Mendieta C, Gonzalez-Blanco A. Supernumerary teeth and localized juvenile periodontitis: a review of the literature and case report. Periodont Case Rep. 1988; 10:23-27
Odell EW, Hughes FJ. The possible association between localized juvenile periodontitis and supernumerary teeth. J Periodontol. 1995; 66:449-451
Açikgöz A, Ozden FO, Fisgin T Oral and dental findings in Fanconi's anemia. Pediatr Hematol Oncol. 2005; 22:531-539
Rubin MM, Nevins A, Berg M, Borden B. A comparison of identical twins in relation to three dental anomalies: multiple supernumerary teeth, juvenile periodontosis, and zero caries incidence. Oral Surg Oral Med Oral Pathol. 1981; 52:391-394
Kaslick RS, Chasens AI. Periodontosis with periodontitis: a study involving young adult males II. Clinical, medical, and histopathologic studies. Oral Surg Oral Med Oral Pathol. 1968; 25:327-350
Casavecchia P, Uzel MI, Kantarci A Hereditary gingival fibromatosis associated with generalized aggressive periodontitis: a case report. J Periodontol. 2004; 75:770-778
Jadwat Y, Anagnostopoulos C, Wood NH, Lemmer J, Meyerov RH, Feller L. Localized aggressive periodontitis associated with unusual gingival enlargement posing a diagnostic dilemma: a case report. SADJ. 2008; 63:230-232
Nitta H, Kameyama Y, Ishikawa I. Unusual gingival enlargement with rapidly progressive periodontitis. Report of a case. J Periodontol. 1993; 64:1008-1012
Bökenkamp A, Bohnhorst B, Beier C, Albers N, Offner G, Brodehl J. Nifedipine aggravates cyclosporine A-induced gingival hyperplasia. Pediatr Nephrol. 1994; 8:181-185
Açikgöz G, Açikgöz A, Keskiner I, Türk T, Otan F. Aggressive periodontitis with supernumerary teeth: a retrospective study. J Periodontol. 2004; 75:1458-1460
Akincibay H, Orsal SO, Sengün D, Tözüm TF. Systemic administration of doxycycline versus metronidazole plus amoxicillin in the treatment of localized aggressive periodontitis: a clinical and microbiologic study. Quintessence Int. 2008; 39:33-39
Saglie FR, Marfany A, Camargo P. Intragingival occurrence of Actinobacillus actinomycetemcomitans and Bacteroides gingivalis in active destructive periodontal lesions. J Periodontol. 1988; 59:259-265
Tonetti MS, Mombelli A. Aggressive periodontitis, 5th edn. In: Lang Niklaus P, Lindhe Jan Oxford: Blackwell Publishing Ltd; 2008
Slots J. Research, Science and Therapy Committee. Systemic antibiotics in periodontics. J Periodontol. 2004; 75:1553-1565
Bidault P, Chandad F, Grenier D. Systemic antibiotic therapy in the treatment of periodontitis. J Can Dent Assoc. 2007; 73:515-520
This case report describes the management of an 18-year-old female who presented with generalized aggressive periodontitis, gingival enlargement and a mesiodens. Diagnosis for aggressive periodontitis was determined based on history, clinical findings and radiographic examination. Treatment included oral prophylaxis, extraction of the mesiodens and elimination of infectious micro-organisms, using a combination of surgical intervention and antimicrobial therapy with long-term maintenance.
Clinical Relevance: Presence of gingival enlargement in cases of aggressive periodontitis may be clinically confusing; hence, the diagnosis should always be based on the patient's history as well as the clinical and radiographic findings.
Article
Aggressive periodontitis is an inflammatory disease, with onset during early adult years, and is characterized by rapid, severe destruction of periodontal tissues, including the alveolar bone, in apparently healthy young adults.1 Aggressive periodontitis usually presents with gingival tissues that are free of inflammation, despite the presence of deep periodontal pockets.1 Diagnosis in cases of aggressive periodontitis is important as bone loss progresses rapidly, and these cases do not respond to conventional therapy. Supernumerary teeth with aggressive periodontitis have been noted in case reports.2–7 Gingival enlargementassociated with aggressive periodontitis is rare.8–10 In this case report, we present the management of a patient with generalized aggressive periodontitis associated with generalized gingival enlargement and mesiodens.
Aggressive periodontitis occurs in localized and generalized forms. Localized aggressive periodontitis usually has a circumpubertal onset with periodontal damage being localized to permanent first molars and incisors.1 However, atypical patterns are possible. The disease is frequently associated with the periodontal pathogen Aggregatibacter actinomycetemcomitans (previously Actinobacillus actinomycetemcomitans) and neutrophil function abnormalities. A robust serum antibody response to infecting agents is frequently detected. Generalized aggressive periodontitis usually affects people under 30 years of age, but patients may be older. There is generalized interproximal attachment loss affecting at least three permanent teeth other than the first molars and incisors.1 Attachment loss occurs in pronounced episodic periods of destruction.
