Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J. 2011; 44:583-609 https://doi.org/10.1111/j.1365-2591.2011.01872.x
Tsesis I, Fuss Z. Diagnosis and treatment of accidental root perforations. Endod Topics. 2006; 13:95-107
Kvinnsland I, Oswald RJ, Halse A, Grønningsaeter AG. A clinical and roentgenological study of 55 cases of root perforation. Int Endod J. 1989; 22:75-84 https://doi.org/10.1111/j.1365-2591.1989.tb00509.x
Balla R, LoMonaco CJ, Skribner J, Lin LM. Histological study of furcation perforations treated with tricalcium phosphate, hydroxylapatite, amalgam, and Life. J Endod. 1991; 17:234-238 https://doi.org/10.1016/S0099-2399(06)81928-X
Beavers RA, Bergenholtz G, Cox CF. Periodontal wound healing following intentional root perforations in permanent teeth of Macaca mulatta. Int Endod J. 1986; 19:36-44 https://doi.org/10.1111/j.1365-2591.1986.tb00888.x
ElDeeb ME, ElDeeb M, Tabibi A, Jensen JR. An evaluation of the use of amalgam, Cavit, and calcium hydroxide in the repair of furcation perforations. J Endod. 1982; 8:459-466 https://doi.org/10.1016/S0099-2399(82)80151-9
Breault LG, Fowler EB, Primack PD. Endodontic perforation repair with resin-ionomer: a case report. J Contemp Dent Pract. 2000; 1:48-59
Ford TR, Torabinejad M, McKendry DJ Use of mineral trioxide aggregate for repair of furcal perforations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 79:756-763 https://doi.org/10.1016/s1079-2104(05)80313-0
Main C, Mirzayan N, Shabahang S, Torabinejad M. Repair of root perforations using mineral trioxide aggregate: a long-term study. J Endod. 2004; 30:80-83 https://doi.org/10.1097/00004770-200402000-00004
Lantz B, Persson PA. Periodontal tissue reactions after root perforations in dog's teeth. A histologic study. Odontol Tidskr. 1967; 75:209-237
Himel VT, Brady J, Weir J Evaluation of repair of mechanical perforations of the pulp chamber floor using biodegradable tricalcium phosphate or calcium hydroxide. J Endod. 1985; 11:161-165 https://doi.org/10.1016/S0099-2399(85)80140-0
Frank AL. Resorption, perforations, and fractures. Dent Clin North Am. 1974; 18:465-487
Froughreyhani M, Salem Milani A, Barakatein B, Shiezadeh V. Treatment of strip perforation using root MTA: a case report. Iran Endod J. 2013; 8:80-83
Lotfi M, Vosoughhosseini S, Saghiri M Effect of alkaline ph on sealing ability of white mineral trioxide aggregate. Med Oral Patol Oral Cir Bucal. 2011; 16:e1014-1016 https://doi.org/10.4317/medoral.17158
Chau JY, Hutter JW, Mork TO, Nicoll BK. An in vitro study of furcation perforation repair using calcium phosphate cement. J Endod. 1997; 23:588-592 https://doi.org/10.1016/S0099-2399(06)81129-5
Hartwell GR, England MC. Healing of furcation perforations in primate teeth after repair with decalcified freeze-dried bone: a longitudinal study. J Endod. 1993; 19:357-361 https://doi.org/10.1016/S0099-2399(06)81363-4
Yong D, Choi JJE, Cathro P Development and analysis of a hydroxyapatite supplemented calcium silicate cement for endodontic treatment. Materials (Basel). 2022; 15 https://doi.org/10.3390/ma15031176
Bonte E, Beslot A, Boukpessi T, Lasfargues JJ. MTA versus Ca(OH)2 in apexification of non-vital immature permanent teeth: a randomized clinical trial comparison. Clin Oral Investig. 2015; 19:1381-1388 https://doi.org/10.1007/s00784-014-1348-5
Iandolo A, Ametrano G, Amato M IG-File: a novel tool to improve root canal cleaning and measurement of the apical foramen. G Ital Endod. 2011; 25:72-81
Mente J, Hage N, Pfefferle T Treatment outcome of mineral trioxide aggregate: repair of root perforations. J Endod. 2010; 36:208-213 https://doi.org/10.1016/j.joen.2009.10.012
Chen YW, Ho CC, Huang TH The ionic products from mineral trioxide aggregate-induced odontogenic differentiation of dental pulp cells via activation of the Wnt/β-catenin signaling pathway. J Endod. 2016; 42:1062-1069 https://doi.org/10.1016/j.joen.2016.04.019
Wang M, Li B, Liu Y, Tang L, Zhang Y, Xie Q. A novel bionic extracellular matrix polymer scaffold enhanced by calcium silicate for bone tissue engineering. ACS Omega. 2021; 6:35727-35737 https://doi.org/10.1021/acsomega.1c05623
Santos JM, Coelho CM, Sequeira DB Subcutaneous implantation assessment of new calcium-silicate based sealer for warm obturation. Biomedicines. 2021; 9 https://doi.org/10.3390/biomedicines9010024
Chiu YC, Fang HY, Hsu TT The characteristics of mineral trioxide aggregate/polycaprolactone 3-dimensional scaffold with osteogenesis properties for tissue regeneration. J Endod. 2017; 43:923-929 https://doi.org/10.1016/j.joen.2017.01.009
