Peres PE, Santos DC, Tabchoury CPM, Cury JA Effect of bicarbonate on fluoride reactivity with enamel. Rev Odonto Cienc. 2009; 24:6-9
Frencken JE, Sharma P, Stenhouse L Global epidemiology of dental caries and severe periodontitis – a comprehensive review. J Clin Periodontol. 2017; 44:S94-S105
Axelsson P, Lindhe J The effect of a plaque control program on gingivitis and dental caries in schoolchildren. J Dent Res. 1977; 56:C142-148
Löe H, Theilade E, Jensen SB Experimental gingivitis in man. J Periodontol. 1965; 36:177-187
Van Palenstein Helderman W Longitudinal microbial changes in developing human supragingival and subgingival dental plaque. Arch Oral Biol. 1981; 26:7-12
Addy M, Slayne MA, Wade WG The formation and control of dental plaque – an overview. J Appl Bacteriol. 1992; 73:269-278
Meyle J, Chapple I Molecular aspects of the pathogenesis of periodontitis. Periodontol 2000. 2015; 69:7-17
Van der Weijden GA, Slot DE Efficacy of homecare regimens for mechanical plaque removal in managing gingivitis a meta review. J Clin Periodontol. 2015; 42:S77-91
Fejerskov O, Escobar G, Jøssing M, Baelum V A functional natural dentition for all–and for life? The oral healthcare system needs revision. J Oral Rehabil. 2013; 40:707-722
Axelsson P, Lindhe J Effect of controlled oral hygiene procedures on caries and periodontal disease in adults. J Clin Periodontol. 1978; 5:133-151
Gallagher A, Sowinski J, Bowman J The effect of brushing time and dentifrice on dental plaque removal in vivo. J Dent Hyg. 2009; 83:111-116
Kumar S, Tadakamadla J, Johnson NW Effect of toothbrushing frequency on incidence and increment of dental caries: a systematic review and meta-analysis. J Dent Res. 2016; 95:1230-1236
Slot DE, Wiggelinkhuizen L, Rosema NA, Van der Weijden GA The efficacy of manual toothbrushes following a brushing exercise: a systematic review. Int J Dent Hyg. 2012; 10:187-197
Chapple IL, Van der Weijden GA, Doerfer C Primary prevention of periodontitis: managing gingivitis. J Clin Periodontol. 2015; 42:S71-76
Sanz M, Serrano J, Iniesta M Antiplaque and antigingivitis toothpastes. Monogr Oral Sci. 2013; 23:27-44
Lippert F An introduction to toothpaste – its purpose, history and ingredients. Monogr Oral Sci. 2013; 23:1-14
Madhuri SV, Buggapati L Dentifrices: an overview from past to present. Int J Appl Dent Sci. 2017; 3:352-355
Fischman SL The history of oral hygiene products: how far have we come in 6000 years?. Periodontol. 20001997; 15:7-14
Valkenburg C, Kashmour Y, Dao A The efficacy of baking soda dentifrice in controlling plaque and gingivitis: a systematic review. Int J Dent Hyg. 2019; 17:99-116
Whelton H, Spencer A, Do L, Rugg-Gunn A Fluoride revolution and dental caries: evolution of policies for global use. J Dent Res. 2019; 98:837-846
Muhler JC, Radike AW, Nebergall WH, Day HG The effect of a stannous fluoride-containing dentifrice on caries reduction in children. J Dent Res. 1954; 33:606-612
Weatherly LM, Gosse JA Triclosan exposure, transformation, and human health effects. J Toxicol Environ Health B Crit Rev. 2017; 20:447-469
Marinho VC, Higgins JP, Sheiham A, Logan S Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2003;
Marinho VC, Higgins JP, Sheiham A, Logan S Combinations of topical fluoride (toothpastes, mouthrinses, gels, varnishes) versus single topical fluoride for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2004;
Walsh T, Worthington HV, Glenny AM Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst Rev. 2019; 3
Kassebaum NJ, Smith AGC, Bernabe E Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: a systematic analysis for the global burden of diseases, injuries, and risk factors. J Dent Res. 2017; 96:380-387
Listl S Value-based oral health care: moving forward with dental patient-reported outcomes. J Evid Based Dent Pract. 2019; 19:255-259
Listl S, Galloway J, Mossey PA, Marcenes W Global economic impact of dental diseases. J Dent Res. 2015; 94:1355-1361
Zero DT Dentifrices, mouthwashes, and remineralization/caries arrestment strategies. BMC Oral Health. 2006; 6:(Suppl 1)
