Professor of Oral Surgery, King's College London; Honorary Consultant in Oral Surgery, King's College Hospital NHS Foundation Trust and Guy's and St Thomas' NHS Foundation Trust, London
A feared aspect of dental care for patients is their expectation of pain and injections. Local anaesthesia in dentistry is an important means of reducing procedural pain and increasing patient comfort during treatment. However, it can be a source of pain in itself. Fear of needles and painful injections is a significant contributing factor to dental anxiety and is a commonly reported concern among patients. This review aims to discuss modes by which the painless and effective injection can be achieved, exploring the causative factors of discomfort and how they can be modulated. Although a wide array of techniques and technologies exist within the field of local anaesthesia (which are outlined in this paper), there is no definitive method for delivering the perfect injection for each and every patient. By being more mindful of current research and understanding with regards to local anaesthesia, however, clinicians may become more confident in their ability to provide a more atraumatic experience.
CPD/Clinical Relevance: The aim of this review is to make clinicians aware of evidence-based suggestions for reducing the discomfort associated with delivering conventional local anaesthesia in routine dental practice, as well as to inform clinicians about alternative modes of administration of local anaesthesia which may serve as adjuncts in the management of anxious patients.
Article
Matin Ali Madadian
It is no secret that a visit to the dentist is perceived within society as being an unpleasant or daunting experience and dental phobia is somewhat commonplace. Pain, insufficient anaesthesia, the sensation of injections and seeing needles are among some of the most common anxiety-provoking stimuli and source of complaint in the dental setting,1 and are, in part, responsible for creating this negative image of the profession.
There is evidence to show that people with higher levels of anxiety are more likely to attend the dentist irregularly2 and also are more likely to have poorer oral health.3 One study showed that more than 1 in 4 adults had some fear of dental injections, with 5% of those surveyed admitting to avoiding treatment due to this.4 Furthermore, fear of injection poses a potential clinical hazard which is not often considered. A survey of medical emergencies in North America showed that more than half of emergencies which occurred within the dental setting were vasovagal syncope associated with the administration of local anaesthetic.5
Therefore, it is clear that there is an ethical and practical case for ensuring the provision of painless effective local anaesthesia: for the reduction of anxiety, improving patient comfort, improving rates of attendance and, ultimately, encouraging better oral health. Local anaesthesia in dentistry can, and should, be atraumatic and dental health professionals therefore owe this practice to their patients, where possible.6
This review aims to outline and discuss the causative factors inducing pain in the administration of local anaesthesia, current understandings on methods that exist to minimize pain, and the efficacy of new innovations in local anaesthesia in comparison to the conventional injection.
The role of psychological factors in local anaesthesia
The pain associated with delivering an injection is complex and multi-factorial (depending on the dentist, the patient and the equipment used), and is not only caused by the procedure itself, but begins with the anticipation of the event. Studies have shown a correlation between increased anxiety prior to procedures and reduced pain thresholds.7 In dentistry, patients with previous unpleasant experiences or those with dental anxiety have been shown to perceive more pain.8 A clinician may also inadvertently contribute to patient anxiety by using phrases like ‘this will hurt a bit’ or ‘this may feel uncomfortable’ prior to injections, or by displaying the needle/syringe within view. Another interesting factor has been found to be the appearance of the injector used. One study group of paediatric patients showed increased anxiety towards conventional metal syringes as opposed to alternatives (ie plastic, The WandÒ etc).9 It is therefore paramount for the attainment of a painless injection first to avoid inducing anxiety and to establish a calm environment for the patient.
