Davis PJ, Brook AH. The presentation of talon cusp: diagnosis, clinical features, associations and possible aetiology. Br Dent J. 1986; 160:(3)84-88
Buenviaje TM, Rapp R. Dental anomalies in children: a clinical and radiographic survey. ASDC J Dent Child. 1984; 51:(1)42-46
Chawla HS, Tewari A, Gopalakrishnan NS. Talon cusp – a prevalence study. J Indian Soc Pedod Prev Dent. 1983; 1:(1)28-34
Mellor JK, Ripa IW. Talon cusp: a clinically significant anomaly. Oral Surg Oral Med Oral Pathol. 1970; 29:225-228
Hattab FN, Yassin OM, al-Nimri KS. Talon cusp in permanent dentition associated with other dental anomalies: review of literature and reports of seven cases. ASDC J Dent Child. 1996; 63:(5)368-376
Sumer AP, Zengin AZ. An unusual presentation of talon cusp: a case report. Br Dent J. 2005; 199:(7)429-430
Ekambaram M, Yiu CK, King NM. An unusual case of double teeth with facial and lingual talon cusps. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 105:(4)e63-67
Hegde S, Kumar BR. Mandibular talon cusp: report of two rare cases. Int J Paediatr Dent. 1999; 9:(4)303-306
Chen RJ, Chen HS. Talon cusp in the primary dentition. Oral Surg Oral Med Oral Pathol. 1986; 62:67-72
Gardner DG, Girgis SS. Talon cusps: a dental anomaly in the Rubinstein-Taybi syndrome. Oral Surg Oral Med Oral Pathol. 1979; 47:(6)519-521
Goldstein E, Medina JL. Mohr syndrome or oral-facial digital II: report of two cases. J Am Dent Assoc. 1974; 89:377-382
Dash JK, Sahoo PK, Das SN. Talon cusp associated with other dental anomalies: a case report. Int J Paediatr Dent. 2004; 14:(4)295-300
Dayal PK, Mani NJ, Verma PK. Talon cusp: a review and case report. J Dent. 1980; 8:(1)85-87
Lomçali G, Hazar S, Altinbulak H. Talon cusp: report of five cases. Quintessence Int. 1994; 25:(6)431-433
Gündüz K, Celenk P. Survey of talon cusps in the permanent dentition of a Turkish population. J Contemp Dent Pract. 2008; 9:(5)84-91
Rantanen AV. Talon cusp. Oral Surg Oral Med Oral Pathol. 1971; 32:(3)398-400
Brin I, Becker A, Shalhav M. Position of the maxillary permanent canine in relation to anomalous or missing lateral incisors: a population study. Eur J Orthod. 1986; 8:(1)12-16
Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994; 64:(4)249-256
Peck L, Peck S, Attia Y. Maxillary canine-first premolar transposition, associated dental anomalies and genetic basis. Angle Orthod. 1993; 63:(2)99-109
Nadkarni UM, Munshi A, Damle SG. Unusual presentation of talon cusp: two case reports. Int J Paediatr Dent. 2002; 12:(5)332-335
Mader CL. Mandibular talon cusp. J Am Dent Assoc. 1982; 105::651-653
Kjaer I. Morphological characteristics of dentitions developing excessive root resorption during orthodontic treatment. Eur J Orthod. 1995; 17:(1)25-34
Lee RY, Artun J, Alonzo TA. Are dental anomalies risk factors for apical root resorption in orthodontic patients?. Am J Orthod Dentofacial Orthop. 1999; 116:(2)187-195
The talon cusp – an uncommon anomaly J Seehra F Coutts Dental Update 2024 39:4, 707-709.
Authors
JSeehra
BDS(Hons), MFDS RCS, MSc, MOrth RCS(Eng)
Senior Registrar in Orthodontics, Department of Orthodontics and Paediatrics, Guy's and St Thomas's NHS Foundation Trust, Floor 22, Guy's Tower London SE1 9RT
Consultant Orthodontist, Maxillofacial Unit, East Kent Hospitals University NHS Foundation Trust, William Harvey Hospital, Kennington Road, Willesborough, Ashford, Kent TN24 0LZ, UK
Talon cusps are an uncommon dental anomaly of odontogenic origin. Talon cusps can also present with other dental anomalies, however these have been infrequently reported in the literature. The following is a report of two cases in which talon cusps were detected in combination with two distinct dental anomalies: an ectopic canine and transposition.
