The Establishment of an Intravenous Conscious Sedation Service for Adult Patients in a Primary Dental Care Setting Rebecca SL Binnie Nigel D Robb Sarah L Manton Stephen J Bonsor Dental Update 2024 47:1, 707-709.
Authors
Rebecca SLBinnie
BDS, DPDS, GDP
The Dental Practice, 21 Rubislaw Terrace, Aberdeen; Clinical Lecturer (Scholarship), Institute of Dentistry, University of Aberdeen
BDS(Hons) MSc FHEA FDS RCPS(Glasg) FDFTEd FCGDent GDP
The Dental Practice, 21 Rubislaw Terrace, Aberdeen; Hon Senior Clinical Lecturer, Institute of Dentistry, University of Aberdeen; Online Tutor/Clinical Lecturer, University of Edinburgh, UK.
Dental anxiety is common within the population and can detrimentally affect the delivery of dental care for those patients affected. Non-pharmacological-based behaviour management techniques are available to the clinician but may not be sufficient or applicable for every patient. In such cases, intravenous conscious sedation with midazolam has been demonstrated to be safe, effective and well tolerated. The present article reviews the criteria and guidance which must be addressed by the dental team when establishing an intravenous conscious sedation service in a primary dental care setting.
CPD/Clinical Relevance: General dental practitioners may wish to consider establishing a conscious sedation service in their practices to facilitate the care of nervous patients or those undergoing prolonged, unpleasant treatments such as surgical procedures. The present paper aims to highlight the considerations which require to be addressed in order to establish such a service for adult patients using intravenous midazolam.
Article
Rebecca SL Binnie
The incidence of dental fear and anxiety is consistent worldwide.1 Although the United Kingdom (UK) was ranked second amongst European countries for the percentage of adults most likely to visit their dentist for an examination, almost half of UK adults have a fear of dental treatment, with 12% experiencing extreme and disabling anxiety.2 Acute dental fear has many effects on the delivery of dental care. Those exhibiting high levels of anxiety are less likely to attend and more likely to cancel appointments, exhibit poorer oral health and be more challenging to treat. In addition, they are often unable to give full valid consent.1,3, 4, 5 It is therefore imperative that effective anxiety management is provided for such patients.
There are a number of recognized behavioural management strategies supported by evidence which may be utilized when treating the dentally anxious. These include, but are not limited to, music, cognitive behavioural therapy (CBT), relaxation therapy and hypnosis.1,6, 7, 8 Unfortunately, for some patients, these behavioural management techniques and local analgesia alone are insufficient for them to receive dental treatment. The option and availability of conscious sedation could facilitate the provision of treatment for anxious patients who may otherwise avoid dental care. In addition, conscious sedation is indicated to support those patients undergoing more prolonged or unpleasant treatments, for example, the surgical placement of dental implants.9
What is conscious sedation?
The Academy of Medical Royal Colleges (AoMRC) published a document in 2015 entitled Safe Sedation Practice for Healthcare Procedures which defined conscious sedation as ’…a technique in which the use of a drug or drugs produces a state of depression of the central nervous system enabling treatment to be carried out, but during which verbal contact with the patient is maintained throughout the period of sedation. The drugs and techniques used to provide conscious sedation for dental treatment should carry a margin of safety wide enough to render loss of consciousness unlikely'.10 Conscious sedation can be achieved by using a range of drugs and various routes of administration.11 In the UK, conscious sedation in primary dental care is largely administered using either nitrous oxide with oxygen, known as inhalational sedation or Relative Analgesia (RA) or by using intravenous midazolam.
Midazolam
Midazolam is a benzodiazepine which works by increasing the susceptibility of the cells in the cerebral cortex to the sensory inhibitory neurotransmitter gamma-aminobutyric acid (GABA). This biochemical reduces nerve excitability resulting in the effects of sedation and muscle relaxation. It also reduces the risk of convulsions in susceptible patients. Midazolam is also associated with anterograde amnesia, a period of memory loss following the administration of the drug.12 Helpfully, this can cause patients to forget potentially psychologically traumatic procedures. However, it can also result in patients being unable to recall anything about the dental treatment. Whilst this may be seen as an advantage, there is a downside in that patients then have no memorable positive experience from which they can build for future appointments to overcome their dental phobia. Furthermore, patients may think that during subsequent sedations they are not sedated to the same depth as they were previously.
As with every drug, midazolam has some undesirable side-effects. The most significant is respiratory depression, which occurs by two mechanisms. Firstly, it decreases the sensitivity of the carbon dioxide receptors in the respiratory centre in the brainstem. Any decrease in ventilation results in increased blood carbon dioxide concentrations, which is not detected and so no compensatory increase in respiratory effort occurs. Secondly, its muscle relaxant properties affect the diaphragm and intercostal muscles which are involved in respiration.13
It is important to note that midazolam interacts with other drugs and the clinician should consult the British National Formulary (BNF) to cross-check against any other medication which the patient may be taking. Midazolam increases and prolongs serum levels of certain commonly encountered antimicrobials in dental practice, such as erythromycin, clarithromycin and fluconazole.14
The phenomenon of sexual fantasies during sedation has been reported but is not fully understood, and is often a misinterpretation of events with a correlation to higher doses.15 Females are 50% more likely than males to experience hallucinations which occur in 1 to 3% of cases with benzodiazepines.16 It is therefore imperative that a second person is present at all times in the treatment room as a chaperone to corroborate against potential allegations which may be made against any dental team member, as well as assisting in the clinical monitoring of the sedated patient.
Despite these minor problems, midazolam has been shown to be an effective and safe drug. A study of 997 patients undergoing third molar removal were randomly allocated into five groups and given different IV drugs, or a combination of drugs, for sedation. It found that commonly titrated intravenous drug regimens in dental conscious sedation, including midazolam as a single agent, produced significant anxiolysis when compared to a saline placebo group. The same study also found midazolam to produce a therapeutic benefit with minimal serious side-effects.17 A systematic review of prospective randomized controlled trials found midazolam to be safe and, as a result, the most commonly used drug to induce conscious sedation for dental procedures.11 By using intravenous titration, the clinician responsible for administering the sedation (the sedationist) is able to tailor the time of onset and depth to suit most patients and procedures.18 IV sedation using midazolam therefore lends itself to be used in general dental practice provided that the clinic is properly equipped and organized to provide this care and the staff are appropriately trained and experienced.