Petersen PE, Lennon MA Effective use of fluorides for the prevention of dental caries in the 21st century: the WHO approach. Community Dent Oral Epidemiol. 2004; 32:319-321
Hujoel PP Historical perspectives on advertising and the meme that personal oral hygiene prevents dental caries. Gerodontology. 2019; 36:36-44
Goldman AS, Yee R, Holmgren CJ, Benzian H Global affordability of fluoride toothpaste. Global Health. 2008; 4
Paraskevas S, Rosema NA, Versteeg P The additional effect of a dentifrice on the instant efficacy of toothbrushing: a crossover study. J Periodontol. 2007; 78:1011-1016
Valkenburg C, Slot DE, Bakker EW, Van der Weijden FA Does dentifrice use help to remove plaque? A systematic review. J Clin Periodontol. 2016; 43:1050-1058
Baking soda uses beyond food. definition, safety, cleaning uses, and more. 2021. http://tinyurl.com/3huwuf24
Shrestha P, Zhang Y, Chen WJ, Wong TY Triclosan: antimicrobial mechanisms, antibiotics interactions, clinical applications, and human health. J Environ Sci Health C Toxicol Carcinog. 2020; 38:245-268
Olaniyan LW, Mkwetshana N, Okoh AI Triclosan in water, implications for human and environmental health. Springerplus. 2016; 5
Research and Markets. Global Toothpaste Market Trajectory & Analytics Report 2020: Herbal and Natural Toothpastes Give Tough Competition to Conventional Toothpastes. 2020. http://tinyurl.com/bdex3rsu
Dental Hygienist, Clinical Epidemiologist; Department of Periodontology, Academic Centre for Dentistry Amsterdam (ACTA), University of Amsterdam and Vrije Universiteit Amsterdam, Amsterdam, Netherlands
This comprehensive review traces the evolution of dentifrices from ancient concoctions to modern formulations, evaluating their role in oral health and environmental impact. Despite the global burden of oral diseases, notably dental caries and periodontitis, advancements in dentifrice technology have contributed to the decline in caries prevalence, although periodontitis remains a challenge. The historical perspective outlines the transition from abrasive powders to fluoride-enriched pastes, emphasizing the significance of toothbrushing frequency and technique, alongside the use of dentifrices, for effective plaque control and caries prevention. The modern era has seen a proliferation of dentifrice variations, with a focus on cosmetic attributes often overshadowing therapeutic benefits. The review also discusses the environmental considerations of dentifrice production and disposal, highlighting the shift towards sustainable packaging and ingredient transparency. The market analysis reveals a mature industry with a projected growth, influenced by consumer preferences and oral hygiene awareness.
CPD/Clinical Relevance: Regular toothbrushing with fluoridated dentifrice remains a cornerstone of oral hygiene practices, directly influencing the reduction of plaque accumulation and the incidence of caries and periodontitis.
Article
Oral diseases are among the most prevalent diseases globally, and they negatively impact on people's quality of life.1 Dental caries and periodontitis are the two most common oral diseases, and the major causes of tooth loss.2 Although these diseases are, in essence, preventable, they persist with high prevalence and are chronic and progressive in nature.1 The costs of treating oral diseases impose a large economic burden on families and healthcare systems.1
Prevention of caries and periodontitis
The prevalence of dental caries has decreased over the years, but the prevalence of periodontitis remains high.2 Caries, or tooth decay, is the destruction of tooth structure by acids formed by oral micro-rganisms. Dental plaque is essential in the pathogenesis of dental caries.3 It is also the main aetiological factor for gingivitis,4 which is a nondestructive inflammation of the gingival tissue. Gingivitis can progress to a chronic disease called periodontitis, characterized by inflammatory conditions that affect the supporting tissues surrounding the teeth.5,6 Periodontitis is mediated by a dysbiosis in the host–bacteria interaction, and is characterized by the loss of periodontal attachment.7 The mainstay for prevention and management of periodontal diseases has been to control bacterial plaque accumulation and/or to protect against its deleterious effects.6,8 Therefore, control of dental plaque is one of the fundamental requirements for the maintenance of a functional healthy dentition throughout a person's life.9
