awareness about the amount of sugar in common foodstuffs.
Another app developed by Public Health England called the ‘Easy Meal’ app provides healthier versions of favourite meals. It can be found on the ‘One You’ website, launched in March 2016.25 Patients can be informed of this website as a means of finding further information on healthy eating.
Conclusions
This article aims to explore not only the theories underlying health behaviours, but offers techniques and examples of ways in which the dental professional can engage patients to take responsibility for their dietary habits and ultimately their oral health. In order to provide patients with self-efficacy and encourage long-term behaviour change, moving away from a prescriptive model of information giving should be encouraged, thereby embracing the importance of the patient-centred approach.