Mehta SB, Loomans BAC, Banerji S An investigation into the impact of tooth wear on the oral health related quality of life among adult dental patients in the United Kingdom, Malta and Australia. J Dent. 2020; 99 https://doi.org/10.1016/j.jdent.2020.103409
Schlueter N, Luka B Erosive tooth wear – a review on global prevalence and on its prevalence in risk groups. Br Dent J. 2018; 224:364-370 https://doi.org/10.1038/sj.bdj.2018.167
Bartlett DW, Lussi A, West NX Prevalence of tooth wear on buccal and lingual surfaces and possible risk factors in young European adults. J Dent. 2013; 41:1007-1013 https://doi.org/10.1016/j.jdent.2013.08.018
Bartlett D A personal perspective and update on erosive tooth wear – 10 years on: part 1 – diagnosis and prevention. Br Dent J. 2016; 221:115-119 https://doi.org/10.1038/sj.bdj.2016.555
Young A, Amaechi BT, Dugmore C Current erosion indices – flawed or valid? Summary. Clin Oral Investig. 2008; 12:(Suppl 1)S59-63 https://doi.org/10.1007/s00784-007-0180-6
Dahl BL, Krogstad O The effect of a partial bite raising splint on the occlusal face height. An x-ray cephalometric study in human adults. Acta Odontol Scand. 1982; 40:17-24 https://doi.org/10.3109/00016358209019805
Mehta SB, Banerji S, Millar BJ, Suarez-Feito JM Current concepts on the management of tooth wear: part 2. Active restorative care 1: the management of localised tooth wear. Br Dent J. 2012; 212:73-82 https://doi.org/10.1038/sj.bdj.2012.48
Darbar UR, Hemmings KW Treatment of localized anterior toothwear with composite restorations at an increased occlusal vertical dimension. Dent Update. 1997; 24:72-75
Buonocore MG A simple method of increasing the adhesion of acrylic filling materials to enamel surfaces. J Dent Res. 1955; 34:849-853 https://doi.org/10.1177/00220345550340060801
Mehta SB, Banerji S, Millar BJ, Suarez-Feito JM Current concepts on the management of tooth wear: part 4. An overview of the restorative techniques and dental materials commonly applied for the management of tooth wear. Br Dent J. 2012; 212:169-177 https://doi.org/10.1038/sj.bdj.2012.137
Wetselaar P, Faris A, Lobbezoo F A plea for the development of an universally accepted modular tooth wear evaluation system. BMC Oral Health. 2016; 16 https://doi.org/10.1186/s12903-016-0309-6
Ganss C, Klimek J, Lussi A Accuracy and consistency of the visual diagnosis of exposed dentine on worn occlusal/incisal surfaces. Caries Res. 2006; 40:208-212 https://doi.org/10.1159/000092227
Bartlett D, Ganss C, Lussi A Basic Erosive Wear Examination (BEWE): a new scoring system for scientific and clinical needs. Clin Oral Investig. 2008; 12:(Suppl 1)S65-68 https://doi.org/10.1007/s00784-007-0181-5
Vered Y, Lussi A, Zini A Dental erosive wear assessment among adolescents and adults utilizing the basic erosive wear examination (BEWE) scoring system. Clin Oral Investig. 2014; 18:1985-1990 https://doi.org/10.1007/s00784-013-1175-0
Dixon B, Sharif MO, Ahmed F Evaluation of the basic erosive wear examination (BEWE) for use in general dental practice. Br Dent J. 2012; 213 https://doi.org/10.1038/sj.bdj.2012.670
Mehta SB, Loomans BAC, Bronkhorst EM A study to investigate habits with tooth wear assessments among UK and non-UK dental practitioners. Br Dent J. 2020; 228:429-434 https://doi.org/10.1038/s41415-020-1326-z
Loomans B, Opdam N, Attin T Severe tooth wear: European Consensus Statement on Management Guidelines. J Adhes Dent. 2017; 19:111-119 https://doi.org/10.3290/j.jad.a38102
O’Toole S, Mistry M, Mutahar M Sequence of stannous and sodium fluoride solutions to prevent enamel erosion. J Dent. 2015; 43:1498-1503 https://doi.org/10.1016/j.jdent.2015.10.003