Toothbrushing
Toothbrushing on a daily basis is the most important step an individual can take to reduce plaque accumulation and to prevent gingivitis and the eventual development of periodontitis. It will also help to reduce the development of new carious lesions.6,10,11,12 Regardless of the use of fluoride, individuals who brush their teeth often are at lower risk for new carious lesions than people who brush infrequently.12 The risk is higher for people who brush two or fewer times per day, compared with those who brush more than twice a day.12 In addition to the frequency of brushing, the accuracy with which a person brushes their teeth can determine its effect.13,14 Other factors, such as health awareness and motivation, as well as socio-economic status and diet, may be partly responsible for the observed effects.12
Dentifrices
‘Dentifrice’ is a general term that describes preparations that are used together with a toothbrush for the purpose of cleaning and polishing the teeth, and is often used in scientific literature.15 It covers the term ‘toothpaste’ which is more commonly used in communication today. ‘Dentifrice’ is derived from the Latin, dentifricium, which combines the words dens or dentis, (tooth) and fricare (to rub).16 Dentifrices are not an invention of modern times.17 The history of dentifrices includes many examples of preparations that may even have contained harmful substances.18 Throughout the ages, dentifrices have been used to improve aesthetics, remove unpleasant odours from the mouth, strengthen the teeth and allay dental pain. They have also been used as a prophylactic to ward off epidemic diseases.19
Ancient history
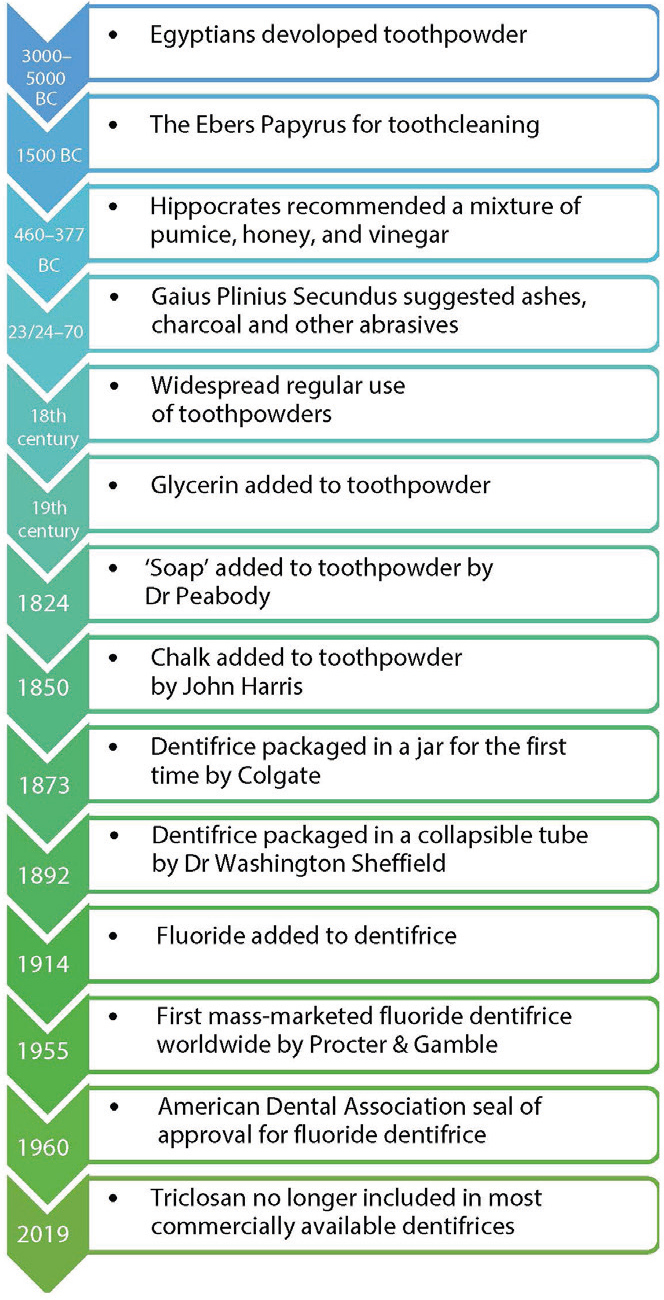
Around 3000–5000BC, ancient Egyptians developed a ‘powder’ having the main aim of removing debris from teeth. It contained powdered ashes from oxen hooves, as well as myrrh, eggshells and pumice. Water was probably added at the time of use to create a paste.17 An Egyptian medical manual, the Ebers Papyrus, written in circa 1500BC, contained a recipe for teethcleaning preparations.19 A millennium later, Hippocrates (460–377BC) described in his De Morbis Mulierum an ‘Indian medicament’ used for cleaning the teeth and giving a sweet smell to the breath.19 The Roman author, Gaius Plinius Secundus (23/24–79AD), advocated using the ashes from the head of a hare. He also stated that any useful dentifrice could be improved by adding spikenard oil to lessen the bad smell of the mouth.19 Around the same time, people in China and India were using tooth powders and pastes. The Chinese formulated their dentifrices with flavoring agents, such as ginseng, herbal mints, and salt. The dentifrices from the start of that era were rather similar to those of today.17 The most common issues with ancient dentifrices were their abrasiveness, poor taste and high cost, which meant they were not affordable on a wide scale.17
Early modern history
By the industrial era, in the 18th century, the regular use of toothpowders had become more widespread. Doctors, dentists and chemists were responsible for the development of these powders.17 Bicarbonate of soda was the basis for most of them, and is still a popular dentifrice ingredient.17,20 Glycerin was added early in the 19th century to make the powder into a paste and to prevent the paste from drying out. It also enhanced the flavour.17 ‘Soap’, in the form of salts from fatty acids, such as sodium palmitate, was added to toothpowder in 1824 by Dr Peabody. Chalk was added in the 1850s by John Harris. In 1873, Colgate was the first company to mass produce dentifrice in a jar.17 The first dentifrice that came a collapsible tube was produced by Dr Washington Sheffield in 1892, and was adopted by Colgate in 1896. The addition of fluoride as the active ingredient in dentifrice was introduced in 1914, and patented in 1915.17
