Prada I, Micó-Muñoz P, Giner-Lluesma T Influence of microbiology on endodontic failure. Literature review. Med Oral Patol Oral Cir Bucal. 2019; 24 https://doi.org/10.4317/medoral.22907
Karamifar K, Tondari A, Saghiri MA Endodontic peri-apical lesion: An overview on the etiology, diagnosis and current treatment modalities. Eur Endod J. 2020; 5:54-67 https://doi.org/10.14744/eej.2020.42714
Siqueira JF, Rôças IN, Ricucci D, Hülsmann M Causes and management of post-treatment apical periodontitis. Br Dent J. 2014; 216:305-312 https://doi.org/10.1038/sj.bdj.2014.200
Bergenholtz G Assessment of treatment failure in endodontic therapy. J Oral Rehabil. 2016; 43:753-758 https://doi.org/10.1111/joor.12423
Haapasalo M, Udnas T, Endal U Persistent, recurrent, and acquired infection of the root canal system post-treatment. Endod Topics. 2003; 6:29-56 https://doi.org/10.1111/j.1601-1546.2003.00041.x
Stein TJ, Corcoran JF Anatomy of the root apex and its histologic changes with age. Oral Surg Oral Med Oral Pathol. 1990; 69:238-242 https://doi.org/10.1016/0030-4220(90)90334-o
Shacham M, Levin A, Shemesh A Accuracy and stability of electronic apex locator length measurements in root canals with wide apical foramen: an ex vivo study. BDJ open. 2020; 6 https://doi.org/10.1038/s41405-020-00052-3
Kielbassa AM, Frank W, Madaus T Radiologic assessment of quality of root canal fillings and peri-apical status in an Austrian subpopulation. An observational study. PloS One. 2017; 12 https://doi.org/10.1371/journal.pone.0176724
Naito T Better success rate for root canal therapy when treatment includes obturation short of the apex. Evid Based Dent. 2005; 6 https://doi.org/10.1038/sj.ebd.6400335
Kersten HW, Wesselink PR, Thoden van Velzen SK The diagnostic reliability of the buccal radiograph after root canal filling. Int Endod J. 1987; 20:20-24 https://doi.org/10.1111/j.1365-2591.1987.tb00583.x
Schropp L, Kirkevang LL Accuracy and reliability of intraoral radiographs in determining the cleanliness of root canals after endodontic retreatment. Eur Endod J. 2017; 2:1-5 https://doi.org/10.14744/eej.2017.17014
Antunes HS, Rocas IN, Alves FR, Siqueira JF Total and specific bacterial levels in the apical root canal system of teeth with post-treatment apical periodontitis. J Endod. 2015; 41:1037-1042 https://doi.org/10.1016/j.joen.2015.03.008
Restrepo-Restrepo FA, Canas-Jimenez SJ, Romero-Albarracin RD Prognosis of root canal treatment in teeth with preoperative apical periodontitis: a study with cone-beam computed tomography and digital peri-apical radiography. Int Endod J. 2019; 52:1533-1546 https://doi.org/10.1111/iej.13168
Heling I, Gorfil C, Slutzky H Endodontic failure caused by inadequate restorative procedures: review and treatment recommendations. J Prosthet Dent. 2002; 87:674-678 https://doi.org/10.1067/mpr.2002.124453
Bellamy R The implications of coronal leakage in endodontically treated teeth. Irish Dentist. 2004; 7:17-19
Portenier I, Waltimo TM, Haapasalo M Enterococcus faecalis-the root canal survivor and ‘star’ in post-treatment disease. Endod Topics. 2003; 6:135-159 https://doi.org/10.1111/j.1601-1546.2003.00040.x
Molander A, Reit C, Dahlen G, Kvist T Microbiological status of root-filled teeth with apical periodontitis. Int Endod J. 1998; 31:1-7
Ozdemir HO, Buzoglu HD, Calt S Effect of ethylenediaminetetraacetic acid and sodium hypochlorite irrigation on Enterococcus faecalis biofilm colonization in young and old human root canal dentin: in vitro study. J Endod. 2010; 36:842-846 https://doi.org/10.1016/j.joen.2010.01.008
Evans M, Davies JK, Sundqvist G, Figdor D Mechanisms involved in the resistance of Enterococcus faecalis to calcium hydroxide. Int Endod J. 2002; 35:221-228 https://doi.org/10.1046/j.1365-2591.2002.00504.x
Prada I, Mico-Munoz P, Giner-Lluesma T Influence of microbiology on endodontic failure. Literature review. Med Oral Patol Oral Cir Bucal. 2019; 24:e364-e372 https://doi.org/10.4317/medoral.22907
Ricucci D, Siqueira JF, Lopes WS Extra-radicular infection as the cause of persistent symptoms: a case series. J Endod. 2015; 41:265-273 https://doi.org/10.1016/j.joen.2014.08.020