Altering the psychological state and emotions have been known to play a role in reduced pain perception.10 Various methods have been trialled in an attempt to modulate attention, such as music-distraction or inducing a positive-emotional state by relaxation, and have been shown to have a considerable impact on dental anxiety.11 In a study of paediatric patients, active distractions by encouraging deep breathing and blowing out of air led to fewer signs of pain and these patients were more compliant in the delivery of the injection.12 Other means of anxiolysis, such as hypnosis, have been trialled, with reasonable success indicated in one study of 82 dental implant surgery patients showing a significant reduction in heart rate/blood pressure compared to the control.13 Similarly, the use of anxiolytic medications prior to procedures have also shown positive effects in the management of dentally anxious patients.14
Such methods, among others, may be routinely implemented into practice prior to procedures, where necessary, in order to facilitate treatment of patients with some degree of dental anxiety.
Preparing the surface mucosa for injection
A discomfort-inducing step in delivering local anaesthesia is the penetration of the needle through the most superficial tissues. One common way of tackling this is the use of topical anaesthesia in the form of a concentrated solution/gel/spray that may be applied to the mucosa, which acts by blocking noxious stimuli from peripheral sensory nerve endings from the most superficial intra-oral mucosa.15 A randomized controlled trial has proven the efficacy of topical agents compared to a placebo in the delivering of dental injections in some cases, such as for palatal infiltrations.16 A variety of different agents are available (for example lidocaine 5%, benzocaine 20%) and studies show a similar degree of clinical efficacy between various types of topically applied gel.17 Other delivery mechanisms, such as lidocaine patches, have been trialled as alternatives with similar effect,18 or in some studies have proven to be more effective than gel application in pain reduction for patients.19 The main limitation of the use of intra-oral patches as an alternative to topical gel, however, is the duration of application. This can be up to 15 minutes prior to delivery of the injection, but it could potentially be a viable/feasible option where gel is not tolerated by the patient and the use of some pre-procedural anaesthesia is indicated (ie in a paediatric patient who dislikes the taste or sensation of topical gel).