Clinical Relevance: It is important to recognize that the management of talon cusps may require a multidisciplinary approach and should be considered during treatment planning.
Article
A talon cusp is a rare dental anomaly of odontogenic origin first reported by Mitchell in 1892.1 The prevalence has been reported at 0.012%,2 0.17%3 and 7.7%.4 Davies and Brook2 defined a talon cusp as:
…an additional cusp that prominently projects from the lingual surface of primary or permanent anterior teeth, is morphologically well-delineated, and extends at least half the distance from the cement-enamel junction to the incisal edge.
The resemblance to an eagle's talon is a reflection of the shape of this anomaly.5
Both genetic and environmental factors have been suggested as aetiological factors. The reported incidence is higher in males than females. Typically, talon cusps can present on the palatal or lingual aspect of the incisors, and occur more frequently in the maxillary dentition, with the maxillary lateral incisor the most commonly affected tooth.2,5,6 Labial talon cusps have, however, also been reported.7,8 Talon cusps can also be found in both permanent and primary teeth9,10 and associated with syndromes such as Sturge-Weber,10 Rubinstein-Taybi11 and Mohr syndromes.12
Talon cusps can also present with other dental anomalies. Davies and Brook,2 in a review of 20 cases of talon cusps, reported individual cases of both transposition of LR2 and LR3 and a supernumerary. Other anomalies include: peg-shaped lateral incisor,5 hypodontia,9,13 impacted canine,14 and double teeth.15,16 Interestingly, hyperactivity of the dental lamina has been postulated as an aetiological factor of talon cusps,17 which is also implicated in the aetiology of double teeth and supernumerary teeth. Overall, the prevalence of talon cusps with other dental anomalies is rare.
The following is a report of two cases in which talon cusps were detected in combination with two distinct dental anomalies.