Mehta SB, Banerji S, Millar BJ, Suarez-Feito JM Current concepts on the management of tooth wear: part 1. Assessment, treatment planning and strategies for the prevention and the passive management of tooth wear. Br Dent J. 2012; 212:17-27 https://doi.org/10.1038/sj.bdj.2011.1099
Moazzez RV, Austin RS, Rojas-Serrano M Comparison of the possible protective effect of the salivary pellicle of individuals with and without erosion. Caries Res. 2014; 48:57-62 https://doi.org/10.1159/000352042
Kumar S, Keeling A, Osnes C The sensitivity of digital intraoral scanners at measuring early erosive wear. J Dent. 2019; 81:39-42 https://doi.org/10.1016/j.jdent.2018.12.005
Ahmed KE, Whitters J, Ju X Clinical monitoring of tooth wear progression in patients over a period of one year using CAD/CAM. Int J Prosthodont. 2017; 30:153-155 https://doi.org/10.11607/ijp.4990
Loomans BAC, Kreulen CM, Huijs-Visser HECE Clinical performance of full rehabilitations with direct composite in severe tooth wear patients: 3.5 years results. J Dent. 2018; 70:97-103 https://doi.org/10.1016/j.jdent.2018.01.001
Hemmings KW, Darbar UR, Vaughan S Tooth wear treated with direct composite restorations at an increased vertical dimension: results at 30 months. J Prosthet Dent. 2000; 83:287-293 https://doi.org/10.1016/s0022-3913(00)70130-2
Bartlett D, Sundaram G An up to 3-year randomized clinical study comparing indirect and direct resin composites used to restore worn posterior teeth. Int J Prosthodont. 2006; 19:613-617
Smales RJ, Berekally TL Long-term survival of direct and indirect restorations placed for the treatment of advanced tooth wear. Eur J Prosthodont Restor Dent. 2007; 15:2-6
Poyser NJ, Briggs PF, Chana HS The evaluation of direct composite restorations for the worn mandibular anterior dentition – clinical performance and patient satisfaction. J Oral Rehabil. 2007; 34:361-376 https://doi.org/10.1111/j.1365-2842.2006.01702.x
Gulamali AB, Hemmings KW, Tredwin CJ, Petrie A Survival analysis of composite Dahl restorations provided to manage localised anterior tooth wear (ten-year follow-up). Br Dent J. 2011; 211 https://doi.org/10.1038/sj.bdj.2011.683
Al-Khayatt AS, Ray-Chaudhuri A, Poyser NJ Direct composite restorations for the worn mandibular anterior dentition: a 7-year follow-up of a prospective randomised controlled split-mouth clinical trial. J Oral Rehabil. 2013; 40:389-401 https://doi.org/10.1111/joor.12042
Redman CD, Hemmings KW, Good JA The survival and clinical performance of resin-based composite restorations used to treat localised anterior tooth wear. Br Dent J. 2003; 194:566-572 https://doi.org/10.1038/sj.bdj.4810209
Hamburger JT, Opdam NJ, Bronkhorst EM Clinical performance of direct composite restorations for treatment of severe tooth wear. J Adhes Dent. 2011; 13:585-593 https://doi.org/10.3290/j.jad.a22094
Attin T, Filli T, Imfeld C, Schmidlin PR Composite vertical bite reconstructions in eroded dentitions after 5·5 years: a case series. J Oral Rehabil. 2012; 39:73-79 https://doi.org/10.1111/j.1365-2842.2011.02240.x
Ramseyer ST, Helbling C, Lussi A Posterior vertical bite reconstructions of erosively worn dentitions and the ‘stamp technique’ - a case series with a mean observation time of 40 months. J Adhes Dent. 2015; 17:283-289 https://doi.org/10.3290/j.jad.a34135
Vailati F, Gruetter L, Belser UC Adhesively restored anterior maxillary dentitions affected by severe erosion: up to 6-year results of a prospective clinical study. Eur J Esthet Dent. 2013; 8:506-530
Milosevic A, Burnside G The survival of direct composite restorations in the management of severe tooth wear including attrition and erosion: a prospective 8-year study. J Dent. 2016; 44:13-19 https://doi.org/10.1016/j.jdent.2015.10.015
