Kielbassa AM, Hinkelbein W, Hellwig E, Meyer-Lϋckel H. Radiation-related damage to dentition. Lancet Oncol. 2006; 7:326-335
Epstein JB, Emerton S, Kolbinson DA Quality of life and oral function following radiotherapy for head and neck cancer. Head Neck. 1999; 21:1-11
Henriksson R, Fröjd O, Gustafsson H Increase in mast cells and hyaluronic acid correlates to radiation-induced damage and loss of serous acinar cells in salivary glands: the parotid and submandibular glands differ in radiation sensitivity. Br J Cancer. 1994; 69:320-326
Duncan GG, Epstein JB, Tu D, Pater mJL. Quality of life, mucositis, and xerostomia from radiotherapy for head and neck cancers: a report from the NCIC CTG HN2 randomized trial of an antimicrobial lozenge to prevent mucositis. Head Neck. 2005; 27:421-428
Henson BS, Inglehart MR, Eisbruch A, Ship JA. Preserved salivary output and xerostomia-related quality of life in head and neck cancer patients receiving parotid-sparing radiotherapy. Oral Oncol. 2001; 37:84-93
Lin A, Kim HM, Terrell JE, Dawson LA, Ship JA, Eisbruch A. Quality of life after parotid-sparing IMRT for head-and-neck cancer: a prospective longitudinal study. Int J Radiat Oncol Biol Phys. 2003; 57:61-70
Aguiar GP, Jham BC, Magalhaes CS, Sensi LG, Freire AR. A review of the biological and clinical aspects of radiation caries. J Contemp Dent Pract. 2009; 10:83-89
Epstein JB, McBride BC, Stevenson-Moore P, Merliees H, Spinelli J. The efficacy of chlorhexidine gel in reduction of Streptococcus mutans and Lactobacillus species in patients treated with radiation therapy. Oral Surg Oral Med Oral Pathol. 1991; 71:172-178
Epstein JB, Loh R, Stevenson-Moore P, McBride BC, Spinelli J. Chlorhexidine rinse in prevention of dental caries in patients following radiation therapy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1989; 68:401-405
Eliasson L, Carlén A, Almståhl A, Wikström M, Lingström P. Dental plaque pH and micro-organisms during hyposalivation. J Dent Res. 2006; 85:334-338
Llena-Puy C. The role of saliva in maintaining oral health and as an aid to diagnosis. Med Oral Patol Oral Cir Bucal. 2006; 11:E449-455
Han P, Suarez-Durall P, Mulligan R. Dry mouth: a critical topic for older adult patients. J Prosthodont Res. 2015; 59:6-19
Saleh J, Figueiredo MA, Cherubini K, Salum FG. Salivary hypofunction: an update on aetiology, diagnosis and therapeutics. Arch Oral Biol. 2015; 60:242-255
McCaul LK. Oral and dental management for head and neck cancer patients treated by chemotherapy and radiotherapy. Dent Update. 2012; 39:135-140
Powell LV, Persson RE, Kiyak HA Effect of a 0.12% chlorhexidine rinse on salivary lactobacilli and mutans streptococci. J Dent Res. 2001; 80
Epstein JB, van der Meij EH, Lunn R, Stevenson-Moore P. Effects of compliance with fluoride gel application on caries and caries risk in patients after radiation therapy for head and neck cancer. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996; 82:268-275
Cochrane NJ, Cai F, Huq NL, Burrow MF, Reynolds EC. New approaches to enhanced remineralization of tooth enamel. J Dent Res. 2010; 89:1187-1197
Worthington HV, Clarkson JE, Eden OB. Interventions for preventing oral mucositis for patients with cancer receiving treatment. Cochrane Database Syst Rev. 2006;
Barber AJ, Butterworth CJ, Rogers SN. Systematic review of primary osseointegrated dental implants in head and neck oncology. Br J Oral Maxillofac Surg. 2011; 49:29-36
Schiegnitz E, Al-Nawas B, Kämmerer PW, Grötz KA. Oral rehabilitation with dental implants in irradiated patients: a meta-analysis on implant survival. Clin Oral Investig. 2014; 18:687-698
Salivary gland damage is the most common adverse effect associated with radiation therapy to the head and neck. A combination of hyposalivation and dietary changes, with a reduced emphasis on oral hygiene practices can contribute to a massive increase in a person's caries risk status. This can be further complicated by limited mouth opening. To enable optimal dental care for head and neck cancer patients before, during and after radiation therapy, patients must be informed and educated about the potential risks of dental caries and the preventive strategies available. All patients should receive a pre-radiotherapy dental assessment by a Restorative Dentistry Consultant. This information will be delivered to the patient, often at an emotionally charged time, and can be lost amongst all the information related to other aspects of his/her cancer management. General Dental Practitioners (GDPs) are therefore in a pivotal position to reiterate this information post radiation therapy and ensure compliance with preventive strategies, with the overall aim to improve quality of life and avoid the need for future extractions and the resulting risk of osteoradionecrosis.