Tawil PZ, Duggan DJ, Galicia JC. Mineral trioxide aggregate (MTA): its history, composition, and clinical applications. Compend Contin Educ Dent. 2015; 36:247-252
Torabinejad M, Parirokh M. Mineral trioxide aggregate: a comprehensive literature review – part II: leakage and biocompatibility investigations. J Endod. 2010; 36:190-202 https://doi.org/10.1016/j.joen.2009.09.010
Bryan EB, Woollard G, Mitchell WC. Nonsurgical repair of furcal perforations: a literature review. Gen Dent. 1999; 47:274-248
Budig CG, Eleazer PD. In vitro comparison of the setting of dry ProRoot MTA by moisture absorbed through the root. J Endod. 2008; 34:712-714 https://doi.org/10.1016/j.joen.2008.03.004
Chogle S, Mickel AK, Chan DM Intracanal assessment of mineral trioxide aggregate setting and sealing properties. Gen Dent. 2007; 55:306-311
The world today is literate enough about the basics of oral health conditions and available treatment options. Due to the availability of many resources on different platforms the urge to retain natural teeth rather than have extractions has increased. Dental catastrophes are sometimes unavoidable in everyday dental practice. The prime motive should be patient benefit while the general dental practitioner (GDP) identifies the risks associated with the case, availability of equipment and enhanced operator skill when deciding to the referral of the patient to a specialist. Most failed root canal treatment cases have one or more associated endodontic errors. This case report presents stepwise management of such a case of iatrogenic perforation that occurred during the initial endodontic management. It emphasizes the significance of evidence-based treatment planning, role of magnification, selection of the appropriate armamentarium for performing root canal treatment, use of bioactive materials that collectively demonstrate peri-apical healing following the repair of endodontic mishaps. It also emphasizes on the importance of recall in such cases where adequate healing can be tracked over a period.
CPD/Clinical Relevance: Knowledge of management of iatrogenic perforations is useful information for clinicians.
Article
Iatrogenic perforation is an unfortunate complication that can occur during the course of endodontic treatment.1 Perforations are artificial communications between the root canal system and the supporting tissues of the tooth or oral cavity that reduce the prognosis for the tooth, and can lead to extraction.2 A study has shown that iatrogenic perforations occur in 2–12% of endodontically treated teeth during the root canal treatment.3
Iatrogenic perforations can happen either during the instrumentation of the root canal or during the post space preparation after the root canal has been prepared.4 The prognosis for a perforated tooth depends on the location of the perforation, the length of time that the perforation is open to contamination, the feasibility of sealing the perforation, and the accessibility of the main canal.5 Although a perforation is known to reduce the prognosis for the treatment, the perforation itself may not cause irreversible inflammation and failure.2 However, when a bacterial infection and/or an irritative restoration material is superimposed on the trauma of the perforation, healing will not take place. If not treated in time, consequences, such as gingival down-growth of epithelium into the perforation area,5 inflammation, resorption and/or necrosis, may result.6,7 Repair of a perforation without peri-radicular inflammation can be carried out provided infection is avoided, and asepsis maintained during the treatment.8
Many materials have been used to repair perforations, including amalgam,9 Cavit (SPE America 3M, Norristown, PA),10 Super-EBA (HI Bosworth Co, Skokie, IL),11 glass ionomer,12 among others. In order to achieve success, the perforation site must be adequately sealed with a material that is biocompatible, non-toxic, insoluble in the presence of tissue fluids, and capable of promoting regeneration of the peri-radicular tissues. Mineral trioxide aggregate (MTA) has been the material of choice for repairing root perforations.13 MTA has not only been shown to be biocompatible with the surrounding tissues, but has also a demonstrated ability to allow regeneration of these hard tissues.14
The aim of this case report is to show a case of the management of a root canal perforation caused by overzealous post space preparation after obturation.