Bartlett D, Varma S A retrospective audit of the outcome of composites used to restore worn teeth. Br Dent J. 2017; 223:33-36 https://doi.org/10.1038/sj.bdj.2017.583
Mehta SB, Lima VP, Bronkhorst EM Clinical performance of direct composite resin restorations in a full mouth rehabilitation for patients with severe tooth wear: 5.5-year results. J Dent. 2021; 112 https://doi.org/10.1016/j.jdent.2021.103743
Hoekstra-van Hout PMJ, Schols JGJH, Mehta SB Posterior Dahl: a minimally invasive method for the treatment of localized posterior tooth wear. J Adhes Dent. 2023; 25:31-38 https://doi.org/10.3290/j.jad.b3837959
Banerji S, Mehta SB, Kamran T A multicentred clinical audit to describe the efficacy of direct supra-coronal splinting – a minimally invasive approach to the management of cracked tooth syndrome. J Dent. 2014; 42:862-871 https://doi.org/10.1016/j.jdent.2014.02.017
Goldstein G, Campbell S The Dahl concept: best evidence consensus statement. J Prosthodont. 2022; 31:196-200 https://doi.org/10.1111/jopr.13441
Mehta SB, Bronkhorst EM, Lima VP The effect of pre-treatment levels of tooth wear and the applied increase in the vertical dimension of occlusion (VDO) on the survival of direct resin composite restorations. J Dent. 2021; 111 https://doi.org/10.1016/j.jdent.2021.103712
Crins LAMJ, Opdam NJM, Kreulen CM Randomized controlled trial on the performance of direct and indirect composite restorations in patients with severe tooth wear. Dent Mater. 2021; 37:1645-1654 https://doi.org/10.1016/j.dental.2021.08.018
Edelhoff D, Güth JF, Erdelt K, Brix O, Liebermann A Clinical performance of occlusal onlays made of lithium disilicate ceramic in patients with severe tooth wear up to 11 years. Dent Mater. 2019; 35:1319-1330 https://doi.org/10.1016/j.dental.2019.06.001
Hammoudi W, Trulsson M, Svensson P, Smedberg JI Long-term results of a randomized clinical trial of 2 types of ceramic crowns in participants with extensive tooth wear. J Prosthet Dent. 2022; 127:248-257 https://doi.org/10.1016/j.prosdent.2020.08.041
Sterenborg BAMM, Bronkhorst EM, Wetselaar P The influence of management of tooth wear on oral health-related quality of life. Clin Oral Investig. 2018; 22:2567-2573 https://doi.org/10.1007/s00784-018-2355-8
Sterenborg BAMM, Kalaykova SI, Knuijt S Speech changes in patients with a full rehabilitation for severe tooth wear, a first evaluation study. Clin Oral Investig. 2020; 24:3061-3067 https://doi.org/10.1007/s00784-019-03174-7
Kassardjian V, Andiappan M, Creugers NHJ, Bartlett D A systematic review of interventions after restoring the occluding surfaces of anterior and posterior teeth that are affected by tooth wear with filled resin composites. J Dent. 2020; 99 https://doi.org/10.1016/j.jdent.2020.103388
Oudkerk J, Eldafrawy M, Bekaert S The one-step no-prep approach for fullmouth rehabilitation of worn dentition using PICN CAD-CAM restorations: 2-yr results of a prospective clinical study. J Dent. 2020; 92 https://doi.org/10.1016/j.jdent.2019.103245
Lobbezoo F, Visscher CM, Ahlberg J, Manfredini D Bruxism and genetics: a review of the literature. J Oral Rehabil. 2014; 41:709-714
Wieckiewicz M, Bogunia-Kubik K, Mazur G Genetic basis of sleep bruxism and sleep apnea-response to a medical puzzle. Sci Rep. 2020; 10 https://doi.org/10.1038/s41598-020-64615-y
Over the decades, the management of tooth wear has changed significantly. With the development in the materials available and an understanding of certain occlusal concepts, a minimally invasive strategy is now the preferred option. This article outlines these developments within an evidence-based framework. Contemporary research is referenced to support the clinical approaches to current management strategies and possible future expectations.