CPD/Clinical Relevance: This article highlights the GDP's role in the shared management of head and neck cancer patients who have received radiotherapy as part of their cancer treatment. The critical issue of dental caries, one of the late effects of radiation-induced hyposalivation, will be focused upon. Other side-effects, such as trismus and osteoradionecrosis, will also be discussed. This article aims to supply GDPs with accurate information to provide to their patients with post radiation therapy, whilst highlighting what treatment is within their remit and when it may be appropriate to refer.
Article
Salivary gland damage is the most common adverse effect associated with radiation therapy to the head and neck.1 Salivary flow decreases rapidly during the first week of treatment, followed by fibrosis of the glands and permanent loss of secretory capacity. This can result in a dramatically diminished quality of life.1,2 The discomfort of reduced salivary flow is compounded by severe inflammation and ulceration of the oral mucosa cavity, a condition called mucositis (Figure 1). This usually begins after the first two weeks of radiotherapy, and improves after a few weeks following completion of treatment.
Figure 1. Mucositis.
The degree of salivary gland damage is dependent on the volume of tissue irradiated and the total dose administered, and results in both a quantitative and qualitative effect on saliva production. Doses above 20 Grays (Gy) are associated with the loss of up to 90% of salivary acinar cells3 and head and neck cancer (HNC) patients usually receive doses as high as 70 Grays.
The symptom of xerostomia can be debilitating, resulting in patient discomfort and a decreased quality of life.4,5,6 It can lead to pain, an increase in oral infections and functional limitations impacting on a person's voice, taste, swallowing or sleep. Hyposalivation is the term to describe an actual decrease in the measured salivary flow and this is a major risk factor for the development of caries.
Other significant problems include a limitation of mouth opening and increased risk of osteoradionecrosis (ORN). ORN is described as hypovascularity and necrosis of bone followed by either trauma-induced or spontaneous mucosal breakdown, leading to a non-healing wound.
Radiation caries
Radiation-induced caries describes the rapidly developing lesions that can appear after radiotherapy. Its distribution tends to be different from those carious lesions in the non-irradiated population, appearing on incisal edges, cusp tips and smooth surfaces (Figure 2).7 It is often circumferential along the cemento-enamel junction and gingival margins, which can lead to decoronation if the tooth becomes sufficiently unsupported.
Figure 2. ‘Radiation caries’.