Case report
A 25-year-old female was referred to the clinic with the complaint of persistent pain in the right mandibular vestibule region. The patient's medical history revealed no significant findings.
On clinical examination, the right mandibular first molar was tender to percussion; however, probing depth and mobility were within normal range. History revealed the initiation of root canal treatment in LR6 2 days previously, after which the patient reported an increase in pain. Since the root canal treatment had been started, it was decided to complete the treatment under rubber dam isolation and with the use of a dental operating microscope. A pre-operative radiograph was taken before commencing (Figure 1).
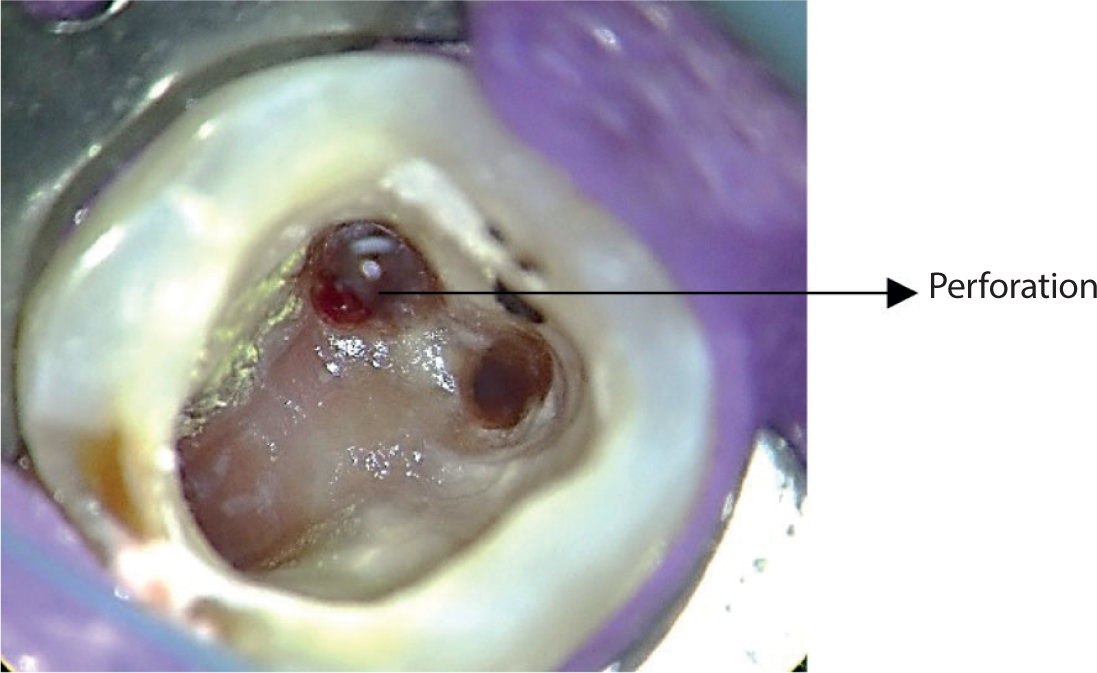
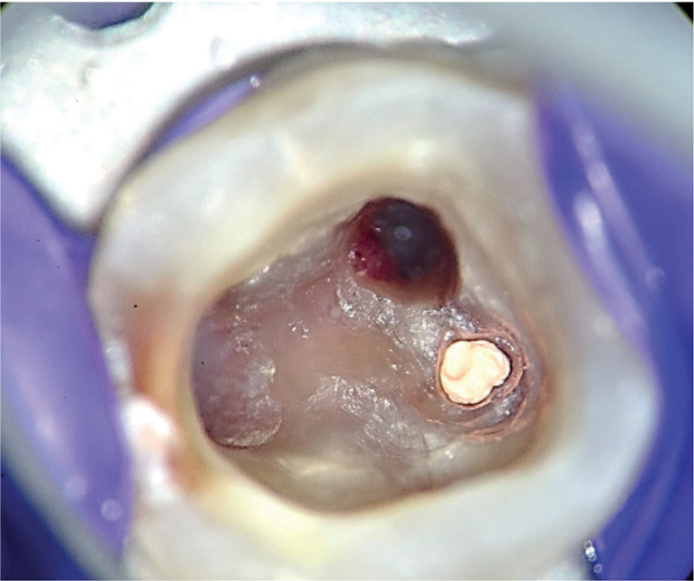
After isolation with rubber dam, the temporary restoration was removed to gain access to the pulp chamber. The endodontic access cavity was flushed with saline and dried for visualization. Once cleaned, the pulp chamber was examined carefully and the presence of a strip perforation in the mesiobuccal (MB) canal was revealed (Figure 2). Once the perforation was confirmed, bleeding was arrested at the site.