Setting up a sedation service
There are many benefits of having access to an in-house intravenous conscious sedation service. Firstly, as an additional service line it offers the potential to attract additional patient groups who perhaps may not be able to access dental care readily, such as the dentally anxious. Once such patients have had a positive experience, the service can become a practice-builder, as they share these experiences with others. Having an in-house service makes referrals amongst colleagues easier and quicker than referral to an external facility, particularly where a prolonged or complex treatment is being contemplated (for example, dental implant placement or a minor oral surgical procedure). With internal referrals, there are fewer communication issues as all the information relating to the patient is likely to be on the practice patient management database and readily accessible by all clinicians. Furthermore, there is no time lag in receiving emails or letters, which commonly occurs with external referrals. It also ensures a continuity of care, as patients do not have to be referred outwith the practice. This is seen as a positive by anxious patients as they particularly value the familiarity of staff and surroundings. Sedation as a service can be used to support many other treatments. Such a service can support other colleagues in other local practices as they can refer patients to the service for care.
Any sedation service must be based on a high level of safety and the delivery of care in an environment which encourages quality assurance practices.19 There are a number of aspects which must be considered prior to setting up an intravenous sedation service using midazolam in a general dental practice.
Facilities
Guidelines have been published by the Intercollegiate Advisory Committee for Sedation in Dentistry (IACSD) and the Scottish Dental Clinical Effectiveness Programme (SDCEP) which govern the provision of sedation in primary dental care.19, 20 These documents make specific recommendations regarding the environment where the service is to be provided. The treatment room should have adequate space for the clinical team to provide treatment under sedation and to carry out any emergency medical care, should this be required. Access for the emergency services to attend and to transfer the patient must be considered. It is desirable to have a designated area available where the patient can be recovered, although it is acceptable to do so in the treatment room. It is important to note that the layout and location of some practices may not lend themselves to the provision of conscious sedation due to building and other local restrictions.
Equipment
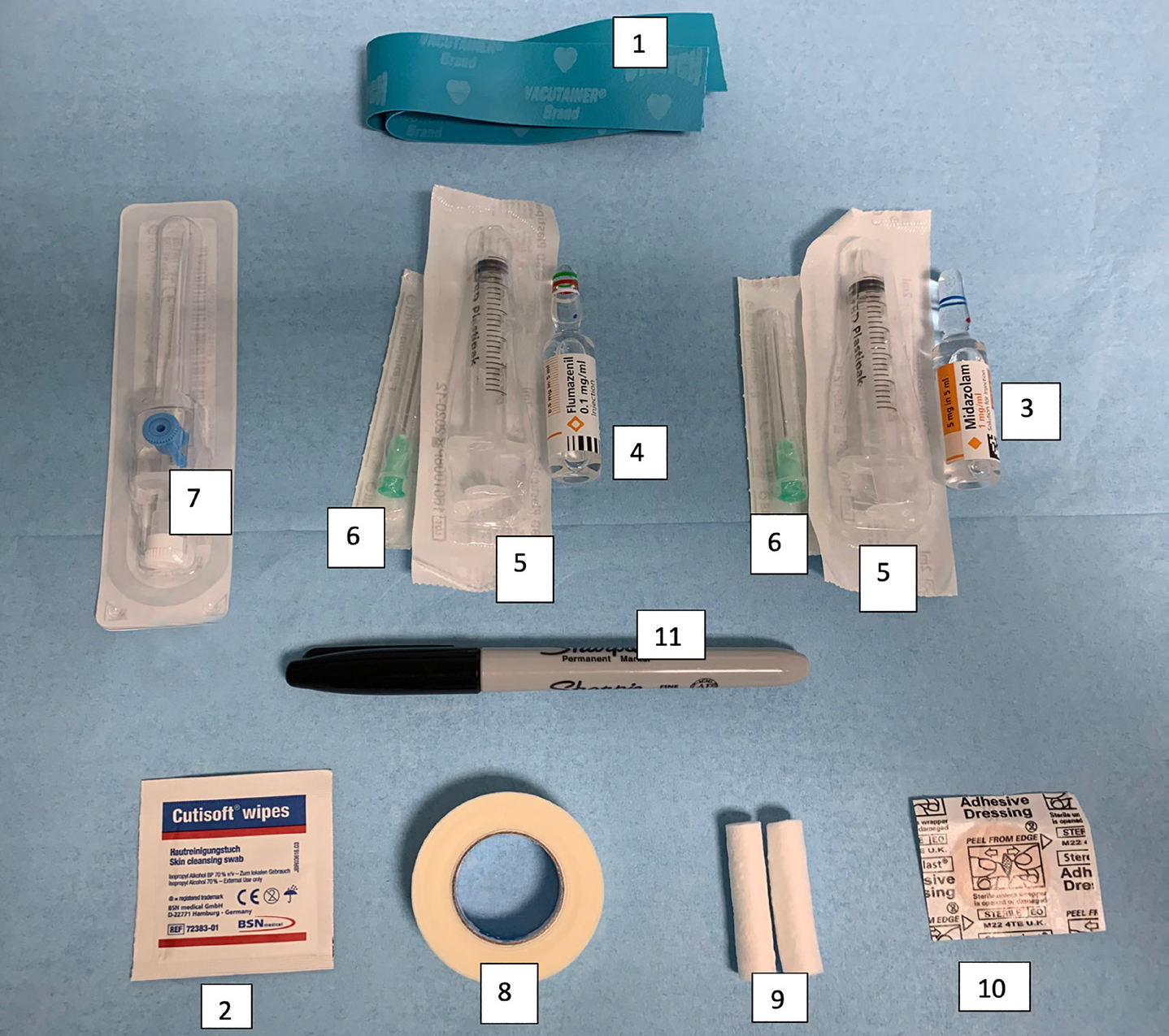
The equipment required for the pre-operative assessment, administration, monitoring and recovery of intravenous sedation with midazolam is listed in Table 1 and illustrated in Figures 1 and 2. This equipment must be suitable for purpose, calibrated and appropriately maintained.21 The Resuscitation Council (UK) stipulates the emergency equipment which must be readily available if required.22 This equipment must be checked regularly, with evidence of these checks logged in a written record which needs to be retained for purposes of audit.