Friedman S Considerations and concepts of case selection in the management of posttreatment endodontic disease (treatment failure). Endod Topics. 2002; 1:54-78 https://doi.org/10.1034/j.1601-1546.2002.10105.x
Nair PR, Pajarola G, Schroeder HE Types and incidence of human peri-apical lesions obtained with extracted teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996; 81:93-102 https://doi.org/10.1016/s1079-2104(96)80156-9
Archana D, Gopikrishna V, Gutmann JL Prevalence of peri-radicular radiolucencies and its association with the quality of root canal procedures and coronal restorations in an adult urban Indian population. J Conserv Dent. 2015; 18:34-38 https://doi.org/10.4103/0972-0707.148888
Sjogren U, Figdor D, Persson S, Sundqvist G Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J. 1997; 30:297-306 https://doi.org/10.1046/j.1365-2591.1997.00092.x
Bierenkrant DE, Parashos P, Messer HH The technical quality of nonsurgical root canal treatment performed by a selected cohort of Australian endodontists. Int Endod J. 2008; 41:561-570 https://doi.org/10.1111/j.1365-2591.2008.01398.x
Burns LE, Kim J, Wu Y Outcomes of primary root canal therapy: an updated systematic review of longitudinal clinical studies published between 2003 and 2020. Int Endod J. 2022; 55:714-731 https://doi.org/10.1111/iej.13736
Kvist T, Reit C Results of endodontic retreatment: a randomized clinical study comparing surgical and nonsurgical procedures. J Endod. 1999; 25:814-817 https://doi.org/10.1016/S0099-2399(99)80304-5
When considering performing root canal re-treatment, we must first consider why the original treatment failed. Failure of root canal treatments can occur when ideal technical standards for control of the root canal infection are not achieved. Sometimes, extra-radicular infection may prevent a successful treatment outcome. Teeth with post-treatment peri-apical infection can be managed by either non-surgical or surgical root canal re-treatment, both of which aim to restore health to the peri-apical tissues and prolong the survival of the tooth in the oral cavity.
CPD/Clinical Relevance: Examples of different clinical circumstances that were considered for root canal re-treatment are presented.
Article
Before deciding whether root canal re-treatment is warranted, we must first consider why the original treatment may have failed. Root canal treatment is ultimately the management of a bacterial infection,1 and post-treatment disease can be managed when the causative factors are eliminated or controlled.2 When root canal treatment is performed adequately, healing of the peri-apical lesion usually occurs with a gradual reduction and resolution of the radiolucency on subsequent examination.3 Root canal treatment may not always succeed, however, and patients may request re-treatment to resolve persistent infection4 or other reasons, such as a cyst, foreign body reaction, residual infection, or new infection.3 Root canal treatment failures are associated with clinical procedures that have not reached a satisfactory standard for managing or eradicating bacterial infection,5 resulting in an inflammatory process in the peri-apical tissue of the affected tooth.6 Unsuccessful root canal treatments may be attributed to both technical and biological failures, which include infection/re-infection/cyst formation/foreign body reaction, etc. Technical failures may include aspects of treatment procedures that failed to achieve the intended objective or fell short of the accepted level of care. Biological failures are associated with an inflammatory process in the peri-apical tissues and bacteria persisting in the root canal system. Less often, bacteria established outside the root canal may cause the post-treatment apical periodontitis.7 Either way, bacteria residing in the root canal system and/or micro-organisms in the peri-apical tissue compartment support this pathological process8 and undermine the treatment from achieving an ideal outcome.9
Key considerations for re-treating root canal-treated teeth with peri-apical infection will be discussed in this article.
Representative cases
Figures 1–5 are examples of different clinical circumstances that were considered for root canal re-treatment. These patients were keen to treat the tooth infection and avoid extraction.