Case 1
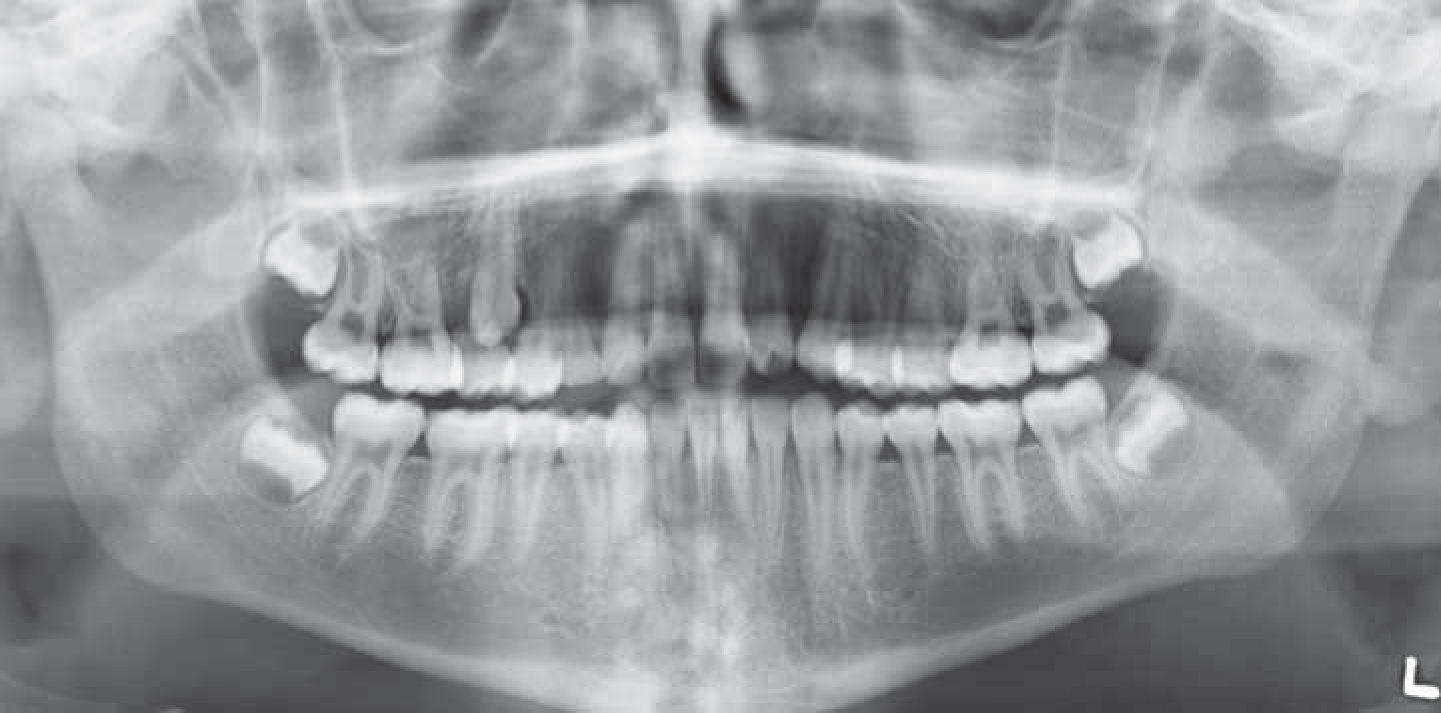
A medically fit and well 13-year-old male was referred to the orthodontic department by his general dental practitioner for advice regarding the unerupted UR3. The patient presented with a Class I incisor relationship on a skeletal I pattern with an average lower facial height and maxillary mandibular planes angle. On examination both the upper and lower labial segments were of average inclination with mild crowding of the upper labial segment. An overjet of 3 mm was measured and the overbite was reduced and incomplete. The UR3 was palpated buccally between the UR4 and UR5 (Figure 1). Radiographic investigations confirmed the diagnosis of transposition of the UR3 (Figure 2). A notable finding was the presence of a talon cusp associated with the UL2. Oral hygiene was of optimal standard. No caries or pathology was evident in the UL2, despite a stained fissure associated with the talon cusp.
Figure 1. Case 1: Upper occlusal view demonstrating the talon cusp associated with the UL2.Figure 2. Case 1: OPG radiograph confirming the transposition of the UR3 and UR4. The outline of the UL2 talon cusp is also visible.
Case 2
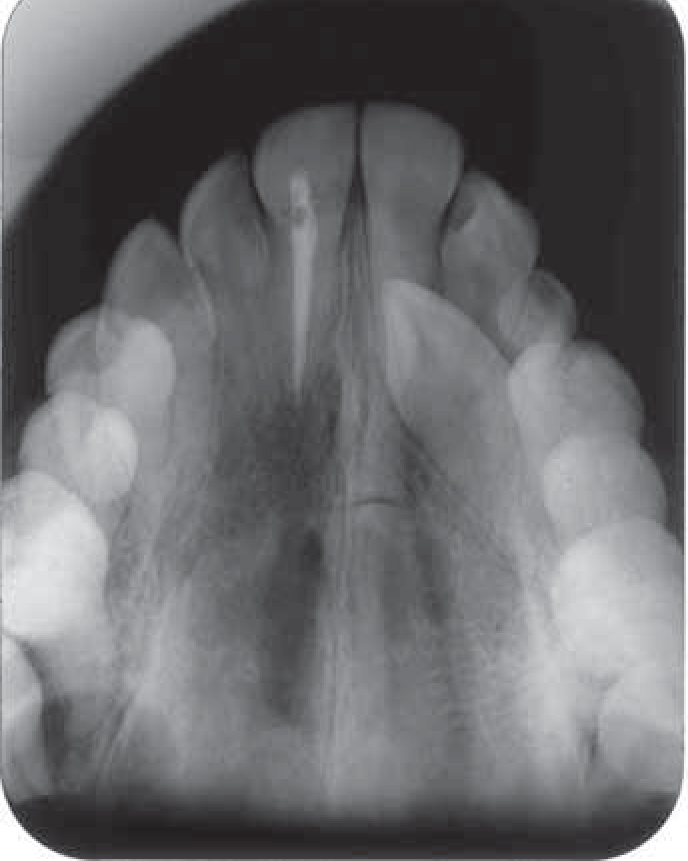
A 14-year-old male was referred to the orthodontic department by his general dental practitioner for advice regarding the palatally ectopic UL3. The patient presented with a Class I incisor relationship on a mild skeletal III pattern with an increased lower facial height and maxillary mandibular planes angle. On examination, both the upper and lower labial segments were of average inclination. The overbite was average and complete and an overjet of 2 mm was measured. Clinically, the UL3 was palpated palatally (Figure 3). Radiographic investigations confirmed the diagnosis of a palatally ectopic UL3 (Figure 4). An interesting finding was the presence of a talon cusp associated with the UL2. Oral hygiene was of moderate standard and no pathology was evident in the UL2.