CPD/Clinical Relevance: Knowledge of current concepts of tooth wear management in general dental practice should facilitate good treatment decisions
Article
Tooth wear can have an adverse impact on a patient’s oral health related quality of life. 1,2 The latter, in conjunction with the well-documented global epidemiological trends,3,4 may account for the growing clinical, academic, research and commercial interest with this condition.5 Over the course of the past half century there have been several significant advances in dentistry. These advances have culminated in improvements in the knowledge and understanding of dental adhesion, dental materials and concepts in clinical occlusion. Developments in the application of digital technology in the clinical setting have also taken place. Each of these factors has had an impact on the management of tooth wear. This article provides an overview of these key developments, with further focus on aspects pertinent to the assessment, diagnosis and the management of tooth wear. For descriptive purposes, we will consider matters prior to the year 2000, between 2000 and the present and the future.
Tooth wear management pre-2000
According to Young et al, the earliest published attempt to diagnose tooth wear took place towards the end of the nineteenth century.6
Clinical indices are commonly applied in contemporary dental practice for the quantification of the level of disease present using scoring criteria based on agreed descriptions. The use of an appropriate clinical tooth wear index may offer the scope of improved inter- and intra-examiner reliability and facilitate communication. Furthermore, the outcome of index scoring alongside information about the patient’s history may help to establish an appropriate diagnosis and assist with care planning. The Eccles index for dental erosion of nonindustrial origin was introduced in the late 1970s.7 The latter was the precursor of several indices, including Smith and Knight's Tooth Wear Index (TWI) published in 1984.6,8 The TWI (with a five-point grading scale) is comprehensive, remains in current use, and can be used to monitor tooth wear progression. Information obtained following the use of the TWI may be used to ascertain the efficacy of the proposed preventive plan and help determine when the implementation of restorative intervention may be appropriate. The introduction of the TWI may have been a key turning point with the assessment of tooth wear and with helping to raise the awareness of this condition among dental professionals.
Figure 1. (a) An example of a ‘Dahl’ appliance in situ. The chrome–cobalt laboratory constructed localized splint to cover the palatal surfaces of the worn maxillary UL3, UL2, UL1, UR1, UR2 and UR3. (b) Left lateral view of the appliance as in (a) to show posterior teeth distal to the canine in disclusion while the ‘Dahl’ appliance is in situ.Figure 2. (a) Localized maxillary tooth wear on the palatal surfaces of the anterior UL3, UL2, UL1, UR1, UR2 and UR3. (b) The maxillary worn teeth depicted in (a) following composite resin placement on the worn surfaces.
Traditionally, rehabilitation of the worn dentition involved the prescription of conventionally retained indirect restorations necessitating the subtraction of tooth tissue at the affected teeth, or the grinding away of opposing teeth to provide the required inter-occlusal clearance for the crown material. In 1975, Dahl et al referred to the need to protect teeth against further iatrogenic loss of healthy tooth substance in the presence of advanced attrition.9 They described the process of prescribing a general raising of the patient’s bite by applying crowns or bridges on all the teeth at the affected jaw, as the ‘solution most frequently resorted to,’ for the treatment of tooth wear cases. This would include examples of localized tooth wear, where there may only be a limited number of teeth affected. Given the complex, costly, time-consuming and highly invasive nature of providing conventionally retained crowns and bridges for the management of tooth wear, they went on to describe a technique to provide the necessary inter-occlusal space for the crown material, using orthodontic means, for the management of an 18-year-old patient with severe palatal surface wear involving their anterior maxillary teeth.9 This approach was by no means novel and the concept of ‘experimental malocclusion’ (among non-tooth wear patients) had been described by Andersen in 1962, using an orthodontic means for the creation of inter-occlusal space.10 The initial protocol applied by Dahl et al involved the fabrication of a removable chrome–cobalt splint that was approximately 2 mm thick and covered only the affected tooth surfaces.9 The splint appliance was retained by buccal clasps engaging the canine and first premolar teeth. This ‘Dahl appliance’ was worn continually other than for cleansing after a meal. Using radiographic analysis, it was demonstrated that after a period of 8 months, the space between the opposing incisor teeth was approximately equal to the thickness of the splint. Approximately 12 months after the commencement of treatment, the Dahl appliance was replaced with fixed, gold pinlay restorations at the palatal surfaces of the affected anterior teeth. This approach was subsequently prescribed to a larger base of patients.11 The inter-occlusal space attained by this approach has been postulated to be achieved through a combination of initial mandibular condylar repositioning, followed by the anterior intrusive (40%) and posterior extrusive movements (60%) of the dento-alveolar segments.11,12
Historically, where the intraocclusal space for tooth wear patients was created using relative axial tooth movement following the placement of a supra-occlusal appliance or restoration (‘Dahl concept’), the affected teeth were subsequently restored using conventionally retained crown restorations.13 While the use of the Dahl appliance would reduce the need to undertake substantial tooth preparation at the palatal surfaces of maxillary anterior teeth, invasive tooth preparations would nevertheless be required. With the progressive development of dental materials and micromechanical adhesion, the prescription of removable Dahl appliances was superseded by adhesively retained ‘fixed’ metal palatal veneers (overcoming the challenges associated with the tolerance and compliance of a removable appliance). It was indeed in Dental Update, in 1997, that Darbar and Hemmings documented a case of localized use of direct resin composite for the treatment of localized anterior tooth wear at an increased vertical dimension.14 The use of bonded tooth-coloured materials (such as resin composite) offering a superior aesthetic outcome, placed at supra-occlusal locations, has been widely described since then.13 The space attained using orthodontic techniques, as described above, will not only enable the restoration of localized wear by minimal intervention, but also alleviate the need to remove healthy tooth structure from the unaffected and affected teeth. Bizarrely, prior to the acceptance of the use of the relative axial movement for the treatment of tooth wear, it was not uncommon for some clinicians to believe that placement of full coverage crowns for the restoration of tooth wear would prevent further wear.