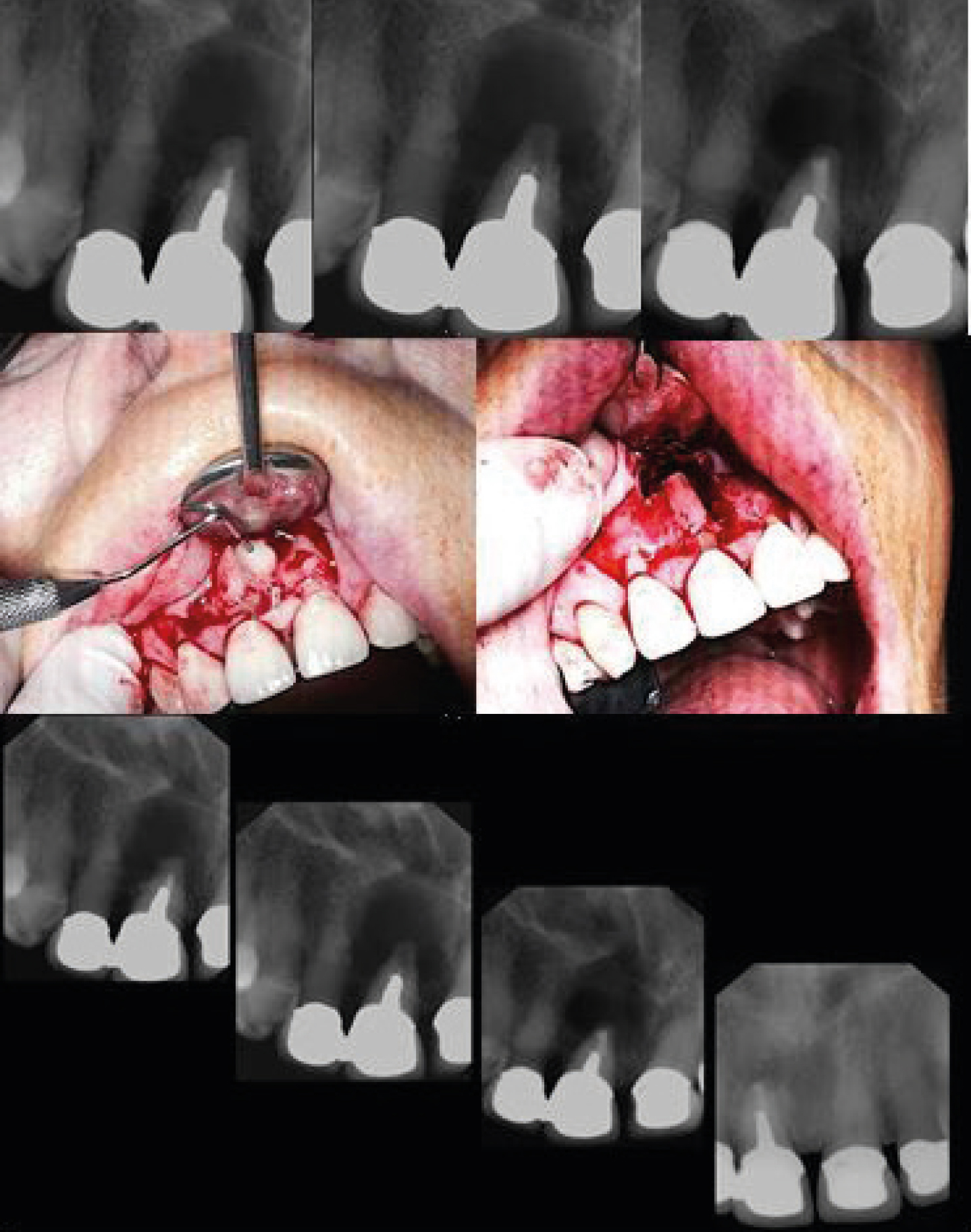
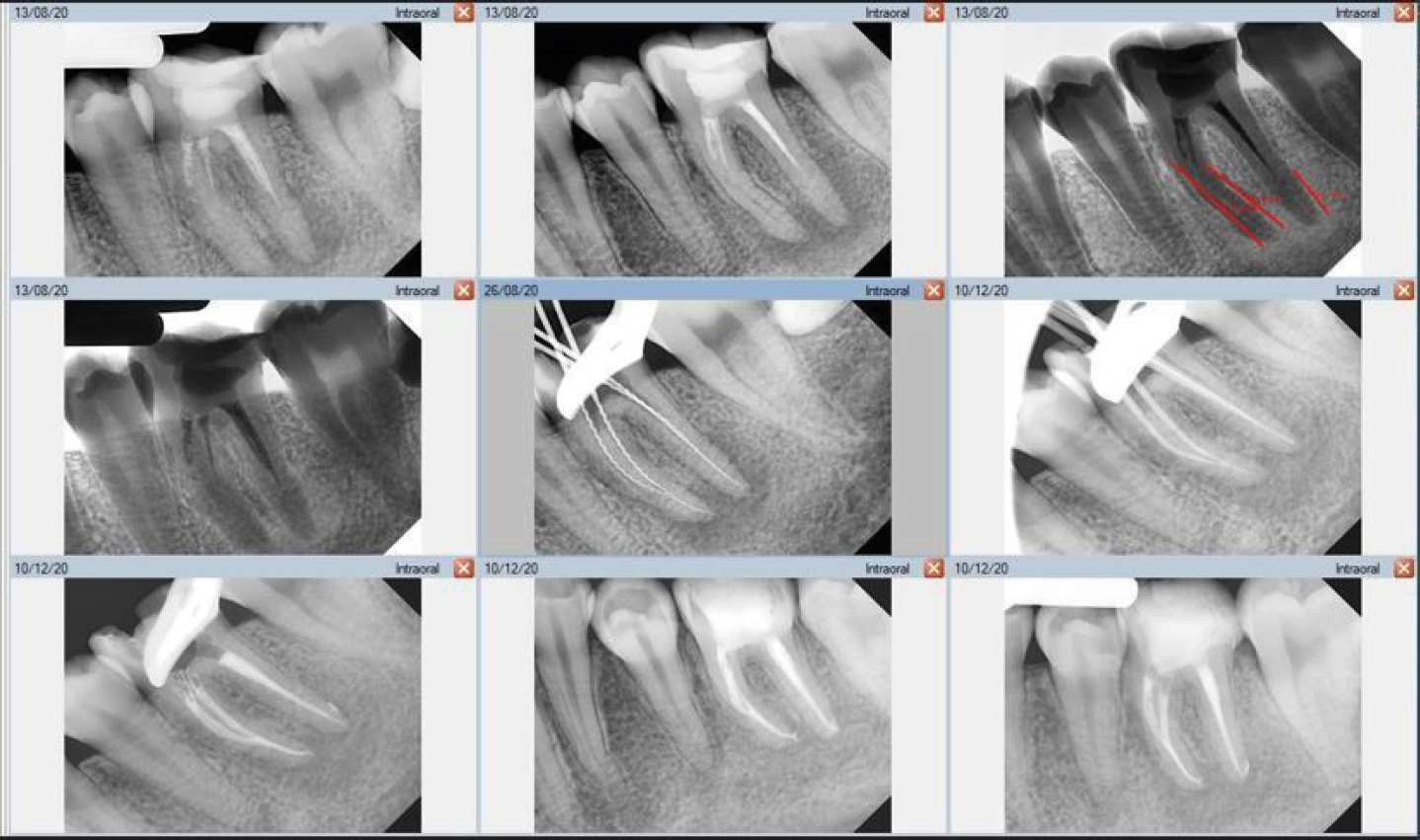
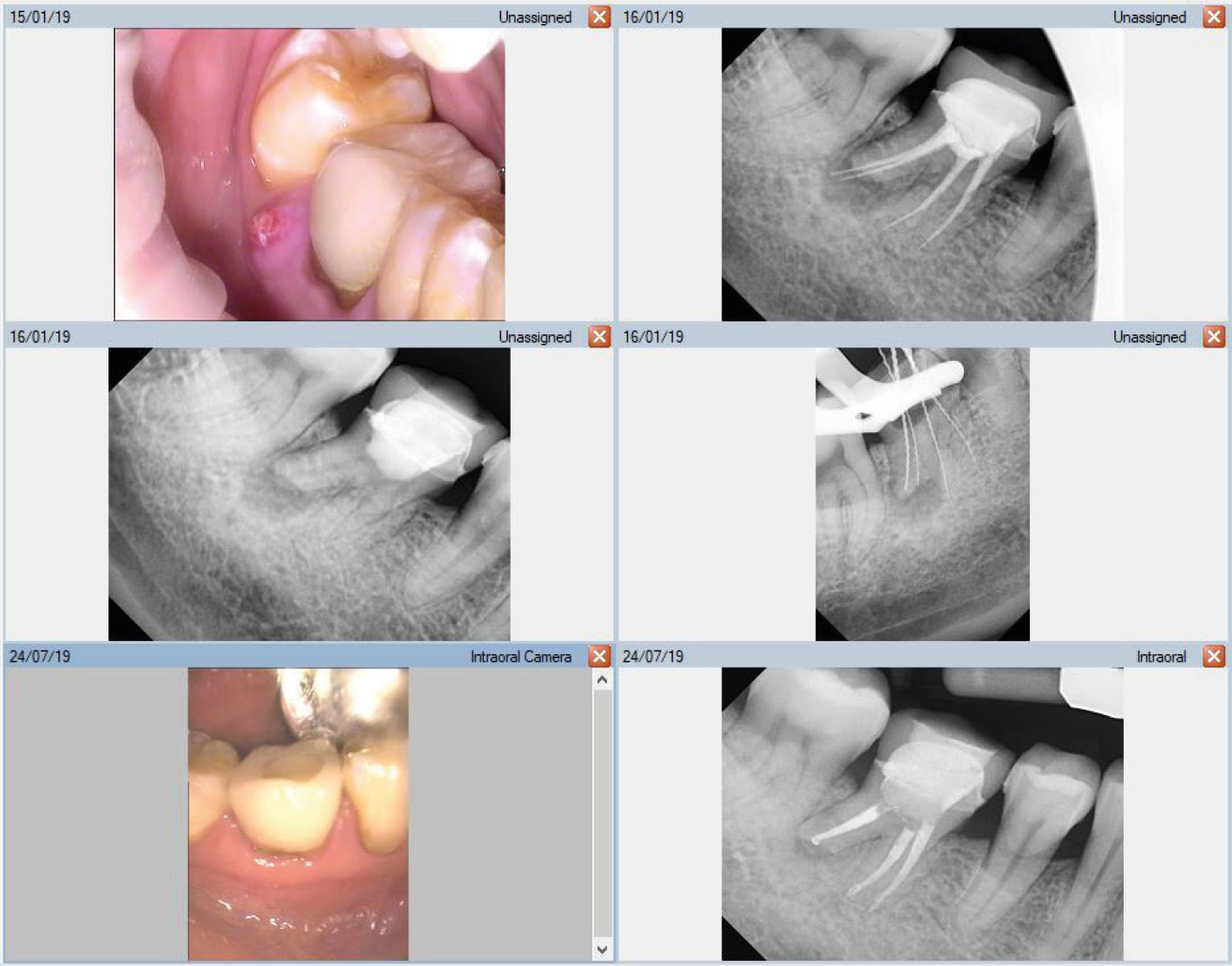
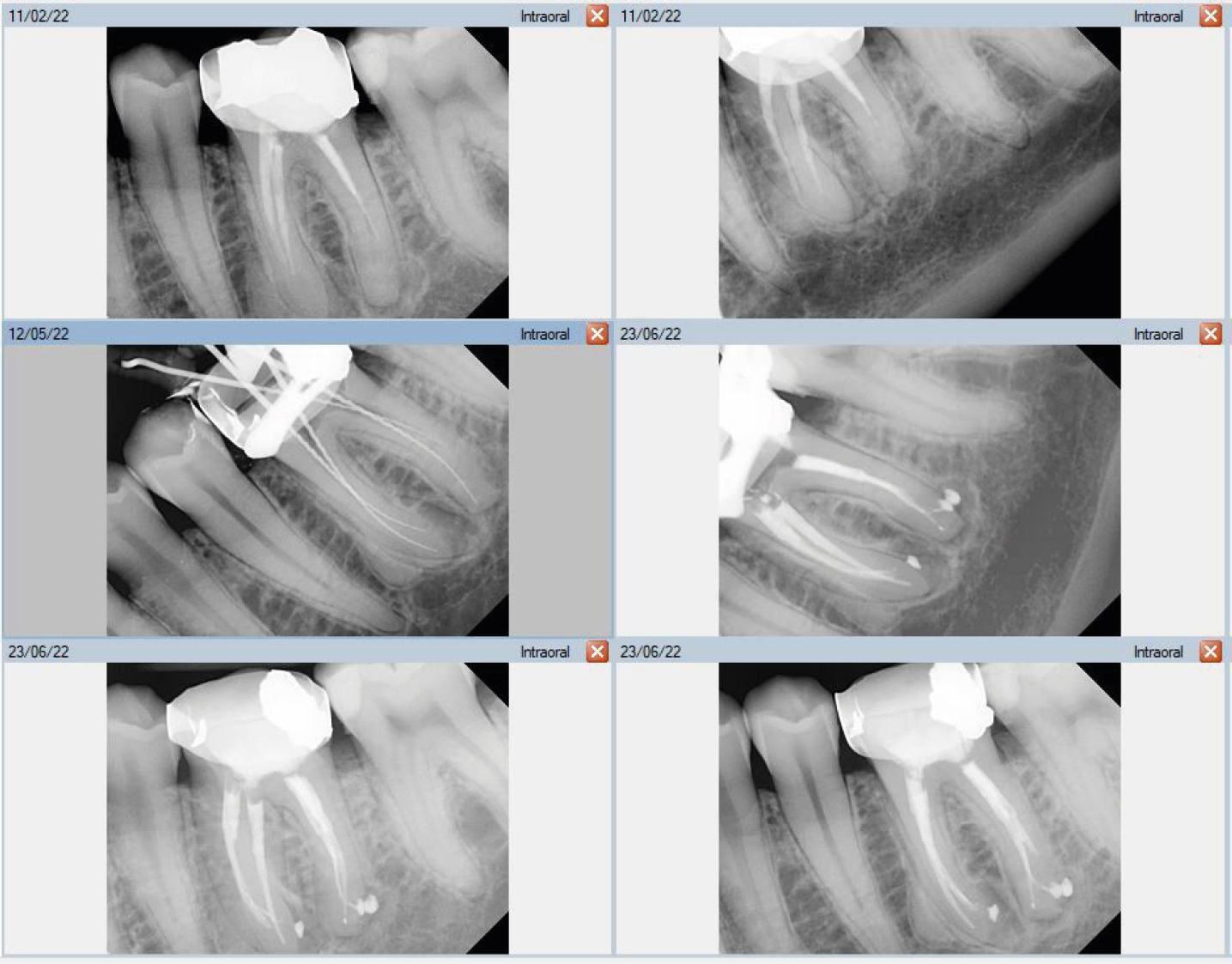
Figure 1. UR1 presenting with a large peri-apical radiolucency around a root-filled tooth restored with a post, core and crown.Figure 2. LL6 presenting with an underextended and poorly-obturated root canal filling.Figure 3. LR6 presenting with an overextended root canal filling.Figure 4. LL6 presenting with a less-than-ideal root canal filling associated with calcified canals.Figure 5. LL7 with a well-fitting crown and an adequate root canal filling, but still presenting with periapical radiolucency.