Equipment Type
General
Scales
Height chart
Clock or stopwatch
Tourniquet
1
Antiseptic wipes
2
Vials of midazolam
3
Vials of flumazenil
4
Syringes (10 ml)
5
Drawing up needles (21 gauge)
6
Cannulae (25–21 gauge)
7
Non-allergenic tape
8
Cotton wool rolls
9
Adhesive dressings
10
Pen
11
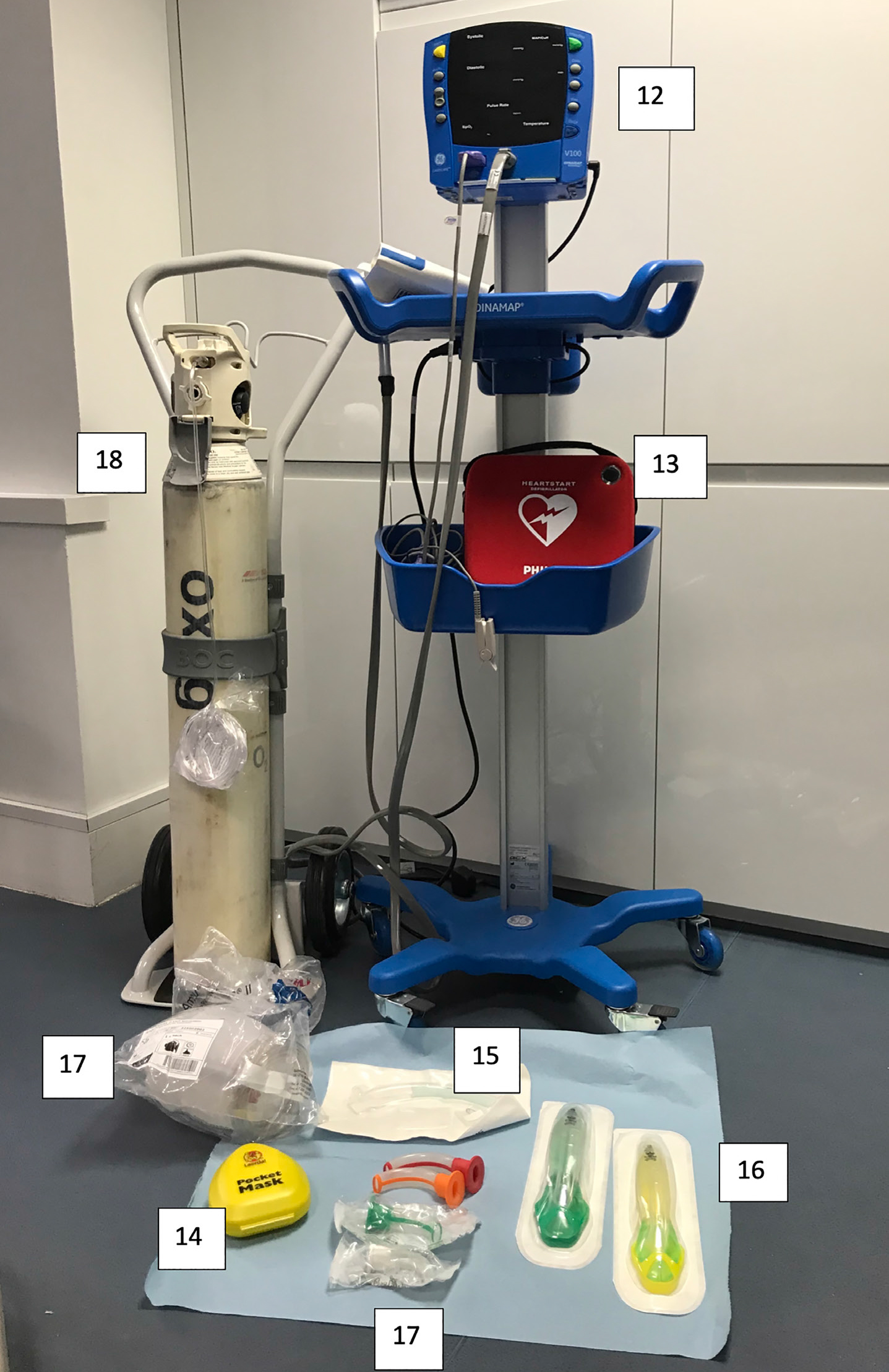
Monitoring
Pulse oximeter
12
Device for measuring blood pressure
12
Emergency
Automated external defibrillator (AED)
13
Airway management: suction
- face masks
14
- nasal cannulae
15
- oropharyngeal airways
16
- bag/mask system
17
Oxygen (‘CD' size cylinder and the ability to provide a flow of 15 litres
18
Figure 1. Examples of equipment required for IV sedation with midazolam as listed in Table 1.Figure 2. Examples of monitoring and resuscitation equipment required for IV sedation with midazolam as listed in Table 1.
Staffing
Appropriately trained and experienced staff are an essential requirement for the delivery of conscious sedation. Sedation can be provided by a dedicated sedationist or by a dental professional having the dual role of operator and sedationist with a second appropriately trained person present. This person could be a dental nurse who is competent to monitor the patient and record clinical signs at regular intervals during treatment. As two trained personnel must remain with the patient as chaperones at all times, there must be another person available to act as a runner.
Staff training
Fully trained staff underpin the safe and effective delivery of all forms of conscious sedation. The IACSD report clearly defines and establishes the standards for education and training in conscious sedation for the UK.19
Initial theory and skills training are mandatory for all staff involved in the clinical delivery and independent practice of intravenous conscious sedation by the titration of midazolam. This training can only be provided by recognized educational providers who must be accredited by an appropriate body. Training must be assessed externally, be quality assured and must support clinical supervision of a minimum of 20 cases.19 A logbook of the cases must be kept by the trainee as evidence of clinical experience and competence. An example of an appropriate logbook is available to download from The Dental Sedation Teachers Group (DSTG) website which can be found at https://www.dstg.co.uk/index.php/documents/document/sedationlogbook-doc. Full learning outcomes for the training are listed in the IACSD report Appendix 1.