There is a good case for giving patients the option of pre-infiltration anaesthesia in some form prior to some dental injections, with positive results in pain reduction,20 but this may not just be as a direct result of its pharmacological activity on the tissues. In one study, subjects were given an intra-oral injection preceded by receiving either a placebo or some topical anaesthesia, where all were given topical anaesthesia. Those with the belief of receiving a placebo suffered from a significantly greater pre-procedural anxiety, indicating that the provision of topical anaesthesia also bears some psychological benefit for the patient.21
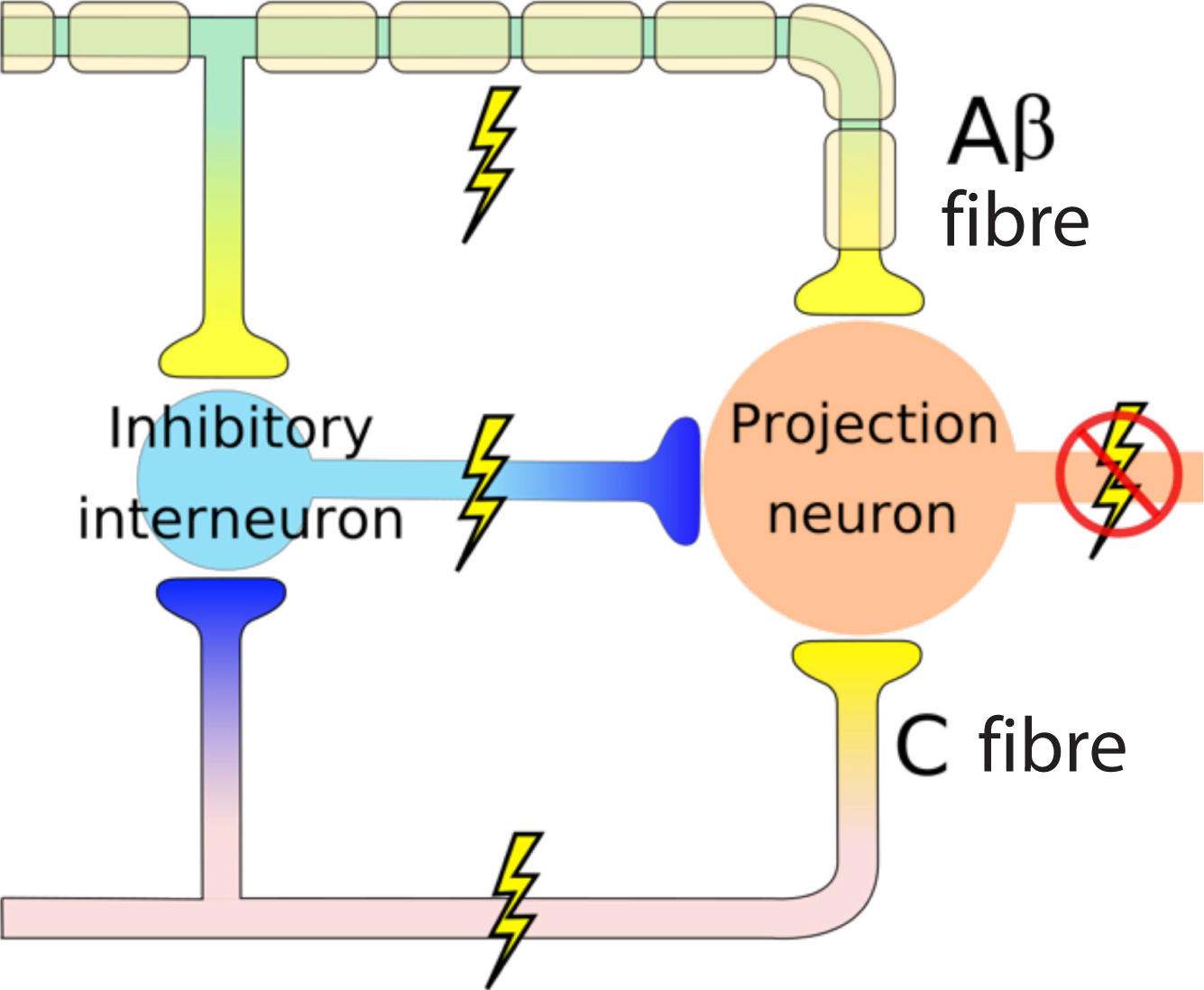
However, the use of topical anaesthesia has not been found to be a universal solution to reducing pain in all intra-oral injections, with no significant effect found in the administration of certain blocks, such as the long buccal and inferior alveolar nerve blocks (IANBs).22 This may be attributed to the nature of the inferior alveolar injection penetrating significantly deeper into the tissues than infiltration techniques, approximately 25 mm from the mucosal surface. Topical anaesthesia is of little value in this situation, with its effective absorption being mainly limited to the most superficial layer of tissue. In such circumstances, transcutaneous electronic nerve stimulation (TENS) has been put forward as a possible alternative with mixed results. The proposed mechanism of action is called the ‘gate control theory’ (Figure 1), first described in 1965, and suggests that stimulation of nerve fibres by an external stimulus (such as that electric current introduced by TENS) inhibits impulse transmission in Aβ and C fibres involved in pain reception at cell bodies in the dorsal horn, which, overall, reduces the perception of the noxious stimulus.23 Research has shown significant reduction in discomfort in delivering an IANB or palatal injection while using this technology,22 where topical anaesthesia showed no benefit, but there is also evidence to the contrary.16
Figure 1. Simplified diagram demonstrating the ‘gate control theory’: stimulation of Aβ fibres lead to stimulation of inhibitory neurones, which in turn inhibit the projection neurone from transmitting pain signals to the sensory cortex of the brain, limiting overall pain sensation.