Figure 2. Clinical picture showing the presence of a perforation at the orifice of the mesiobuccal canal.
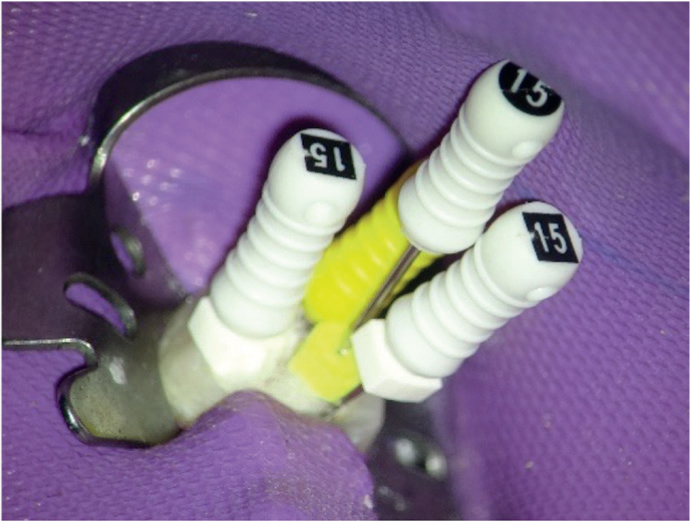
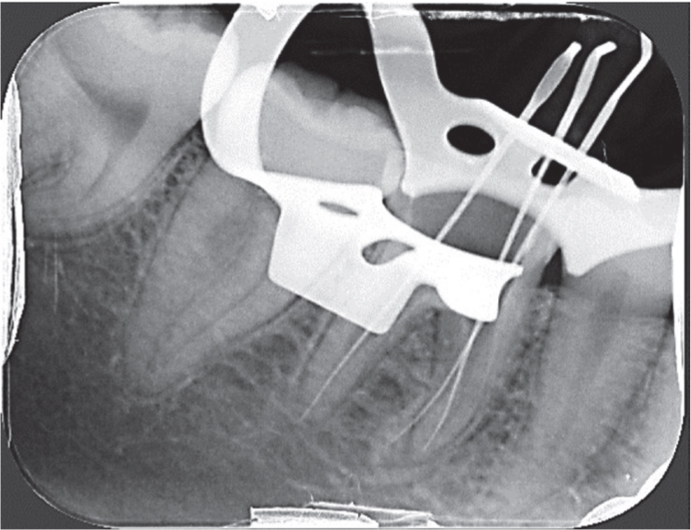
The working length in the mesiolingual and distal canals was determined with the careful use of 15k files with an apex locator and a 15 hedstrom file was used in the MB canal. Finally, a radiograph was taken to verify the working length (Figures 3 and 4).
Figure 3. 15k files used for working length determination.Figure 4. Verification of working length using a radiograph.