Provision is made in the principal documents for experienced sedation providers to continue to practice sedation provided they can demonstrate that they have suitable experience and have maintained their knowledge and skills.19, 20 The exact criteria for relevant experience are impossible to define as specific targets or numbers for individuals do not guarantee competence.23 However, practitioners not regularly practising a technique must consider the need for mentoring or discontinuing to work in that particular sphere.19
It is the responsibility of the individual sedation team member to keep his or her skills current. A minimum of twelve hours of relevant continuing professional development (CPD) every five years is expected for all clinicians providing conscious sedation.19
In addition to the Basic Life Support required by the General Dental Council (GDC) as part of core CPD, those providing sedation must also be trained in Immediate Life Support (ILS) or equivalent. This must include maintenance of the airway and rescue measures for respiratory depression should difficulties develop. The sedation team must be able to recognize promptly a deteriorating patient and be competent in being able to manage him/her appropriately.20 Rehearsals of management of sedation-related adverse events should occur at regular intervals and evidence of such be documented in a bespoke sedation training log.
Protocols, policies and patient information
In order to provide a safe environment, strategies must be put in place to remove the possibility of risk and to keep error to a minimum. Written protocols or standard operating procedures can be helpful for the dental team to follow and their existence shows an organized approach to providing sedation. These protocols should be based on the best clinical practice and most current guidelines and be subject to regular review by the team providing the sedation service. However, such protocols should not be followed unequivocally as they do not replace individual patient assessment and careful treatment planning. The documents required are now discussed.
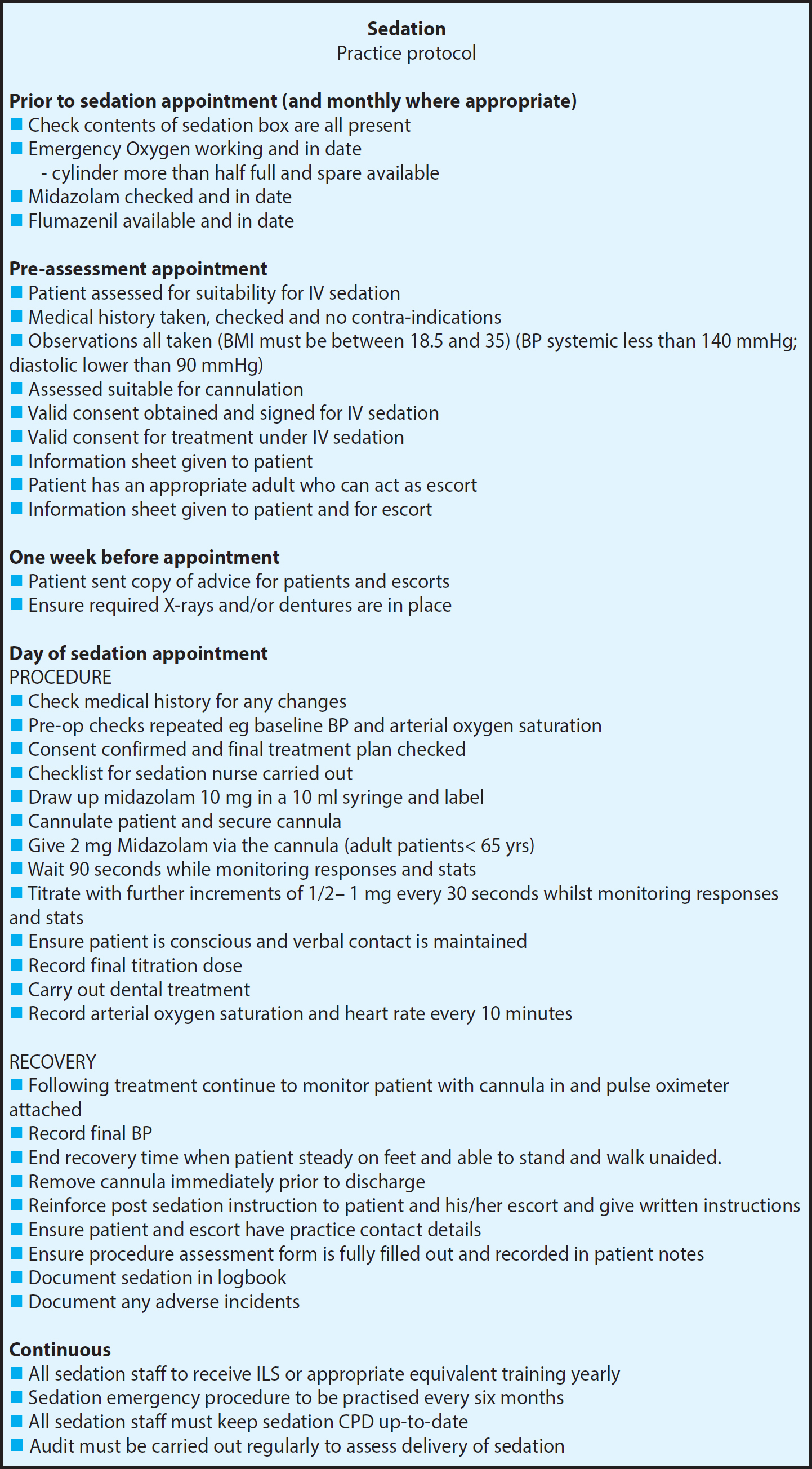
Practice sedation protocol
Any practice providing a sedation service must have a Practice Sedation Protocol in place setting out its delivery. This document should contain a common set of rules and instructions defining what is required at each stage and from each member of the sedation team. It should cover every part of the delivery of the sedation service, such as assessment, procedure, staff roles, sequence of equipment checks and steps to include clinical governance compliance.22 An example is provided in Figure 3.
Figure 3. An example of a sedation protocol for use in general dental practice.
Pre-sedation assessment
Whilst most patients can be sedated in the primary dental care setting, there are some exceptions which are listed in Table 2. Only patients graded I or II, according to the American Society of Anesthesiologists (ASA) guidelines (Table 3), are suitable to be treated in this environment.
Children under 16 years old
Cardiovascular disease
Respiratory disease
Liver disease
Kidney disease
Pregnancy
Psychiatric conditions
ASA III or above
Patients who cannot provide an escort
Uncontrolled hypertension
BMI> 35
Recreational drug users
ASA PS Classification
Definition
ASA I
A normal healthy patient
Healthy, non-smoking, no or minimal alcohol use.
ASA II
A patient with mild systemic disease
Mild diseases only without substantive functional limitations. Examples include (but not limited to): current smoker, social alcohol drinker, pregnancy, obesity (BMI >30), well controlled DM/HTN, mild lung disease.