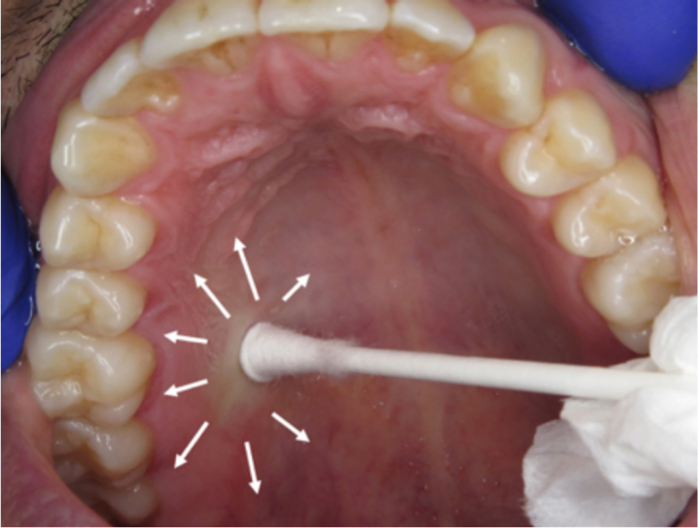
Other forms of sensory distraction have been explored, including pre-cooling the injection site with a cotton pellet sprayed with dichlorodifluoromethane for five seconds, which has been shown to mask the discomfort of injecting in the palatal area to some extent.9 Another widely used mode of sensory distraction, which can be easily implemented in clinical practice, is the gentle application of pressure adjacent to the injection site (ideally with a firm but dull object, such as a cotton tip (Figure 2)). This may be useful in reducing the pain associated with initial penetration, by the same inhibitory mechanism, and also may aid in stabilization of the needle over the injection site prior to penetration.6
Figure 2. Cotton tip applied to palatal mucosa – pressure should be sufficient to cause blanching (see image) of the soft tissue and should be maintained throughout the duration of the injection for best results. Some clinicians may prefer using other objects, such as dental mirror handles, however, it is advisable to be mindful of any sharp edges which may inadvertently damage the tissues or cause discomfort.
There are instances where all the above techniques have given negligible benefit to the patient in terms of pain sensation compared to a placebo. As such, different pharmacological pathways have been explored to modulate the pain response when all else fails: one well-documented in the literature is the use of inhalation sedation with NO2/O2, which has been proven to give significant reduction in discomfort on initial intra-oral injection. This requires comprehensive medical assessment of the patient and informed written consent prior to procedure and is therefore a technique that is reserved for when patient anxiety control necessitates it.24
The involvement of equipment in the painless injection
There are many variables at a clinician's disposal as far as equipment is concerned: different types of needle, syringe and anaesthetic cartridges, all of which have a bearing on the sensation of the injection.
Needle diameter is often believed to have an impact on painful delivery by clinicians and, despite potential increased breakage risk, higher gauge needles are favoured by many. However, one study showed no noticeable difference in pain reported among paediatric patients when using 25- or 30-gauge needles.25 One factor that does, however, have a bearing on pain is the condition of the needle. Electron microscopy has found visible deformity of needle tips upon first intra-oral injection compared to unused needles, which perhaps suggests that secondary injections using the same needle may lead to more pain than the use of a fresh needle for every mucosal penetration.26 In a study in which subjects were given two intra-oral injections, the first with a new needle and second either with a fresh needle or the one used for the initial injection (with both subject and operator blinded to this), there was a statistically significant discrepancy in discomfort noted.27
The second factor to consider is the content of the cartridge used, which includes, but is not limited to, type of anaesthetic solution used, the pH of the solution and the temperature of the solution.