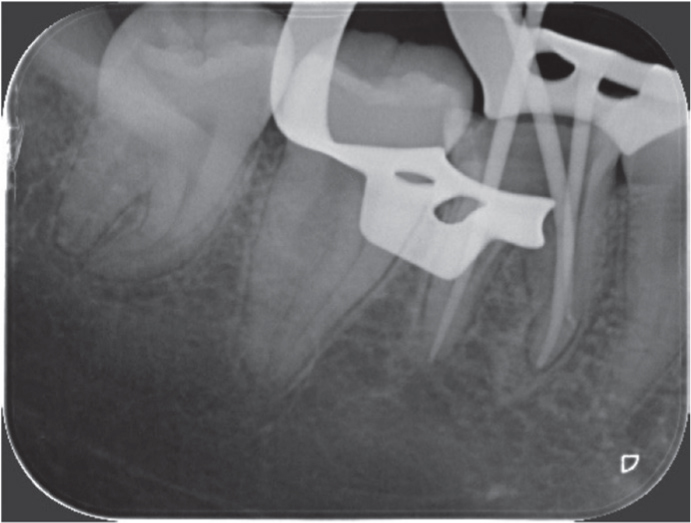
Root canal instrumentation was completed using a crown down approach with Protaper Gold (Dentsply Sirona, USA) files. The canals were instrumented till F2. The perforation site was bypassed carefully so as not to place the rotary file in the perforation, which would again cause bleeding and result in increasing the size of the perforation. Sodium hypochlorite (1% NaOCl) was used as an endodontic irrigant. The canals were irrigated thoroughly to remove any debris and to disinfect the canal. Master cone verification was performed with a peri-apical radiograph (Figure 5).
Figure 5. Master cone verification with a peri-apical radiograph.
The canals were gently dried with paper points and prepared for obturation. The mesiolingual and distal canals were planned to be obturated first (Figure 6) with corresponding F2 gutta percha (GP) and bioceramic sealer (TotalFill, FKG, Switzerland). The mesiobuccal canal was obturated apical to the perforation site as the remainder of the canal was planned to be closed with MTA (Figure 7).
Figure 6. Obturation of the mesiolingual canal with gutta percha and bioceramic sealerFigure 7. Obturation of the mesiobuccal canal with gutta percha and bioceramic sealer. Only the canal apical to the perforation was filled.
MTA (Produits Dentaires, SA) was mixed according to the manufacturer's instructions and compacted into the coronal section of the canal and perforation site using a Schilder plugger (Dentsply Caulk, Milford, USA) (Figure 8). A wet cotton pellet was placed over the MTA, and the tooth was temporarily restored using IRM (Dentsply, York, PA, USA). After 48 hours, the temporary restoration and cotton pellet were removed, and the tooth was permanently restored with resin composite with a glass ionomer base.
Figure 8. Clinical picture showing placement of MTA on the perforation site.Figure 9. Peri-apical radiograph showing obturation and MTA placement.
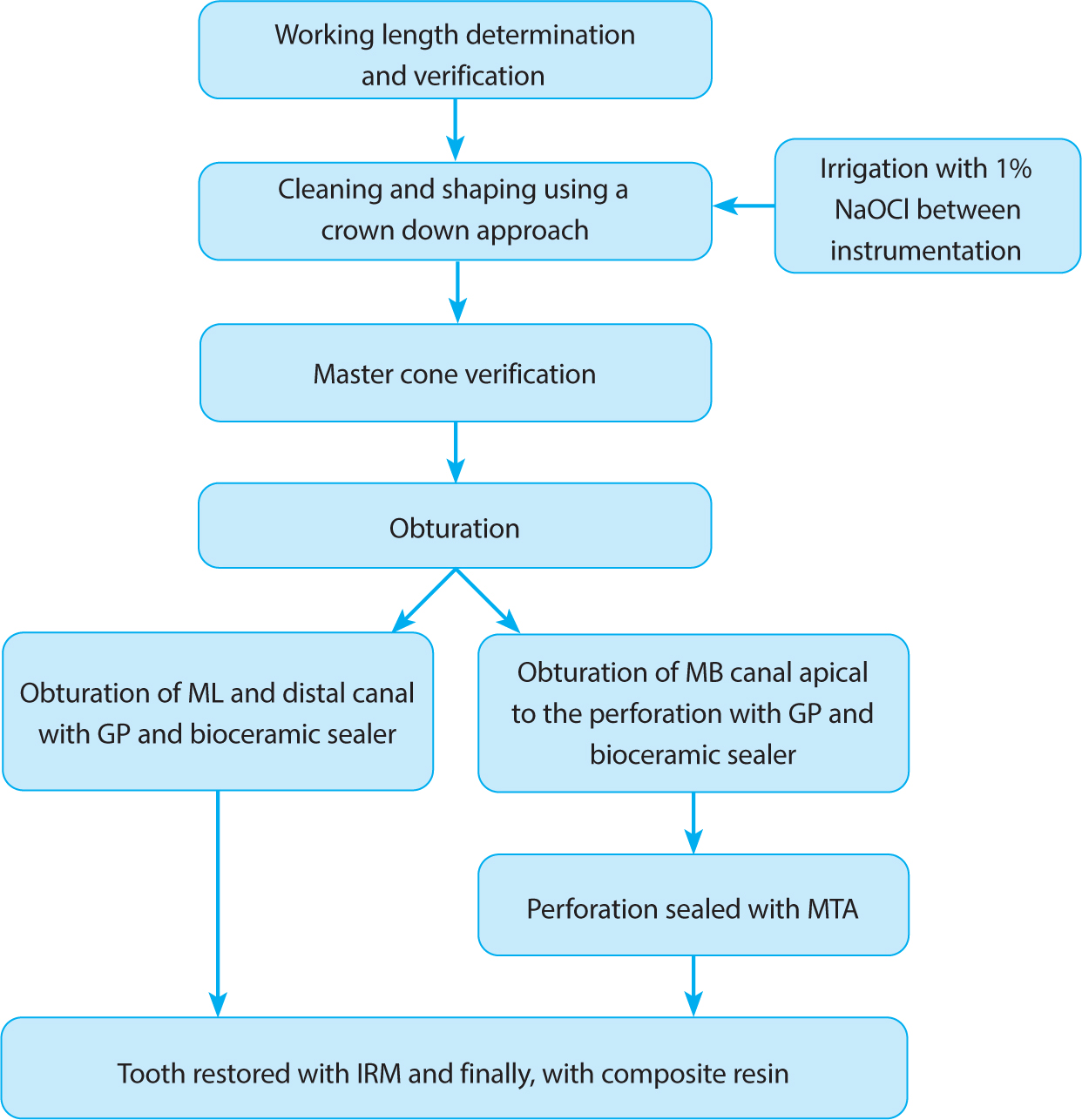
The treatment protocol used to treat this tooth is shown in Figure 10.
Figure 10. The treatment protocol used to treat the tooth.