A key development for the rehabilitation of the worn dentition prior to the year 2000 was the introduction of early forms of bis-GMA-based composite resin by Bowen (documented in 1963) that could be adhesively bonded to enamel tissue with an acid-etch technique using phosphoric acid.15,16
Advances in dental adhesion, the availability of improved resin composites and the ability to predictably bond a range of dental materials have revolutionized the management of tooth wear. There is scope to replace lost tissue with minimal intervention, without the need to provide mechanical retention and resistance form to secure an indirect dental restoration in situ that may otherwise culminate in pulp necrosis and possible premature tooth loss.13,17 Of the available materials and techniques, the prescription of direct resin composite for the treatment of tooth wear has been most frequently documented in the literature. This is hardly surprising, given the potential merits offered by the approach.18
Figure 3. Aetiological factors considered as intrinsic or extrinsic, chemical and mechanical. Most diagnosed tooth wear has a multifactorial aetiology.
The scope to manage patients in a ‘smart’ way, using a combination of early recognition, prevention, adhesive restorative techniques, and orthodontics, culminated in several investigations being conducted into the management of localized and generalized tooth wear. The outcomes of these investigations were reported from 2000 onwards and are briefly discussed below, highlighting the relevant areas.
Tooth wear management between 2000 and the present
In 2016, Wetselaar et al reported the publication of 114 different tooth wear grading systems (clinical indices), with the TWI being the most frequently documented system.19 Although the TWI has been widely accepted and used, challenges with inter-examiner reliability and with the identification of dentine exposure have been reported.20 Furthermore, use of the TWI is not pragmatic for routine screening in general dental practice.20
A key development with tooth wear indices was the introduction of the Basic Erosive Tooth Wear Examination (BEWE).21 The BEWE, a partial scoring system modelled on the Basic Periodontal Examination (BPE), comprises four levels (Table 1). The aim of introducing the BEWE was to facilitate tooth wear screening and raising the professional awareness of tooth wear. The BEWE has been reported to offer ease of use and acceptance among examiners.22 Unfortunately, however, for the screening of tooth wear in general practice, there remains the lack of consensus with a given tooth wear index,23 with one study reporting less than 14% of their sample of 297 dentists using any form of tooth wear index to undertake routine charting for wear and only 5% using the BEWE.24
Table 1. Criteria from the Basic Erosive Wear Examination (BEWE) for grading erosive tooth wear.20
Score
Criteria
1
No erosive tooth wear
2
Initial loss of surface texture
3
Distinct defect; hard tissue loss, 50% of the surface area
Indeed, until more recently, there was a general lack of consensus, with a plethora of aspects relating to (severe) tooth wear management. An important development, following a meeting of an expert panel in Nijmegen, the Netherlands in 2016 was the publication of ‘The consensus statement for the management of severe tooth wear’.25 As part of this, agreement was reached over several important areas including definitions for key terms, such as ‘pathological wear,’ which related to the rate and ‘severe tooth wear,’ which related to the amount of wear (defined by the highest grade of index scores). Without such descriptors, comparing the outcomes of different investigations would prove impossible. A protocol for the overall management of the severely worn dentition was also described in the consensus statement, with emphasis on prescribing effective preventive measures and arrangements for patient counselling and monitoring regardless of the severity of the presenting tooth wear. When tooth wear may be a concern for the patient and/or the clinician, it was also agreed, where possible, restorative intervention should be carried out using minimally invasive approaches, in an additive manner.25
In relation to the prevention of tooth wear, copious work relating to the role of fluoride and other minerals (such as sodium, stannous and titanium ions) has been made available over the past two decades,26 with further recognition of the role of products containing calcium for the management of the progression of erosive lesions.5,27 During this period, there has also been a widening of the understanding of the importance of the frequency of consumption of potentially erosive foods and beverages,28 their respective buffering capacity, as well as the role of saliva (especially the salivary pellicle) in tooth wear progression.29 The aetiological causes have remained multifactorial, however, the trend towards their recognition as intrinsic versus extrinsic and mechanical and/or chemical factors has superseded the more conventional attrition, abrasion, erosion and abfraction descriptions.