Late modern history
Formulating effective fluoride-containing dentifrices is not a simple process.21 In 1955, Procter & Gamble became the first massmarketed producers of fluoride dentifrice worldwide. Their product contained 1000ppm fluoride (in the form of stannous fluoride), with calcium phosphate as the abrasive. The dentifrice was developed after more than 10 years of caries research and was the outcome of a joint research project with Dr Joseph Muhler.17,22 The American Dental Association (ADA) approved the use of fluoride salts in dentifrices in 1960. This step finally resulted in the global roll-out of fluoride-containing dentifrices.17 Currently, any dentifrice applying for the ADA Seal of Acceptance is required to contain fluoride.23 The development of synthetic surfactants after World War II led to the addition of sodium lauryl sulphate (SLS) in dentifrice formulations. This substance remains the most widely used surfactant in dentifrices because of its foaming effect.17 Furthermore, triclosan, in combination with sodium fluoride, obtained approval from the US Food and Drug Administration (FDA) for the prevention of caries, plaque, and gingivitis. However, since 2019, triclosan has no longer been included in most commercially available dentifrice because of issues related to consumer awareness.23,24Figure 1 gives a timeline of the stages of development of dentifrices.
Figure 1. Timeline for dentifrices.
Fluoride
One explanation offered for the decrease in caries in recent years is the contribution of dental care professionals, especially changes in their treatment philosophy towards less invasive approaches.9 Another explanation is the effect of fluoride dentifrice. The cariostatic effect of fluoride has been well documented,9,25,26 and the benefits have been established in research spanning more than half a century.25 A Cochrane systematic review found compelling evidence that fluoride dentifrice prevents caries more than a non-fluoridated dentifrice. Evidence regarding the effects of different fluoride concentrations is however limited. A dose-response effect was observed for d(m)fs among children and adolescents.27 Another Cochrane systematic review found that brushing twice daily increases the effectiveness of fluoridated dentifrice, as evidenced by a decrease in caries increment.25 Fluoride-containing dentifrices are currently, worldwide, by far the most important way of providing the beneficial effect of fluoride. However, although the appropriate use of fluoride has transformed oral health, dental caries will however remain a significant health burden until sugar consumption is reduced in most countries.21
Dentifrices and world oral health
Despite enormous dental expenditures, dental care systems around the world still fail to prevent avoidable dental diseases.28,29 Studies suggest that the global economic burden of dental disease totaled $442 billion in 2010, of which $298 billion was attributable to direct treatment costs, and $144 billion to indirect costs, such as productivity losses due to caries, periodontitis and tooth loss.30 While knowledge on prevention has advanced greatly over the past 50 years, the management of dental disease at the level of the individual patient remains largely empirical.31
Dentifrices can have an active role in dental prevention. The World Health Organization (WHO) states that twice-daily tooth brushing with fluoride-containing (100–1500ppm) dentifrice should be encouraged to prevent dental disease.32 However, it should be noted that the emphasis on the use of fluoride dentifrice alone can give the user a false sense of security if the harm that sugar can cause is ignored.33 In some developing countries, the price of fluoride dentifrice has been found to be too high, which could hinder equitable access.32,34 Consumers in Western society struggle with the question of which product to choose because the range of brands and formulations of dentifrice is overwhelming.