Figure 3. Case 2: Upper occlusal view demonstrating the talon cusp associated with the UL2.Figure 4. Case 2: Upper standard occlusal radiograph clearly demonstrating the talon cusp associated with the UL2.
Discussion
The reported variation in prevalence rates of talon cusps within the literature can be explained by the use of differing classifications and diagnostic criteria employed by authors. In both reported cases, the definition as proposed by Davies and Brook2 was used. As indicated, the diagnosis of a talon cusp is primarily made from the clinical examination. Usually a projection from the lingual or palatal aspect of the affected tooth is evident. Radiographically, a radio-opaque structure is visible as demonstrated by Figure 4. Histologically, talon cusps contain dentine, enamel and varying extensions of pulpal tissue.5,6 The maxillary lateral incisor has been reported to be the commonest tooth involved6 and the talon cusps in both of these cases were associated with the UL2. In addition, talon cusps appear to predominate on the left-side of the arch.2 Interestingly, anomalous upper maxillary lateral incisors have been associated with palatally ectopic canines,18 suggesting this could have been a factor in Case 2. A genetic component has been reported as an aetiological factor in both palatally ectopic canines19 and transpositions.20 Factors such as gender difference, predominance of a particular side of an arch and individual tooth affected and association with other dental anomalies and syndromes are frequently reported as indicators of a genetic aetiology.
Although the majority of talon cusps are asymptomatic in nature, the presence of a deep developmental groove renders these teeth susceptible to caries and is of clinical significance.2,5 In addition, talon cusps can act as an occlusal interference,21 cause irritation to soft tissues22 and compromise aesthetics.8 They can also potentially complicate diagnosis, especially when the affected tooth is unerupted or partially erupted. In this situation, the talon cusp can mimic a supernumerary tooth.2
The management of talon cusps varies according to the clinical presentation. A conservative approach is indicated if the aesthetic appearance is satisfactory with no associated pathology.22 If a deep developmental groove is present, prophylactic restorations are recommended to prevent caries progression.5 If the talon cusp is of aesthetic concern or causing an occlusal interference, selective grinding and recontouring can be performed. Gradual removal of small increments of tooth tissue is recommended to reduce the incidence of pulpal exposure. In the event of exposure, root canal therapy is indicated.5
Root resorption as a result of orthodontic forces is an inevitable consequence of orthodontic treatment. Anomalous incisors have been reported to be at increased risk of root resorption compared to teeth with normal morphological features. Kjaer23 reported teeth with invaginations and taurodontism to be at greater risk of root resorption. The converse is reported by Lee et al24 who demonstrated no increased risk of root resorption. In view of equivocal results, the effect of orthodontic forces on anomalous incisors and their root length cannot be reliably predicated, however, it may be prudent to warn consenting patients of the possible risk and to monitor these teeth radiographically during appliance therapy.
Talon cusps are a rare dental anomaly containing odontogenic tissue with a multifactorial aetiology. The detection of such cusps should alert the clinician to the possibility of other associated anomalies, including ectopic canines and transpositions. The treatment of teeth with talon cusps should involve optimizing oral hygiene and may include a multidisciplinary approach.