Knowledge of the efficacy of the preventive programme would require careful assessment of the progression. This may be done directly, often using an index, or undertaking scoring indirectly using records such as gypsum casts, which has its limitations, and/or clinical photographs. The use of clinical indices for tooth wear assessment has, however, been described to be subjective, nonquantitative and lacking in the required level of sensitivity.30 Furthermore, the use of a tooth wear index may not offer reliable outcomes unless effective training is provided.31 The use of intra-oral scanners has gained considerable popularity in the primary care setting in recent times. Ahmed et al described the feasibility of using CAD/CAM (computer-aided design/computer-assisted manufacture) scanning as a means of offering a more accurate and consistent way of monitoring tooth wear progression compared to the methods listed above.32 Kumar et al reported the potential of scanned data from intraoral scanners to detect early erosive wear, however, the precision was low, which may render detection of minimal changes to be challenging.30
Figure 4. Use of intra-oral scanners for the monitoring of tooth wear.Figure 5. (a) Significant tooth wear on an isolated lower right first molar tooth in a young patient. (b) The singular worn first molar shown in (a) restored with a direct composite restoration. (c, d) Re-establishment of shimstock holds on the left and right teeth after single composite restoration placement as shown in (b).
Performance data for direct resin composite restorations for the treatment of tooth wear started to become available at the start of the new millennium. With some exceptions, promising outcomes, overall, have been described,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47 especially for the restoration of localized anterior tooth wear, with acceptable survival rates (at or about the value of 90%) and high levels of patient satisfaction, with care often involving the placement of dental materials in a supraocclusion. The Dahl concept (also referred to as relative axial movement) has been a key development for the conservative management of localized anterior tooth wear, with a reported overall success rate of 83–100%.12 Furthermore, the objectives of the Dahl concept have been reported to have been achieved among 94–100% of cases in various investigations, with a mean time of 6 months for the occlusion to re-establish and with a very low incidence of adverse events.12 In 2023, Hoekstra-van Hout et al first described the successful use of the Dahl concept for the treatment of localized posterior tooth wear as part of a retrospective case series, with high levels of patient satisfaction with their treatment outcomes.48 Although the use of the Dahl concept has since been extended for the successful and minimally invasive management of other dental conditions such as cracked tooth syndrome,49 a recent best evidence consensus statement evaluating the available data in relation to the Dahl concept,50 has alluded to the lack of compelling evidence to support the proposed means by which the inter-occlusal space is achieved, as well as the long-term stability of that position and the stability of the restorations.