ASA III
A patient with severe systemic disease
Substantive functional limitations: One or more moderate to severe diseases. Examples include (but not limited to): poorly controlled DM or HTN, COPD, morbid obesity (BMI ≥ 40), active hepatitis, alcohol dependence or abuse, implanted pacemaker, moderate reduction of ejection fraction, ESRD undergoing regularly scheduled dialysis, premature infant PCA < 60 weeks, history (> 3 months) of MI, CVA, TIA, or CAD/stents.
ASA IV
A patient with severe systemic disease that is a constant threat to life
Examples include (but not limited to): recent (< 3 months) MI, CVA, TIA, or CAD/stents, ongoing cardiac ischemia or severe valve dysfunction, severe reduction of ejection fraction, sepsis, DIC, ARD or ESRD not undergoing regularly scheduled dialysis.
ASA V
A moribund patient who is not expected to survive without the operation
Examples include (but not limited to): ruptured abdominal/thoracic aneurysm, massive trauma, intracranial bleed with mass effect, ischemic bowel in the face of cardiac significant pathology or multiple organ/system dysfunction.
ASA VI
A declared braindead patient whose organs are being removed for donor purposes
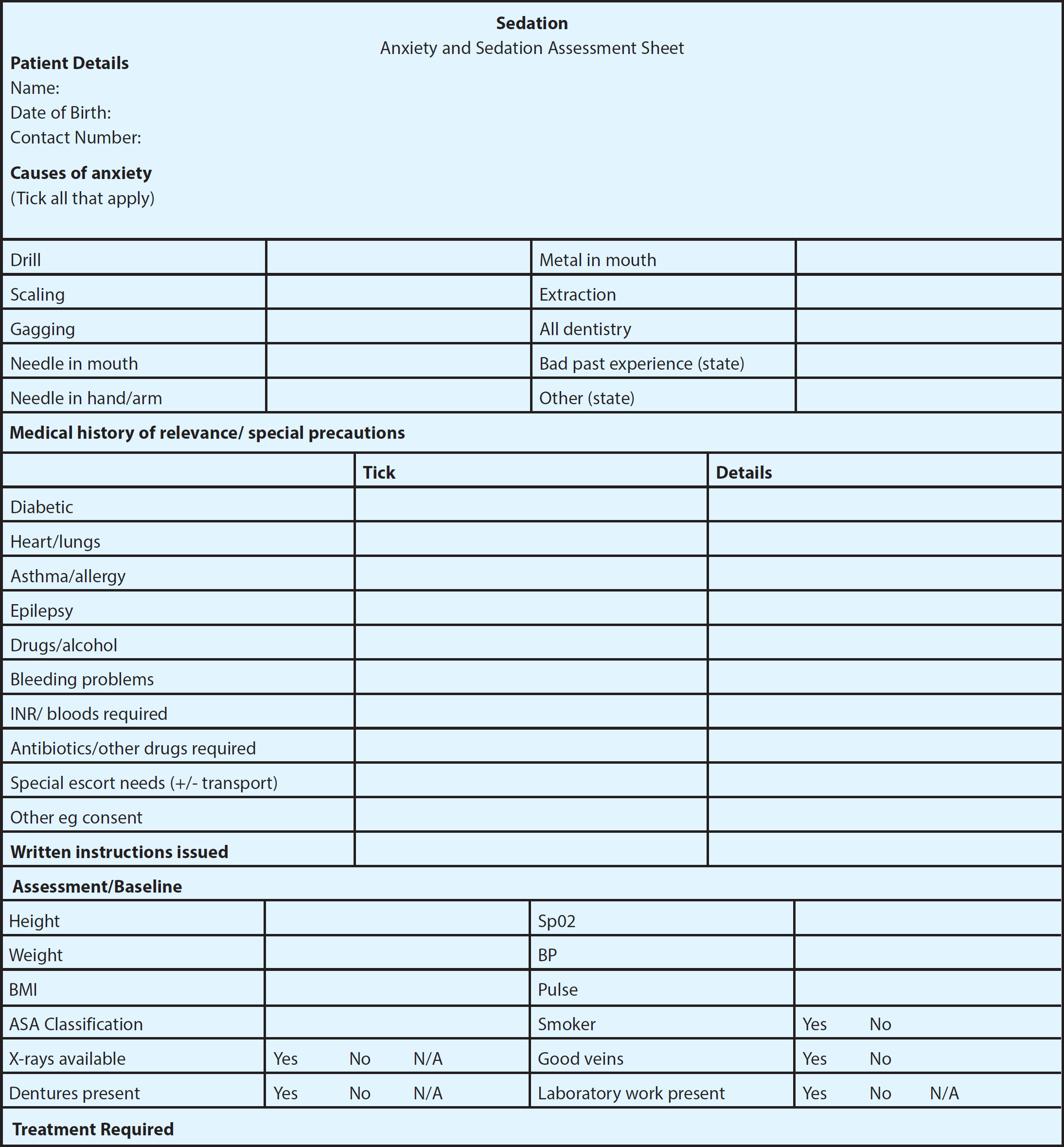
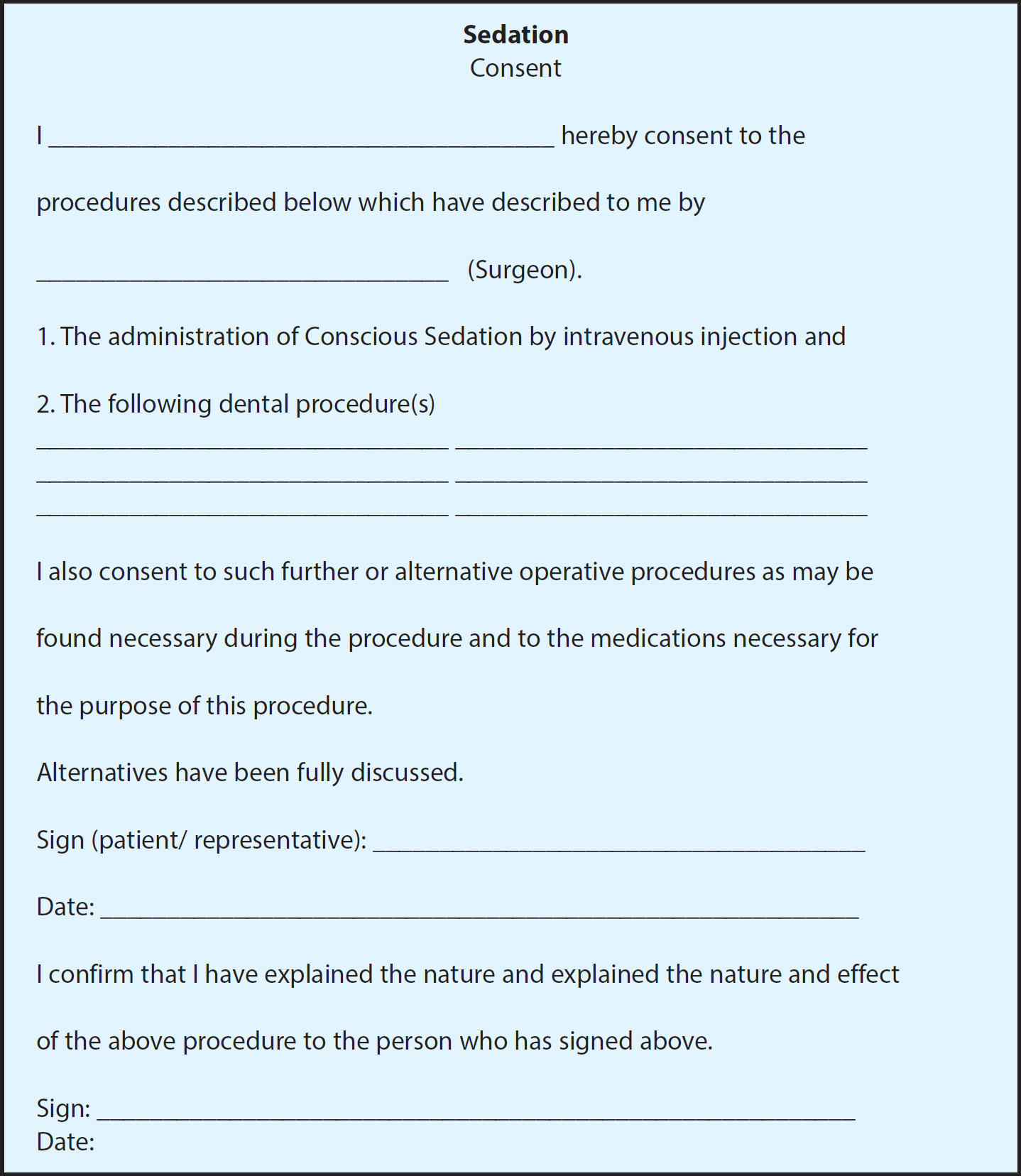
An assessment protocol (Figure 4) ensures that each patient is suitable and that conscious sedation is the correct anxiolytic management strategy. It should encourage a structured, consistent and thorough approach to ensure that all necessary clinical information is gathered, such as medical, dental, anxiety and social histories, as well as the pre-operative vital signs such as heart rate, blood pressure and oxygen saturation.20 The assessment protocol also includes a section on valid consent which must be obtained before the patient is sedated for any dental treatment. Consent must include provision for any alternative treatment should a change in the treatment plan become necessary. All options must be discussed and tailored to the needs of each individual patient.24 The risks, benefits and costs of treatment must be explained to the patient. The difference between general anaesthesia and conscious sedation must be made apparent and, particularly, that during sedation consciousness is maintained. Specific to intravenous sedation, the information provided must specify the reasons for its use, how it will be administered, the drug to be used, all associated risks and the need for an escort.19 Consent must be voluntary, and the patient must have capacity to provide consent. A sample consent form can be seen in Figure 5.