Patients with generalized aggressive periodontitis tend to have a poorer prognosis because they typically have more teeth affected by the disease and because the disease rarely undergoes spontaneous remission, whereas localized forms of the disease have been known to arrest spontaneously.1
Case description
An 18-year-old female presented to the department of periodontics with a chief complaint of gingival swelling and bad breath for the previous two years. The patient was concerned about the progressively increasing spacing between her maxillary anterior teeth. Family history revealed that the patient's mother had generalized aggressive periodontitis (diagnosis was based on clinical and radiographic examinations). Routine blood investigations of the patient showed a normal blood profile. On intra-oral examination, minimal amounts of plaque and calculus were observed, whereas moderate accumulation of deposits were seen in the mandibular anterior region. A peg-shaped supernumerary tooth was noted between the maxillary central incisors (Figures 1–3). Angle's Class I molar relation with spacing in the maxillary anterior segment and a deep overbite was present.
Figure 1. Mesiodens and gingival enlargement noted in an 18-year-old female with generalized aggressive periodontitis.Figure 2. Aggressive periodontitis with gingival enlargement (right lateral view).Figure 3. Aggressive periodontitis with gingival enlargement (left lateral view).
On examination, the gingiva was pale pink with bright red margins in the anterior region, with scalloped contour and rolled margins. Generalized grade II gingival enlargement was noted, which was diffuse and combined (inflammatory and fibrous).11 Full-mouth periodontal charting, including assessment of probing depth and clinical attachment level, revealed deep pockets throughout the mouth with a basic periodontal examination system code 4 of all the sextants. Further periodontal examination revealed distolabial migration of the maxillary central and lateral incisors (based on the history of movement of these teeth away from their original positions). Grade II mobility was observed in the mandibular incisors.
An orthopantomograph revealed classic arc-shaped bone loss around the maxillary and mandibular first molars (mirror image). Generalized interproximal bone loss and furcation involvement was observed in the maxillary and mandibular first molars (Figure 4). Bone loss was also noticed around mandibular and maxillary anterior teeth. Based on the family history as well as clinical and radiographic findings, a diagnosis of generalized aggressive periodontitis with inflammatory gingival enlargement was made. A treatment plan was formulated, explained to the patient, and informed consent was obtained.
Figure 4. Orthopantomograph showing arc-shaped bone loss in relation to first molars and generalized interproximal bone loss.
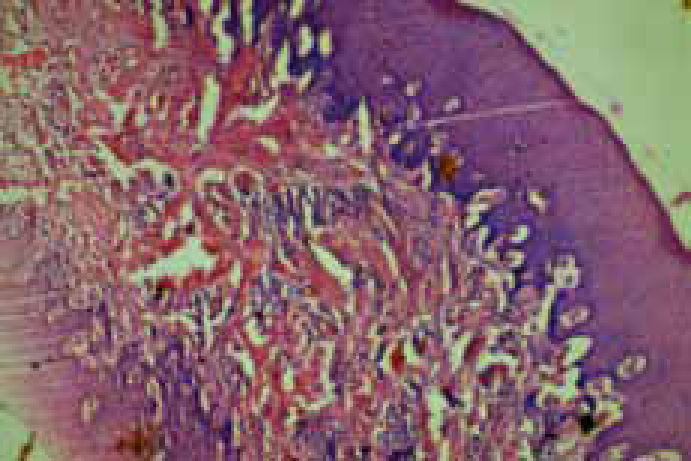
The patient initially underwent phase 1 periodontal therapy that included oral hygiene instruction and reinforcement and evaluation of the patient's plaque control; extraction of the mesiodens, supra and subgingival scaling and root planing to remove microbial plaque and calculus. Adjunctive antimicrobial therapy, which consisted of Doxycycline 200mg stat and 100mg for the following four days, was advised along with mechanical therapy. Phase 2 therapy involved periodontal surgery under local anaesthesia in all four quadrants with internal bevel gingivectomy combined with open-flap debridement. Excised gingiva was submitted for histopathologic examination, which revealed epithelial hyperplasia with an abundance of fibroblasts and inflammatory cells in the connective tissue (Figure 5). The patient continues to be followed-up and has had no recurrence of the gingival enlargement (Figures 6–8). At the completion of one year, periodontal health was stabilized, with reduction in probing depths around all the teeth. The patient was referred for orthodontic correction of the deep bite, space closure and is currently being treated (Figure 9).
Figure 5. Photomicrograph showing epithelial hyperplasia with inflammatory cell infiltration in the connective tissue (H and E 40X).Figure 6. Post-operative photograph. Inset shows the extracted mesiodens.Figure 7. Post-operative photograph (right lateral view).Figure 8. Post-operative photograph (left lateral view).Figure 9. Orthodontic treatment is being carried out.