Many of the investigations listed above relating to the performance of direct composite restorations for the treatment of tooth wear have, however, included relatively small sample sizes and/or shorter observation periods. Only two of these studies have included samples with more than 1000 direct composite restorations, with longer observation periods.45,47 As part of an evaluation of 1269 direct resin composite restorations for the treatment of 34 patients with severe (generalized) tooth wear by by Mehta et al over an observation time of 5.5 years, only a small number of catastrophic failures were encountered (2.3%).47 In the same study, annual failure rates (AFRs), which include all types of failure) of no more than 2.2% (anterior restorations) or 2.9% (posterior restorations) were observed. However, molar tooth restorations and anterior restorations that needed further sessions for completion displayed significantly higher failure risk.47 Assessment of the data from the latter investigation (as part of a separate study) alluded to the importance of a timely intervention, with higher levels of anterior tooth wear associated with higher failure risk and the importance of restoration thickness on survival.51
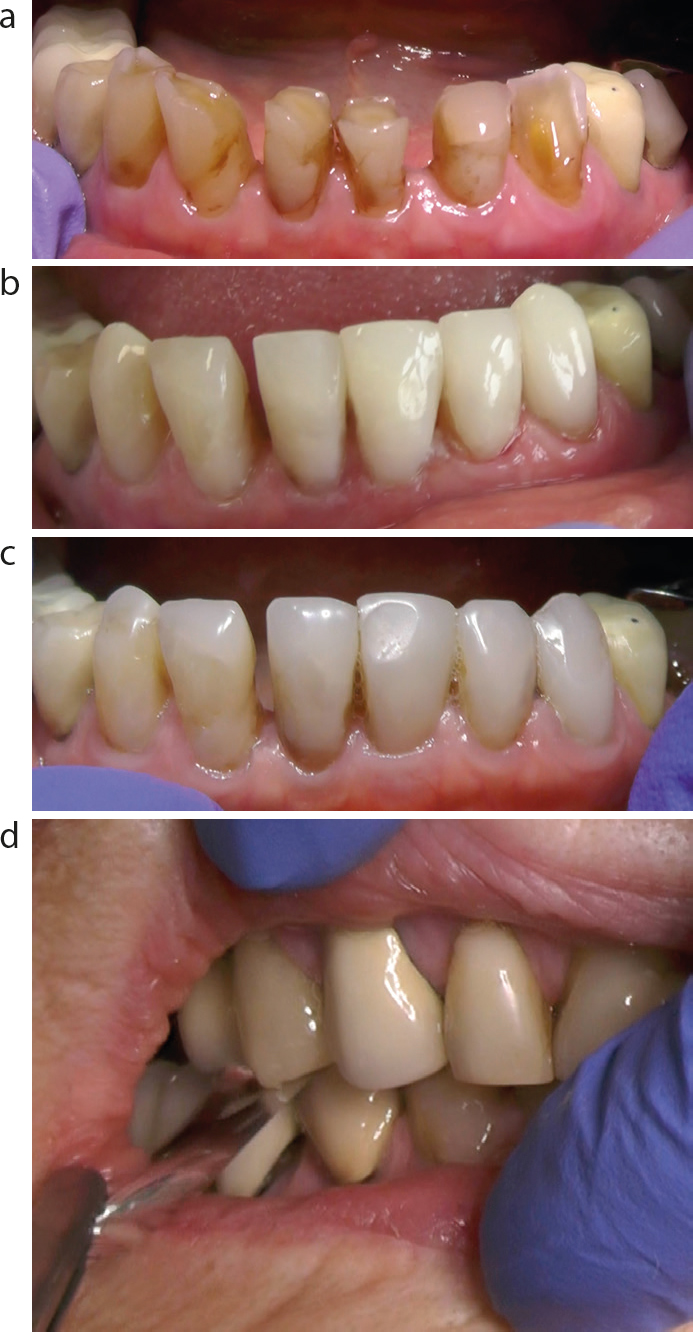
Figure 6. (a) Localized tooth wear on the lower anterior teeth in an elderly patient. (b) Localized lower anterior direct composite build up on LR3, LR2, LR1, LL1, LL2, LL3 for patient shown in (a). (c) Localized lower anterior direct composite build up for patient shown in (a) and (b) after a period of 4 years. (d) Shimstock holds established for patient shown in (a–c) following localized lower anterior composite build ups on LR3, LR2, LR1, LL1, LL2, LL3.
The available data for the performance of indirect restorations for the treatment of tooth wear are less abundant. As part of a randomized clinical trial, with evaluation after 3 years of service, favorable and comparable outcomes were reported by Crins et al for the use of direct and indirect anterior resin composite restorations for the treatment of severe palatal surface wear.52 However, for indirect resin composite restorations in the posterior dentition, the outcomes were considerably lower than posterior direct restorations, with the rate of failure three times higher and AFRs of 3.2–5.4% and 8.5–15.5% for direct and indirect restorations, respectively.