Pre-warming local anaesthetic cartridges to body temperature (37°) in an attempt to minimize pain is often practised by clinicians. However, there is no conclusive evidence to show that there is any statistically significant difference between the sensation of room/body temperature solutions (21°/37°, respectively). Therefore, no justification has been found for incubating cartridges beyond room temperature, but it is most probably wise to allow refrigerated cartridges to warm to room temperature prior to use to prevent discomfort.28
Lower pH anaesthetic solutions have also been proven to increase discomfort on injection. Many anaesthetic formulations will now include buffering agents, such as sodium bicarbonate, in solution to increase the pH, which not only increases comfort of injection, but improves the rate of diffusion of the anaesthetic agent into cells.29
Operator-specific factors in pain reduction
The selection of a specific mode of anaesthesia is largely dependent on which teeth/tissues are to be anaesthetized and for what purpose (eg exodontia/restorative work) and is a decision ultimately made by the clinician. Certain intra-oral injections have been found to be more uncomfortable for patients than others, such as the IANB/palatal infiltration.30 Therefore, in order to achieve pain reduction, it is vital for the practitioner to select injections that could be more uncomfortable only where clinically necessary and most effective. For example, one study comparing the efficacy of a conventional IANB with lidocaine and a buccal infiltration using 4% articaine 1:100000 adrenaline in producing successful pulpal anaesthesia in mandibular first molars, not only showed similar efficacy between the two methods, but also faster onset of anaesthesia using the infiltration technique with articaine.31 In one review, Meechan discusses avoiding mandibular blocks and advocates the use of infiltration dentistry with articaine instead of anaesthesia for all teeth, from the mandibular first molars to the mandibular incisors, as being just as effective. In the anterior mandible, it was found that buccal infiltration was superior to the use of intraligamentary injections (which have not been found to be particularly effective as stand-alone injections) and IANBs (due to cross-over of nerve supplies from the contralateral inferior alveolar nerve in the anterior region).32
When considering this with a reduction in risk of iatrogenic local anaesthetic-related nerve damage by avoiding the unnecessary IANB, it can be said that the use of infiltration with articaine as an alternative is well-justified in many circumstances (eg for anaesthesia in the anterior mandible or for anaesthesia of single teeth).
Another approach first described by Meechan,33 known as the ‘chasing technique’, proposes an interesting way of tackling the uncomfortable palatal injection by means of a two-stage injection technique (Figure 3). Following administration of an initial buccal infiltration, a secondary injection through the interdental papilla is given following the onset of anaesthesia after the initial infiltration. In theory, some of the anaesthetic solution deposited interdentally should diffuse palatally, leading to the partial anaesthesia of the palatal gingivae, which can then be infiltrated with more ease/comfort. This technique is reported to have been employed in practice by clinicians in situations where discomfort of palatal injections is a primary concern, such as within paediatric dentistry.34 However, there have not yet been any clinical trials to evaluate its efficacy objectively, therefore this remains an interesting point of exploration.
Figure 3. Atraumatic techniques for delivering palatal anaesthesia. (a) Topical anaesthesia applied to mucosa with cotton tip. (b) Initial labial infiltration injection followed by (c) intrapapillary injection between the central incisors and, finally, (d) an injection to anaesthetize the nasopalatine area.
Some controlled variables in delivering an injection are down to technique and the way in which a clinician operates. Once the needle has penetrated the mucosa, the main sensation of discomfort felt by the patient is due to deposition of the solution. There is a large body of evidence to suggest that the deposition of solution over a longer period of time contributes to preventing discomfort, and patients tend to show fewer signs of pain. This has been replicated in studies using various block and infiltration techniques intra-orally,35,36 and there is also some data to suggest greater success in achieving pulpal anaesthesia when decreasing the anaesthetic flow-rate.37
Speed of injection and its effect on discomfort
The time taken to inject a full cartridge and the duration of application of a topical agent can have an impact on painlessness and recommended timings vary among operators. Malamed6 is well cited in the literature in the field of local anaesthesia and personally advocates allowing at least 60 seconds for the action of topical anaesthesia for adults (to allow ample time for diffusion of the anaesthetic agent into the superficial tissues prior to penetration) and an additional 60s to deliver a 1.8 ml cartridge, which not only increases the comfort of the injection, but reduces the risk of depositing fluid intravascularly as it allows the operator to aspirate while injecting continuously. Despite this, a large number of practitioners fail to adhere to such guidelines: one large survey of members of the American Academy of Pediatric Dentistry found 89% injecting a cartridge in less than a minute, and only a third applying topical anaesthesia for at least a minute prior to injection.38 There is no definitive timing advocated for use by all clinicians, however, many tend to err towards the side of quicker injections, perhaps due to time constraints in practice. However, the effectiveness of the injection must also be taken into consideration, not just the painlessness. One randomized study found the mean onset of pulpal anaesthesia in first molars in subjects delivered an IANB to be 8 minutes, with most teeth reaching maximum anaesthesia on electric pulp testing up to 30 minutes after delivery of the injection.39 Patience in delivery of injections and prior to beginning operative procedures can therefore be the difference between painless and effective anaesthesia and patient discomfort and lack of compliance.