Figure 4. An example of an anxiety and sedation assessment sheet for use in general dental practice.Figure 5. An example of a consent form for sedation for use in general dental practice.
Patient information
Information must be provided to a patient prior to conscious sedation.19 This should be verbally delivered (ideally at the assessment appointment) and reinforced with written information in plain English. Information should be available in various formats and means of communication to suit the needs of the patient's level of understanding. Examples of the information patients should be provided with are contained in the IACSD document.19 Full reproduction is permissible with appropriate acknowledgment.
Escort requirements
Anyone receiving IV conscious sedation must have a suitably responsible person accompanying them, who is able to escort them home and remain with them in a supervisory capacity for the remainder of the day. Failure to provide a suitable escort has been cited as one of the most common reasons for non-compliance with sedation instructions.25 If a responsible escort cannot be found, treatment under IV sedation cannot be carried out19 and alternatives such as RA should be considered.
Fasting
The need for fasting prior to dental treatment under conscious sedation continues to be debated by both dental and anaesthetic professionals. The chief concern is aspiration. As sedation is light, verbal contact and protective reflexes are maintained, some experts consider fasting unnecessary. Furthermore, they consider that fasting may contribute to the anxiety of the patient.26 However, both the IACSD19 and the AoMRC10 refer to the potential for inadvertent over-sedation to exist, which could result in the loss of the protective airway reflexes. Careful consideration of the requirement of fasting must be made following individual patient assessment. The decision to fast or not to fast a patient must be justified and documented.19 Advice regarding fasting must be given to the patient at the assessment appointment verbally and in written form. When presenting for sedation, patients should be asked what food and fluid they have ingested that day and this should be recorded.