Discussion
Aggressive periodontitis progresses rapidly, destroying the underlying periodontium and causing severe bone loss.1 Owing to minimal clinical symptoms in the initial stages, cases are often detected after significant destruction of the periodontium, which sometimes leaves the clinician with no other option than extraction.1 Diagnosing the cases at a very early stage and providing comprehensive periodontal therapy with adjunctive antimicrobial therapy is the best management solution.1
Supernumerary teeth are common and seen more often in the maxilla compared to the mandible.4 The presence of supernumerary teeth in aggressive periodontitis has been reported.4 Eley reported a case of a female with juvenile periodontitis (now called aggressive periodontitis) and four supernumerary molars.2 Odell and Hughes reported two cases of localized aggressive periodontitis with supernumerary teeth.4 In one of the cases, a small odontome/supernumerary tooth comprising two premolariform tooth crowns in a single crypt was seen between the root apices of the lower right premolars.4 The other case revealed a single peg-shaped supplemental premolar lying between the roots of the upper left premolars with a short but fully formed root.4 On the right side, a cluster of three small tooth crowns, two premolariform and one peg-shaped, were present in a single crypt adjacent to the premolar roots.4 Açikgöz et al have reported two cases of aggressive periodontitis, with one case showing hyperdontia and the other indicating hypodontia.5 Kaslick and Chasens noted one black patient with multiple supernumerary teeth; however, this report did not have any radiographs, and the sites and types of supernumeraries were not described.7
In a retrospective study by Açikgöz et al, 5850 participants were screened for the presence of supernumerary teeth with aggressive periodontitis. There were 174 with supernumerary teeth, whereas only three patients had aggressive periodontitis. The study concluded that association of supernumerary teeth in aggressive periodontitis might occur randomly rather than biologically.12
Aggressive periodontitis is rarely associated with gingival enlargement.8 Casavecchia et al reported a case of hereditary gingival fibromatosis with aggressive periodontitis.8 Jadwat et al reported a case of localized aggressive periodontitis associated with unusual gingival enlargement, which was later diagnosed as pyogenic granuloma and treated conventionally.9 Nitta et al described a case of a female patient with recurrent unusual gingival enlargement with rapidly progressive alveolar bone loss.10 Unusual gingival enlargement was considered owing to systemic factors that exaggerated the gingival response to local irritation and altered the usual clinical features of chronic gingivitis; local plaque irritation produced the extensive and recurrent enlargement of the gingiva.10
In the present case, the presence of inflammatory cells in the histologic examination confirmed that enlargement was inflammatory in nature. Presence of conditions such as gingival enlargement may complicate the diagnosis of generalized aggressive periodontitis; therefore, diagnosis should always be based on a detailed study of the patient's history and clinical, radiographic and microbiologic findings.9–10
Treatment included mechanical therapy with adjunctive antimicrobial therapy. Many studies have reported success in the treatment of aggressive periodontitis using antimicrobials as adjuncts to standard therapy.13 Adjunctive antimicrobial therapy has been recommended because aggressive periodontitis does not respond to conventional periodontal therapy alone and periodontal pathogens like Aggregatibacter actinomycetemcomitans and Porphyromonas gingivalis have the capacity to penetrate and remain in the tissues.14 These pathogens can also reinfect the pocket after the therapy, thereby leading to recurrence of the disease.14 Systemic antibiotics should only be administered as an adjunct to mechanical debridement because, in undisturbed subgingival plaque, the target organisms are effectively protected from the antibiotic agent due to the biofilm effect.15
The choice of antimicrobial therapy could be either empirical (based on either known common pathogens in the condition and their current resistance patterns) or directed (based on culture and susceptibility test results). Both approaches have been suggested but currently there is no direct evidence that microbiologic diagnosis and targeted selection of the antibiotic regimen provides an additional benefit compared to empiric use.15 Antibiotics prescribed for the treatment of aggressive periodontitis include doxycycline (tetracycline), amoxicillin with clavulanate potassium (Augmentin), metronidazole, clindamycin, ciprofloxacin, metronidazole, and azithromycin.16,17 Combinations of metronidazole-amoxicillin and metronidazole-ciprofloxacin-tetracycline have been reported to be successful in many cases. In the present case, doxycycline was selected because of the higher concentration of doxycycline in the gingival crevicular fluid and also as a result of its anti-collagenase activity.17 Successfully treated cases of generalized aggressive periodontitis may show subsequent signs of relapse. With this in mind, the patient was instructed to report every three months for oral hygiene reinforcement and scaling.
Conclusion
Presence of supernumerary teeth in aggressive periodontitis appears to be a coincidence.12 Presence of gingival enlargement in cases of aggressive periodontitis may complicate the diagnosis, which should be based on the study of a patient's history, clinical, radiographic and microbiologic findings.