Newer alternatives to the conventional syringe
One solution devised in recent years (first developed in the 1990s) with regards to speed of injection is the advent of ‘Computer Controlled Local Anesthesia Delivery System Devices’ (CCLADs) for the more controlled delivery of local anaesthesia in dentistry. The Wand/CompuDentTM, SmartjectTM and AnaejectTM systems are among some examples of such devices that offer an alternative to the conventional syringe.
Such devices not only offer ease and accuracy of needle placement intra-orally, due to a design that demands a pen-grip in its application (Figure 4), but also computer control of injection speed and pressure, to maintain a precise flow-rate depending on the resilience of the tissues penetrated (which is of great significance in the palatal and intraligamental tissues). This is then sensed by the device and injection pressure is adjusted accordingly.40 CCLADs in general are still the subject of many clinical trials evaluating their efficacy in comparison to conventional methods. However, a literature review assessing some of the available devices on the market concluded that there is a statistically significant reduction in pain and greater efficacy in adult subjects in general. Nevertheless, further studies are required to reach a definitive stance on their efficacy.41 Despite the significance of this finding, the effect of using such systems may be considered negligible in the face of other factors. A randomized controlled trial conducted on paediatric patients compared pain responses in children of different levels of dental anxiety using the Wand® or traditional injection. The trial failed to find a clear difference in behaviour in children, especially among the highly dentally anxious, leading to the conclusion that it is perhaps more relevant to consider dealing with the fear/anticipation of pain on injection in these cases rather than trying to modulate the pain itself, which may not actually be substantial in comparison.42
Figure 4. Image demonstrating pen-grip when using The WandÒ syringe (left) and processor unit controlling rate of flow of anaesthetic solution (right). Clinicians may prefer the tactile control over this syringe owing to its design, facilitating placement intra-orally. The design itself may also be less anxiety-provoking than a conventional syringe, which may be worth considering when managing the anxious patient.
One alternative technology proposed is the use of vibration in pain reduction, which again is theorized to work by the mechanism explained by the ‘gate control theory’.23 VibraJect® is an attachment that has been designed specifically to be fitted onto a conventional dental syringe (Figure 5), producing high frequency vibrations in the needle tip, intending to reduce pain and possibly negating the need for topical anaesthetic. Blinded studies comparing the VibraJect® system to the conventional approach failed to show any benefit.43 It is worth noting, however, that this technology has not been extensively studied by any means, and there simply isn't enough literature on the topic to draw any definitive conclusions. Secondly, it is difficult to blind subjects to the use of vibration, even with the use of headphones and eye-masks, and patients not made aware of the nature of the vibrating injection may tend to over-report pain or discomfort due to an unexpected/unconventional sensation that VibraJect® may provide.
Figure 5. A conventional syringe with VibraJect® attachment.
Conclusion
There is no hard-and-fast rule to delivering the painless injection; evidence shows outliers and exceptions when using every technique and each patient is different. This does not mean, however, that the attainment of painless local anaesthesia is impossible. With appropriate initial assessment of patients and their preferences, awareness of current knowledge/research with regards to pain reduction, an appreciation of the importance of psychological factors in pain perception, and a flexible delivery technique catering to each individual, one can be confident in making the procedure as streamlined and pain-free as possible.