Monitoring protocol
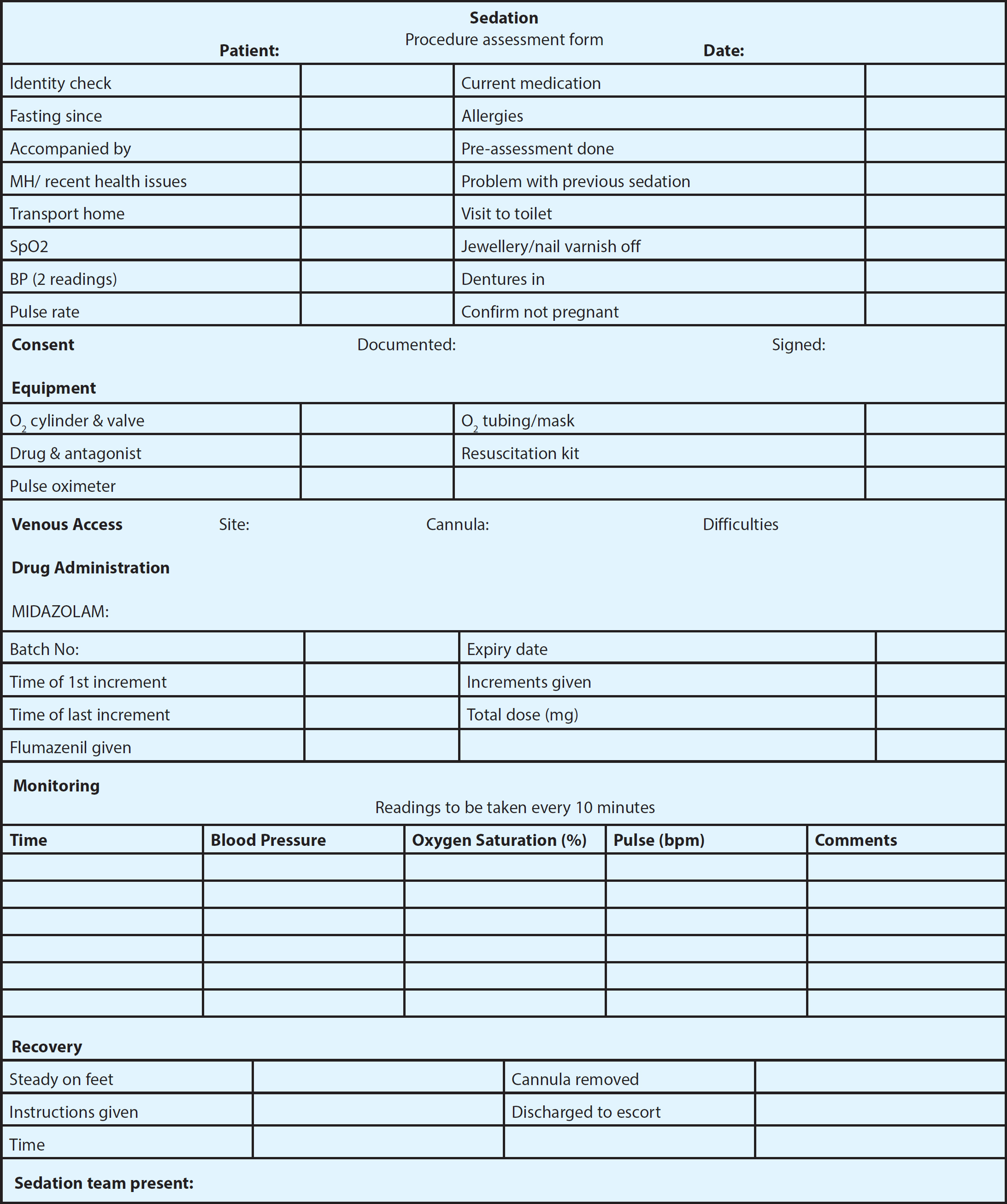
Patients receiving intravenous sedation by single drug midazolam must be monitored closely pre-, intra- and post-operatively. Non-invasive blood pressure measurements and arterial oxygen saturation levels should be recorded contemporaneously in sedation records which then form part of the patient's clinical notes.20 A list of the clinical signs to be monitored are included in Table 4, and an example of a suitable monitoring protocol is suggested in Figure 6. All members of the sedation team must be appropriately trained and competent to monitor the sedated patient.
Checking the level of consciousness/depth of sedation
Airway patency
Respiration (depth and rate)
Skin colour
Capillary refill rate
Heart rate, rhythm and volume
Non-invasive blood pressure
Oxygen saturation (via pulse oximetry with visual display and audible alarm
Figure 6. An example of a form used to record the patient's clinical signs during the procedure.
Medical emergency protocol
Whilst the incidence of an adverse medical event occurring is rare during conscious sedation, the practice's emergency protocol must be readily available to assist should one arise. Each member of the clinical team must know his/her role in the event of an emergency. This should include resuscitation, notification of the emergency services and maintenance of the patient until he/she is transferred to hospital, if deemed necessary.
Reversal of the anxiolytic, sedative and respiratory effects of midazolam can be achieved by the administration of flumazenil, a benzodiazepine antagonist. Although its routine use is discouraged, it can be used for both emergency and elective reversal of sedation. Flumazenil has no apparent sedative effects of its own but has a greater affinity for the receptors and will displace other agonists.
Aftercare and restrictions
Recovery from the administration of midazolam is gradual, progressive and does not end when the patient is permitted to return home.27 Short-term recovery is dependent upon the redistribution of the drug from the receptor sites, with long-term recovery following metabolism and excretion.28 There is individual variation as to the time taken for recovery. Dixon et al found two thirds of patients were not recovered 30 minutes after the end of the treatment session.29 Sedationists need to allow for sufficient recovery time when planning appointments.
Initially, recovery must be under the care of the trained sedation team, with the equipment and drugs to manage any complications immediately available and the patient monitored until deemed fit to be discharged to the responsibility of his/her escort. The decision to discharge rests with the sedationist and should follow an assessment where discharge criteria are met. These criteria are listed in Table 5.