The scope to predictably bond contemporary ceramic materials offering superior aesthetics and acceptable mechanical properties for the restoration of posterior teeth has also been a significant development over the past two decades. This has enabled restorative rehabilitation of the worn dentition without the need to provide mechanical retention and resistance form. Highly promising data have been reported for the use of monolithic posterior occlusal onlays made of lithium disilicate ceramic with a minimum 1 mm layer thickness (n = 103), with a 100% survival rate with up to 11 years of service.53
Until very recently, limited data have been available about the performance of conventionally retained crowns for the treatment of tooth wear.36 In 2022, Hammoudi et al reported on the performance of 713 crowns (pressed lithium disilicate crowns, n = 362 and translucent zirconia crowns, n = 351) for the management of extensive tooth wear with an observation period of up to 6 years.54 A survival rate of 99.7% was reported with the absence of any significant difference between the two materials used, or the presence of a mechanical or chemical aetiology. Full coverage crowns may, therefore, also provide suitable treatment outcomes with the need for minimal maintenance; however, patients must be carefully counselled about the risks. For resin composite restorations, regular refurbishment and periodic maintenance will be required.
The future, post-2023
While the criteria for restorative intervention based on clinical need have been established, which include aesthetic, functional and symptom-related concerns, more recently, data have started to emerge in relation to the importance of the impact of tooth wear on the patient’s quality of life.1,2 This may vary between individuals and is an important consideration when planning the timing of restorative treatment. While attempting to attain informed consent for the restorative treatment of the worn dentition, it would be relevant to discuss the potential improvements in the patient’s quality of life alongside the likely prognosis.1 While short-term data for patient-reported outcome measures (PROMS), following full mouth rehabilitation using direct composite, on measures such as speech function and oro-facial aesthetics is accessible,55,56 it is hoped that longer-term data will also become available. This may enable a better understanding of the true merits of the complex and costly interventions that are often required, especially for full mouth reconstructions.
With the establishment of international tooth wear projects, such as the Radboud Tooth Wear Project in Nijmegen,57 long-term performance data for a plethora of dental materials used for the treatment of tooth wear is likely to become available, together with a deeper understanding of factors that may influence clinical outcomes. These could include (but are not limited to) the role of the aetiology, the extent and severity of the presenting wear, the materials used, the timing of restorative intervention, operator skill and technique, etc. Knowledge of the possible risks may help planning of care and help to reduce the variation in outcomes with the use of direct composite for the treatment of tooth wear as described in a systematic review.58 Further longer-term data may also lend support for the superiority of a given material and/or application technique for the treatment of severe tooth wear, which is currently lacking.59
Bruxism, which has long been considered a considerable challenge during the management of tooth wear, may have a genetic predisposition and therefore require an alternative approach towards controlling its adverse effects.61,62 As digital technology continues to evolve and becomes more widely used in primary dental care, the routine use of digital tooth wear measuring tools may help to accurately identify signs of early tooth wear, assist with its assessment, and help to monitor progression. Furthermore, with the scope to input information, such as the impact of the condition on the patient’s quality of life, the aetiological factors, and the results of further special investigations (eg salivary tests and bruxism measuring tests), artificial intelligence could be used to assist management using established algorithms.
The provision of restorative care for tooth wear patients may also be facilitated using CAD/CAM. The evolution of new dental materials with superior mechanical and adhesive properties may offer more scope to provide treatment with minimal intervention, and could also help a larger number of patients receive the required care in a predictable way and within the primary care setting. An example is the recent introduction of polymerinfiltrated ceramic network materials (PICN) – hybrid ceramics, combining the desirable mechanical, physical and aesthetic properties of both ceramics and composites. PICN materials may be used to restore worn teeth using CAD/CAM and without the need for tooth preparation. Interesting performance data were reported from a 2-year prospective clinical where 192 PICN onlays (0.55 ± 0.21 mm thickness at molar teeth) were prescribed for the treatment of tooth wear, with a planned mean increase in the occlusal vertical dimension of 5.08 ± 0.84 mm using a ‘one step, no-prep approach,’ with 100% survival and 93.5% success, and good patient acceptance.60 The minimally invasive merits offered with this protocol may have a profound impact on the restorative rehabilitation of tooth wear patients.
Conclusion
The developments in materials, coupled with the profession’s understanding and awareness of tooth wear, has significantly steered the management of this condition from an invasive tooth reductive approach towards progressively minimally invasive protocols. With improvements in materials, monitoring and resources, this trend is continuing to develop.