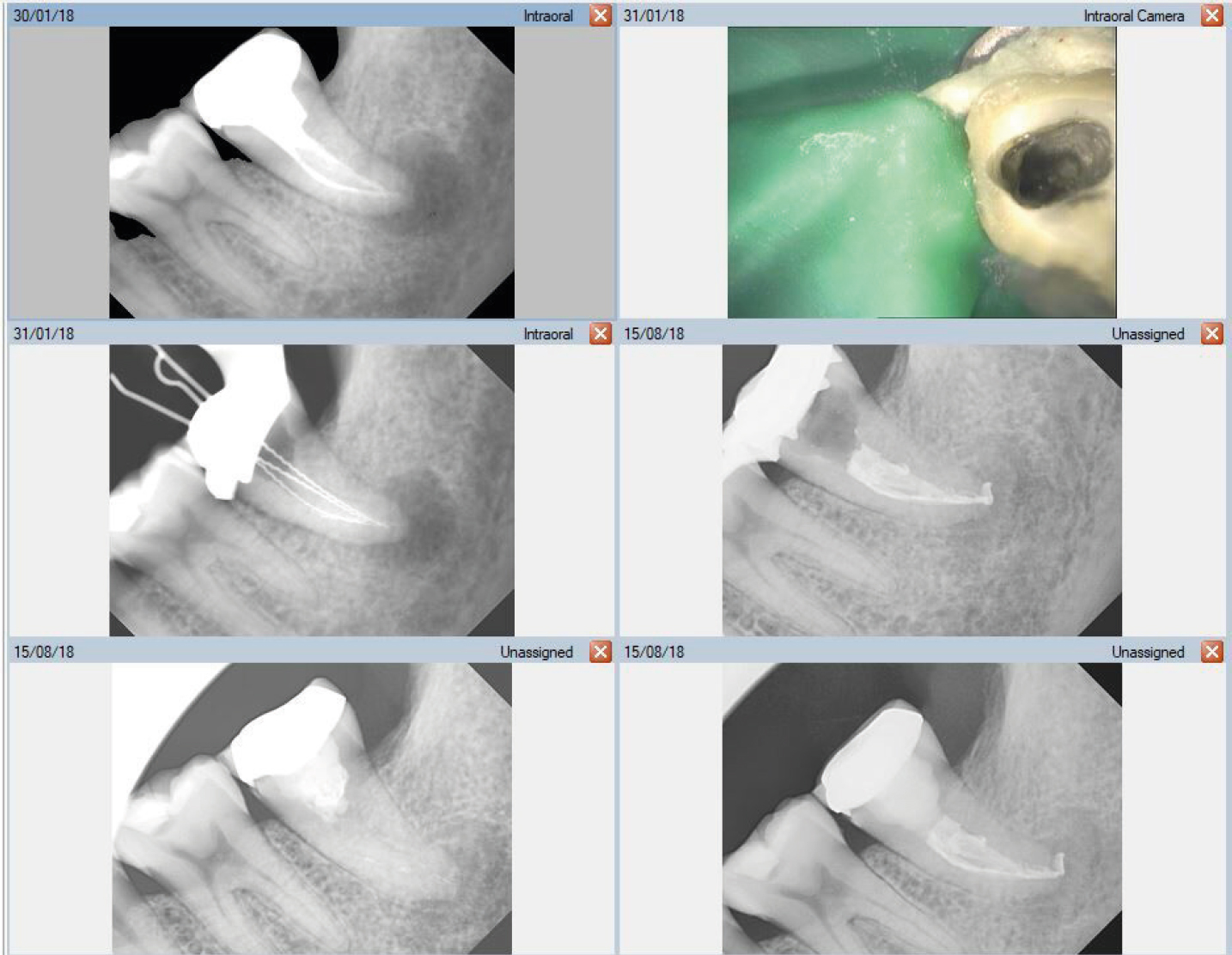
Reason for referral: non-surgical re-treatment of LL7 because of the discomfort experienced when biting and the presence of a buccal swelling.
Symptoms: symptomatic
Diagnosis: acute exacerbation of a chronic apical periodontitis associated with an infected root canal system of LL7.
Technical standard: root canal filling considered acceptable with a well-fitting crown showing no clinical evidence of coronal leakage. However, the age of the crown needs to be taken into consideration because cement can be lost, and leakage can occur. Also, there could be a missed root canal, which cannot be detected on the peri-apical radiograph.
Discussion
To accommodate the fact that healing processes may require considerable time, up to 4 years,10 it may be misleading to categorize all root-filled teeth with a peri-apical lesion as ‘root canal treatment failures' without assessing the observation period between the completion date of root canal treatment and the review appointment. The following may be possible:
The original peri-apical radiolucency has not healed after the primary root canal treatment;
The peri-apical radiolucency has persisted after re-treatment;
The original peri-apical radiolucency has healed but a new lesion has later emerged;
There was no peri-apical radiolucency at the time of endodontic treatment, but a lesion has developed over time.11
Before deciding whether to re-treat a failed root canal-treated tooth, it is important to understand why root canal treatment is susceptible to biological failures.