Discussion
Perforations negatively affect the prognosis a root canal treated tooth. The mesiobuccal roots of maxillary molars and the mesial roots of mandibular molars are the most prone to strip perforations owing to their thin inner dentinal walls and the potential for overzealous preparation with large instruments.2 As a result of trauma and contamination of the site, inflammation and osseous destruction around the perforation site commences.
The treatment of perforations is affected by factors such as time between occurrence and treatment, and the location and size of the perforation2. Lantz and Persson showed that the most favourable healing of perforations occurs when they are treated immediately.15 In this case, the perforation had happened 48 hours previously, and it was decided to repair it as soon as possible. Small-sized perforations are associated with predictable healing owing to there being less destruction and inflammation.2 However, Himel et al16 found that prognosis for the perforation repair treatment was directly proportional to the size of the tooth, with larger teeth having a better prognosis.
One of the most important factors affecting the treatment prognosis is the location of the perforation. The level of the crestal bone and epithelial attachment is the critical zone in terms of prognosis. Perforations located coronal to this zone are known to have good prognosis. However, perforations apical to the critical zone can have good prognosis provided adequate endodontic treatment is rendered and the main canal and perforation site is accessible.5,17 Since the all the factors affecting the prognosis for the treatment were found to be favourable, it was decided to repair the perforation and restore the tooth.
Intracanal medicament is advisable when it comes to long-standing root canal infections. Application of calcium hydroxide is known to reduce inflammation.18 However, calcium hydroxide is known to have a negative effect on the setting of MTA.19 Therefore, in this case it was not used as the perforation was over 24 hours old and not much contamination was suspected.