Patient is orientated in time, place and person
Vital signs are normal and stable with respiratory status not compromised
Pain and comfort addressed and arrangements for post-operative analgesia where necessary
Haemostasis achieved where necessary
Any cannula inserted has been removed
The responsible escort is present and informed regarding supervisory responsibilities
Verbal and written instructions given regarding the sedation, dental treatment undertaken and advice regarding precautions in the post-sedation period
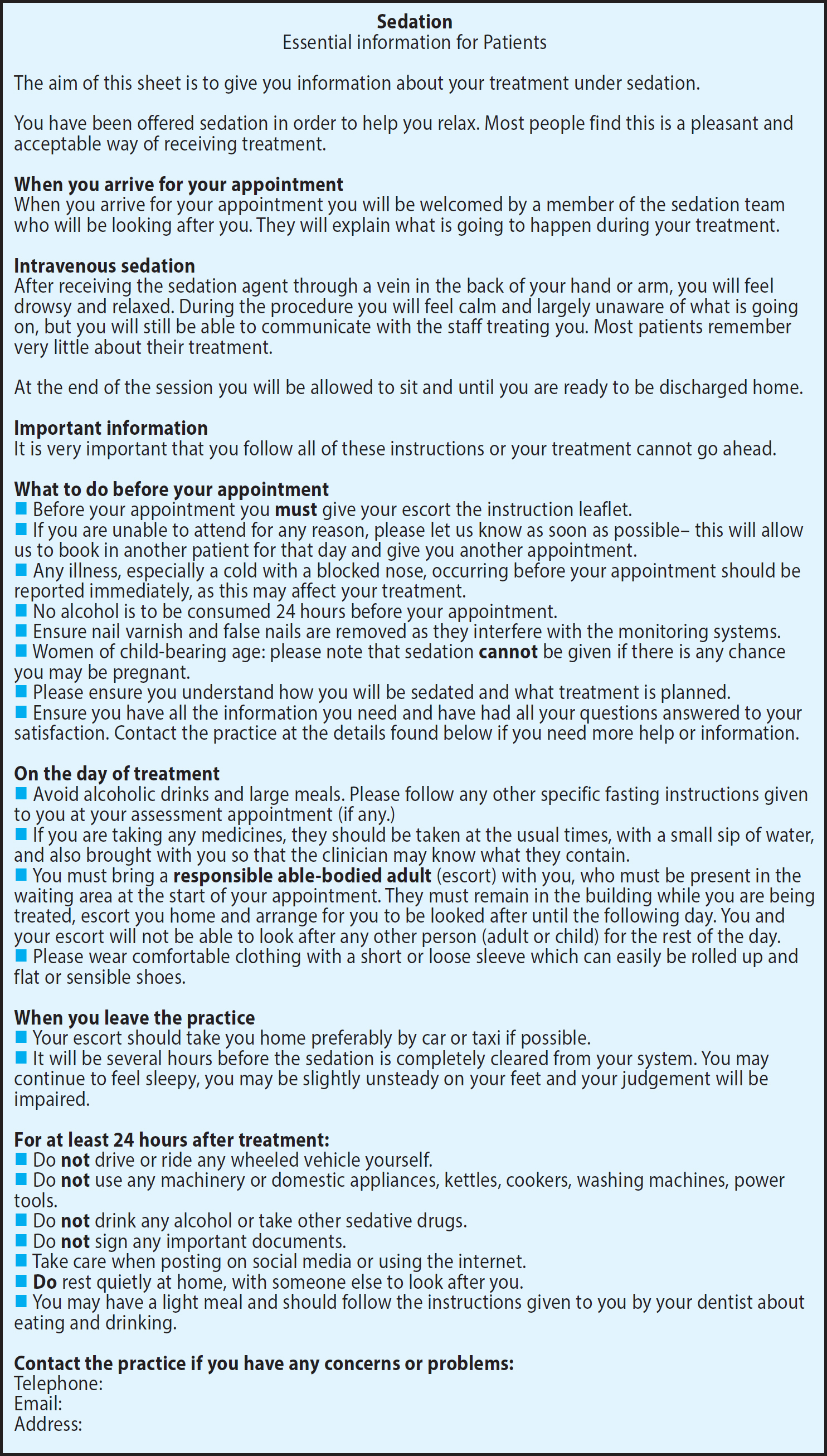
Relevant written information must supplement verbal instructions given to both the patient and escort. Precautions regarding the avoidance of alcohol, driving, important decision-making, signing of legal documents and the operating of machinery must be made clear.19 It may also be prudent to advise against the use of social media and online shopping until such times as the patient has fully recovered. Aftercare advice, including instructions regarding the patient's regular medication, restrictions on post-sedation activities, contact details for further advice or in case of emergency should be provided. This advice is shown in Figure 7.
Figure 7. Information for patients undergoing IV sedation using midazolam in general dental practice.
Sedation record log
A logbook must also be kept for all sedation cases undertaken by the sedation team. The log can be in hard copy or electronic form but must include continuous and contemporaneous records of the number and type of sedation cases. It should also include a list of any adverse events or deviations from standard practice, such as the emergency use of flumazenil.19
Guidelines
Guidance for conscious sedation varies internationally and those providing sedation must refer to the guidance of the country in which they are practising.30 When planning and establishing a new sedation service in a UK dental practice it is crucial to adhere to the current guidance set out in the IACSD and SDCEP documents.19, 20
In addition to sedation specific documents, the provision of conscious sedation falls under the umbrella of other important guidelines and standards. In the UK, the GDC's 2013 document Standards for the Dental Team31 must be adhered to and The Resuscitation Council (UK)'s Quality Standards for Cardiopulmonary Resuscitation Practice and Training Primary Dental Care22 should also be carefully followed.
Quality assurance
In order to provide a safe sedation service, it is imperative that the activity is quality assured. This is done by the inspection of the facilities and documentation in the form of practice inspections and also by carrying out regular audit.
Practice inspections
Formal evaluation of dental sedation services is recommended.20 The SAAD website contains helpful downloadable checklists to help ensure compliance which can be found at https://saad.org.uk/index.php/documents
SAAD has also produced a quality assurance programme to support an evaluation process and this includes an inspection of all the sedation processes and observations of technique.30
Clinical governance and audit
High quality regular audit is expected when delivering conscious sedation with all members of the team participating.19 The focus of audit projects should concentrate on the outcomes of procedures and processes. These audits and any modifications so identified from their analysis must be documented and maintained for inspection.
Systems must be in place to report and investigate critical incidents, as outlined in the AoMRC publication, Safe Sedation Practice for Healthcare Procedures.10
Investigation and significant event analysis in a sedation service should follow adverse events, such as those listed in Table 6. The Safe Anaesthesia Liaison Group (SALG) supports the reporting of specific incidents for the purpose of learning and patient safety, for example, midazolam over-sedation and failure to monitor oxygen saturation. Their website includes an e-form for confidential reporting.32 The use of this link and the reporting of incidents is supported by both the IACSD and the AoMRC. However, reporting incidents can only follow the recognition and management of such events and this relies on fully trained and competent staff.
Use of flumazenil to reverse sedation
Midazolam over-sedation
Sustained drop in oxygen saturation below 90%
Unplanned intervention of the airway
Unplanned hospital admission subsequent to the sedation
Failure of conscious sedation
Delayed recovery
Vomiting, choking or idiosyncratic responses
Conclusion
Dental anxiety is commonly encountered in the general population and can be a barrier to the provision of care for some patients. The establishment of a sedation service in the primary dental care setting can facilitate care for these patients and also those who need to undergo a prolonged or unpleasant procedure. There are a number of considerations which the interested practitioner needs to address prior to, and during the provision of, a conscious sedation service using intravenous midazolam. This technique has been demonstrated to be effective and well tolerated. It can be a practice builder by increasing patient numbers, both by direct and indirect referral and by increasing complex treatment uptake.