In one of the systematic reviews that the authors' group has published, it emerged that a dentifrice does not provide an added effect for the mechanical removal of dental plaque in single toothbrushing exercises. In one of the underlying studies, it was suggested that the toothbrush itself does most of the work.35 The conclusion has been misused in the media, with suggestions that we do not need a dentifrice for toothbrushing.36 This was mainly the case in the general news, but it also appeared in the professional media. Some professional organizations urged their members to correct the information based on the findings, and the British Society of Periodontology issued a press release saying that the paper was an interesting review of the available evidence and a useful addition to the scientific literature on oral hygiene habits, but it does not mean that toothpaste is a waste of time and money and advised that toothbrushing should include the use of dentifrice because it has multiple benefits.37,38
Recently published systematic reviews, meta-analyses and consensus papers covering different aspects of the prevention of dental caries and periodontal disease have each acknowledged the important role and practical limitations of mechanical plaque control.40 The value of supplementing mechanical oral hygiene measures with an adjunctive therapy that combines fluoride and an antibacterial system to enable the simultaneous prevention of caries and periodontal diseases has also been reaffirmed.40
Dentifrices and environmental health
Environmental issues related to dentifrice include packaging, toxic chemicals, and microplastics. Ethical issues include the use of palm oil and animal testing.41,42 While baking soda is regarded as a natural product, it is, on the other hand, chemically produced.39 The environmental impact of baking soda is its carbon footprint from mining and processing.43 Triclosan is a controversial dentifrice ingredient. It can affect humans both positively and negatively.44 Studies raise questions about triclosan's potential links to cancer, its effects on the thyroid, and its role in creating antibiotic-resistant bacteria.45 Colgate removed triclosan from its soaps in 2011, and from its dentifrice in 2019. GlaxoSmithKline, Unilever, and Proctor & Gamble had previously also removed triclosan from their dentifrices in response to consumer concerns and preferences.
A modern consumer trend is the ‘zero waste’ requirement that focuses on waste prevention, and encourages the redesign of resource life cycles. Colgate offers a nationwide recycling programme for dentifrice tubes.46,47,48 Based on this trend, future developments could include more biodegradable packaging, water-soluble soft gel dentifrice pods and fluoridated dentifrice tablets in biodegradable bags, glass jars or boxes.48,49 Although dentifrice tablets are touted in the market as an ‘excellent dentifrice without waste’, they still have no clinically scientific basis.
The global market for dentifrices
Worldwide, dentifrice is a frequently sold oral healthcare product that contributes to a mature and stable market. It is a highly coveted product. Brands of dentifrice have been withdrawn from shelves in some countries and only sold through customer counters. This measure was taken because dentifrice tubes are one of the most stolen products in supermarkets because the premium brands, in particular, are relatively expensive. The stolen products are used for resale. 50,51
Financial information on the overall size of the dentifrice market varies. The global dentifrice market is estimated to reach USD18.3 billion by 2025. The size is driven by sustained population growth, as well as increasing awareness about oral hygiene and the launch of innovative dentifrices.52
In today's consumer-focused market, dentifrice manufacturers place more emphasis on consumer preferences and non-therapeutic cosmetic claims than on the development of new product classes.31,53 Most recent innovations in oral care products have been directed toward making cosmetic marketing claims.31 However, consumer preferences are tightly held industrial secrets. Often users believe that all dentifrices with fluoride provide protection and, therefore, their choices are driven by other factors, such as taste, breath freshening, or specific claims, such as whitening or tartar control, with preferences varying depending on age group.31 Whitening dentifrices have been traditionally viewed more as marketing products developed at the request of consumers than as effective therapeutic interventions.
Dentifrice advertisements often feature dental care professionals in white coats who state which dentifrice they consider the best and, therefore, recommend it. This is in itself remarkable because the three largest dentifrice brands (Colgate, GlaxoSmithKline, Procter & Gamble) each claim that their products are the preferred choice of dentists.54 Surprisingly, the majority of advertisements in magazines for dental care professionals do not provide adequate and evidence-based claims.55 Considering that evidence-based practice is the gold standard,56 manufacturers should be encouraged to place greater emphasis on scientific referencing in these advertisements.55