Historically, materials such as amalgam, zinc oxide eugenol (ZOE) cement, Cavit, glass ionomer cement (GIC), calcium phosphate cement (CPC), decalcified freeze-dried bone (DFDB) have been used.20 Bramante et al reported that ZOE showed poor prognosis when used as a perforation repair material. Further, they showed that it can cause severe inflammatory reactions with abscess formation and resorption of the alveolar crest when used as furcation perforation repair material.21 Cavit is a pre-mixed polyvinyl paste that does not contain eugenol.10 Cavit produced a seal superior to ZOE cement, zinc phosphate cement, gutta-percha, or temporary stopping and was equavalaent to amalgam. Additionally, Widerman et al demonstrated that it did not inhibit the healing of lesions at the site of a perforation, nor was there significant likelihood of a lesion developing adjacent to a perforation filled with Cavit when no lesion was present there initially.22 Calcium phosphate cement has been shown to be highly compatible with hard and soft tissues. However, James et al found no significant differences in percentage leakage or perforation depth.23 DFDB chips are biocompatible, relatively non-toxic, easy to obtain and use, relatively inexpensive, easy to manipulate, completely degrade during the repair process and act as an excellent barrier against which filling material can be placed.20 Hartwell et al reported both positive and negative findings associated with the use of DFDB as a perforation repair material. The positives included the excellent clinical and radiographic findings at 6 months. In 85% of samples, teeth exhibited a normal appearance for periodontal soft tissues, absence of any periodontal pockets or furcation defects and absence of inflammation. The negative findings included an absence of new bone formation and epithelial growth in all specimens.24
Mineral trioxide aggregate (MTA) was introduced by Mahmoud Torabinejad in 1992.20 Since its introduction, it has been widely used and accepted as a material for various purposes. MTA is a calcium silicate cement (CSC) that has been successfully used after the use of sodium hypochlorite as a chemical disinfection25. In endodontics, it has wide range of applications, such as perforation repair, revascularization, an apical plug for the management of large and open apices (apexification) and vital pulp therapy.26-28 MTA is a well-known biocompatible material that induces cementogenesis around the perforation sites.29 Owing to its sealing ability and excellent biocompatibility, it is commonly used in regenerative procedures.30,31 MTA consists of tricalcium silicate, tricalcium aluminate, tetra calcium aluminoferrite, gypsum, bismuth oxide, and other mineral oxides that are reported to be less cytotoxic then other endodontic materials.32 However, MTA has poor wear resistance and fracture toughness that limits its life span in a load-bearing environment.33 It has been used successfully to repair perforations in different clinical situations.34,35 Owing to its hydrophilic nature, moisture is required for complete setting of the material.36 However, some studies have proposed that the moisture from tissues is often enough for proper setting of MTA, without the need for additional moisture from within the canal.37,38.
MTA has proven to be an excellent material for perforation repair. However, it has its own drawbacks, such as a long setting time, the potential to be washed out and the potential for discolouration. For perforations in the anterior region, an alternative material such as Biodentine (Septodont) or BC Totalfill RRM putty (FKG) may be more appropriate because they are less likely to discolour the tooth. They also provide the advantage of shorter setting times in comparison to their counterparts, which may mean that root canal obturation, perforation repair and a definitive core restoration can be completed in a single visit.
In the present case, MTA was successfully placed using an MTA carrier (MAP system, Produits Dentaires, Switzerland) over the perforation site followed by gentle condensation with the endodontic pluggers. Although MTA is a biocompatible and bioactive material, care was still taken to not push the MTA into the peri-radicular area, where it is not required. Since the perforation site was fully accessible and could be seen clearly under the microscope, placement of MTA was possible and efficient. The tooth was finally restored with composite resin and the patient was advised to have a post-endodontic full-coverage restoration.
Conclusion
Iatrogenic perforations do reduce the prognosis for endodontic treatment; however, much depends upon the location, size, time between occurrence and treatment rendered for these endodontic mishaps. Calcium silicate cements have shown to provide good histopathological results and are presently considered as adequate as perforation repair materials. When in contact with the peri-radicular tissues, they induce a repair mechanism by creating a biomineralizing environment. Additionally, a category of material exists that shows high success rates in the treatment of root perforations, and is a valid treatment option with wide variety of endodontic applications. However, there is still a need for long-term clinical data that can verify the success achieved after using these materials for the repair of pathological or iatrogenic perforations.