Technical factors
In terms of acceptable technical standards of root canal treatment, studies differ in their categorization of adequate working length and the optimal apical limit of root canal filling.12 When the apical foramen is intact, the average constriction is approximately 0.5 mm inside the canal and located close to the anatomical apex of the root.13 However, in cases of apical periodontitis, the apical foramen may often be open because of resorptive processes, and a defined apical constriction is usually absent.9 Clinically, a working distance of between 1.5 mm and 2.0 mm short of the radiographic apex has been suggested.14 A more accurate method of determining the working length would be to combine the use of electronic apex locators with radiographs.15 This combination would improve the technical quality of the final root canal filling length.16 A meta-analysis conducted to determine the optimal obturation length demonstrated that root canal fillings ending 0–1 mm short of the apex were the best,17 and a clinical study showed that an optimal treatment outcome was achieved when the apical terminus was 0–1 mm short of the radiographic apex.18 One major problem, however, is that a technically adequate root filling length assessed radiographically may not be a true representation of the adaptation and compaction of gutta percha on a proximal radiograph or in a transverse root section, particularly when canals are oval or ribbon-shaped.19 The accuracy of peri-apical radiographs has been considered poor in determining the cleanliness of root canals after endodontic re-treatment.20 In addition, disinfection of the root canal cannot be assessed or determined from radiographs and, consequently, even well-obturated canals can remain infected and support the persistence of peri-apical disease.8 Common problems that may play a role in the failure of root canal treatment include:
Inadequate mechanical instrumentation to the ideal working length;
Inadequate access cavity design to facilitate cleaning, shaping, and disinfectant irrigation;
Missed canals harbouring potential pathogenic micro-organisms and poor aseptic control techniques;
From a biological perspective, both intra-and extra-radicular infections may be involved in post-treatment disease following root canal treatment.9
Post-treatment disease can result from a persistent intra-radicular infection in the root canal.9 Intra-radicular infections are caused by bacteria harboured in the root canal system,21 having either survived the root canal treatment and persisted22 or invaded the filled root canal space after treatment,23 possibly because of leakage from coronal restoration24 or leakage due to restorative procedures such as post-space preparation.11 To survive in the root-filled canal, the intra-radicular bacteria must withstand intracanal disinfecting measures and adapt to an environment in which there are few available nutrients.8 Ecological strength becomes the determining factor for microbial survival.11 Thus, bacteria, located in areas such as isthmuses, ramifications, deltas, irregularities, and dentinal tubules, may be resistant to root canal treatment procedures.1
Enterococcus faecalis (E. faecalis) is probably the most resistant microbial species to chemomechanical preparation25 and is the dominant species present in post-treatment apical periodontitis in root-filled teeth.26 It can survive instrumentation and irrigation with sodium hypochlorite and ethylene diamine tetraacetic acid27 and is relatively resistant to calcium hydroxide intracanal medicament.28 Sedgley et al29 demonstrated that E. faecalis inoculated into root canals maintained viability for 12 months ex vivo. This resistance is probably due to a functioning proton pump, which is critical for their survival at high pH.28 Molecular studies have also confirmed that species other than E. faecalis have been detected, broadening the spectrum of species associated with failure cases.30 Pinheiro et al31 investigated the microbial flora in canals after failure of root canal treatment and observed Grampositive facultative microbial species with E. faecalis, which agrees with that reported by Molander et al.26 The clinical implications are that intra-radicular bacteria entombed by obturation may survive and give rise to future infection. Enterococcus faecalis, however, is not the most common bacteria with more recent techniques. 32 Possibly, this is due to the micro-organism's ease of culture and detection.
Extra-radicular infection (extra-radicular actinomycosis) is a chronic granulomatous, infectious disease caused by the genera Actinomyces and Propionibacterium5 and can sustain post-treatment disease process of root-filled teeth.21 A recent concept regarding extra-radicular infections as the cause of treatment failure refers to the infection being dependent on or independent of the intraradicular infection.8
Dependent extra-radicular infections are those that are supported by an intra-radicular infection but no longer persist after root canal treatment.33 If extra-radicular infection persists after successful eradication of intra-radicular infection, however, it may be an independent extra-radicular infection33 and be considered the sole cause of post-treatment apical periodontitis.8 The ability of actinomycotic organisms to establish outside the root canal, inaccessible to endodontic disinfection procedures, means they can perpetuate the inflammation at the periapex after treatment5 and therefore be a factor leading to the failure of root canal treatment.33 Where extra-radicular infection is the source of post-treatment disease, apical surgery is considered the treatment of choice because this procedure aims to remove the causative micro-organisms from the infected site (Figure 1). As non-surgical re-treatment can offer some control of micro-organisms inside the root canal system,33 and due to uncertainty regarding the coexistence of extra-radicular infection and root canal infection, concurrent non-surgical and surgical procedures would help eliminate bacteria from all possible sites.
The presence of a peri-apical cyst may also contribute to the failure of root canal treatment. Nair et al35 examined 256 peri-apical lesions from extracted teeth and found only 15% to be peri-apical cysts, 9% were true cysts, and 6% pocket cysts. A peri-apical pocket cyst is a radicular cyst containing an epithelium-lined pathological cavity that is open to the root canal of the affected tooth.36 In theory, because these cysts are open to the root canals, they are more vulnerable to micro-organisms being transported from the root canal system.9 Since endodontic disinfection procedures remove the bacterial infection from the root canal and prevent re-infection with a root canal filling material, a peri-apical pocket cyst may heal after conventional root canal treatment.37 The tissue dynamics of a true cyst, however, are self-sustaining, and the lesion is not dependent on the presence or absence of irritants in the root canal system.35 A true cyst is less likely to be resolved by orthograde endodontic therapy and requires surgical intervention.36 It is not possible, however, to confidently distinguish clinically between pocket and true peri-apical cysts. However, a pocket cyst may discharge its contents into the root canal during instrumentation, which can be detected by the clinician and then a diagnosis made.
Cross-sectional studies of endodontic treatments
When focusing on the relationship between the technical and biological aspects of peri-apical repair, lower success rates have been observed when root fillings are underfilled (Figure 2) or overfilled (Figure 3).12 A histological study reported that a favourable response of the peri-apical tissues occurred when both instrumentation procedures and root canal filling remained short of the apical constriction.38 Cross-sectional surveys of endodontic treatments performed around the world reveal a significant number of inadequate endodontic root canal fillings.12 There is an association revealed in cross-sectional studies between peri-apical radiolucency and the technically inadequate root fillings assessed radiographically.39 Longitudinal studies have reported that endodontic treatments, especially those poorly done, carry a high risk for peri-apical lesion development.40 However, these studies also suggest that it is possible to control and eliminate peri-apical periodontitis if the technical quality is optimal.12 There is variability among different observers in the evaluation and interpretation of root canal treatment success or failure based solely on clinical and radiographic criteria41 and even with the same observer at subsequent examinations.42 Observer bias will affect the interpretation of success or failure in treatment. To minimize observer bias affecting the interpretation of treatment success or failure, the collective opinion of many observers has been proposed.43 Indeed, due to the qualitative nature of many of the endodontic variables, reaching consensus appeared to be the most appropriate form of assessment.43
When should root canal re-treatment be considered?
For cases where a new coronal restoration is considered, if the technical quality of the root filling is unsatisfactory radiographically and there is a peri-apical radiolucency present, the tooth should be considered for endodontic re-treatment (as shown in Figure 4).34 However, for a tooth with an apparently good root canal filling and no peri-apical lesion the decision to re-treat is more ambiguous.44 The patient may choose to undergo elective re-treatment before placement of a new coronal restoration or accept the risk that further re-treatment may be warranted later on. If the tooth in question is not planned to receive a new definitive restoration, a previous underfilled and underextended root filling can be considered a success if the tooth is clinically asymptomatic45 and can be monitored rather than re-treated. If an adequate previous root filling with a peri-apical radiolucent lesion is present, indicative of chronic apical periodontitis, radiographs taken preoperatively and postoperatively can demonstrate the presence, absence, healing, or development of the peri-apical pathosis.34 In most endodontic treatment failures, any peri-apical radiolucency present, be it stable or reduced in size, is an expression of apical periodontitis, the same disease that the initial root canal treatment was intended to be prevent or cure.9 Ideally, recall examination and evaluation should take place for at least 4 years, especially in questionable cases46 and the European Society of Endodontology concurs with this review period.10 An observation period less than 4 years may include cases that have not attained a stable peri-apical condition.47 It is also possible that initially healed cases could later become late failures.48,49 From a biological perspective, when intra-radicular infection is suspected as the causative factor of apical periodontitis, non-surgical re-treatment will remove bacteria from the infected root canal system (Figure 5). When dealing with causes of post-treatment disease, such as extra-radicular actinomycosis or peri-apical true cysts, or where further orthograde root canal re-treatment is contraindicated, a surgical re-treatment approach will eliminate the aetiological cause directly; conventional re-treatment is of little benefit in these cases.50
Conclusion
Root canal treatment failures may be attributed to both technical and biological factors. Retreatment should be considered when a less than ideal standard technical root canal filling is associated with a peri-apical infection, whether asymptomatic or symptomatic, and a new coronal restoration will be required. When intra-radicular infection is suspected, non-surgical re-treatment will remove bacteria from the infected root canal system. When dealing with causes of extra-radicular infection, surgical re-treatment will eliminate the aetiological cause directly.