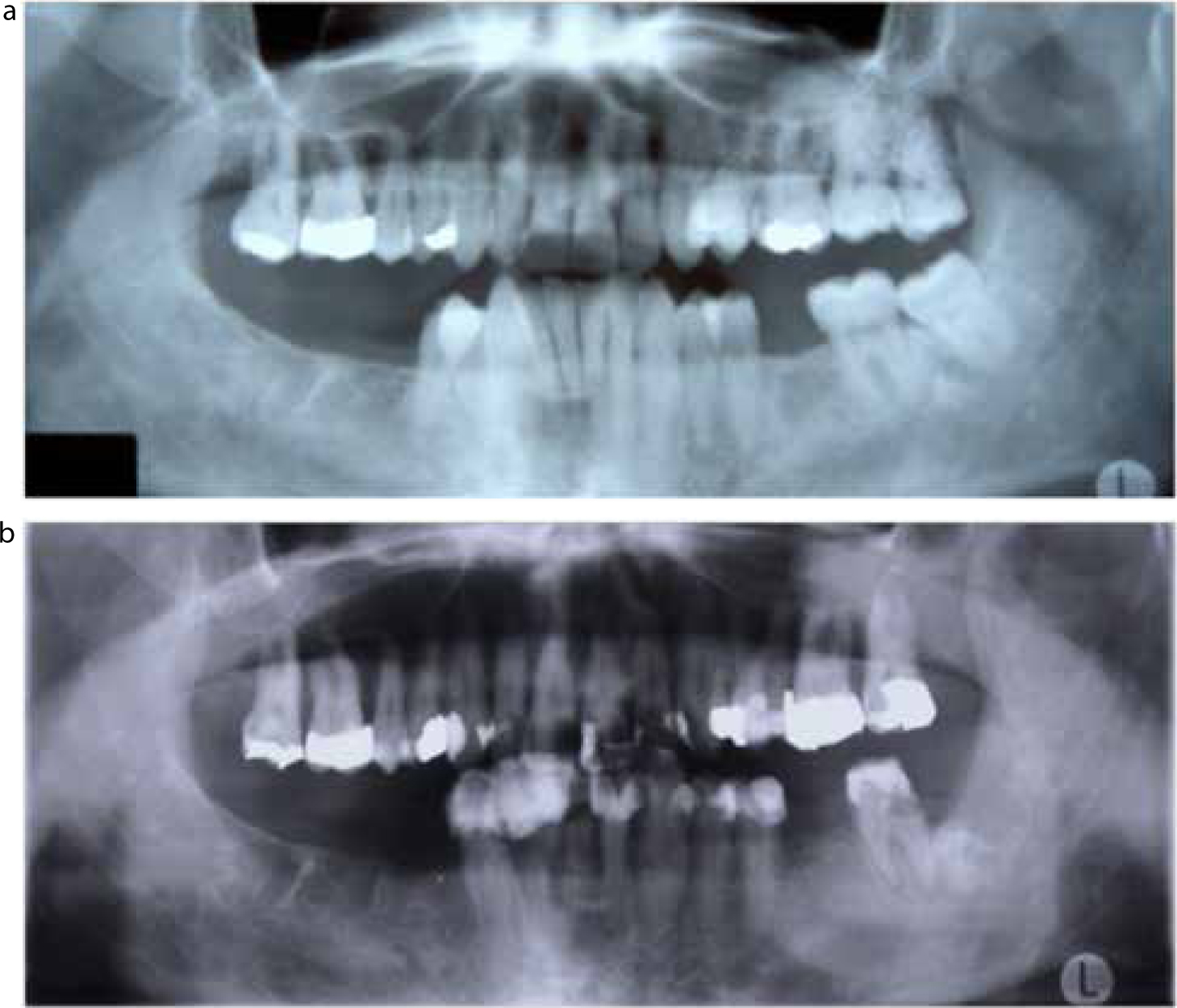
A direct histological effect of radiotherapy on tooth structure has been shown, however, this is believed to be insignificant when compared to the negative indirect effects of radiotherapy; related to reduced saliva flow and its reduced buffering capacity, coupled with dietary changes often with frequent high sugar supplements, a difficulty with oral hygiene and changes in the oral microflora that also occur.1 This highlights why all teeth in the mouth are at risk of radiation caries, it is not limited to teeth within the primary beam of radiation (Figure 3).
Figure 3.
(a, b) Deterioration of the mouth over 6 months through radiation caries.
Risk factors
The following features which contribute to an increased caries risk status will be discussed along with any specific recommendations:
Hyposalivation;
Xerostomia;
Changes in nutritional needs;
Trismus.
Hyposalivation
The reduced quantity of saliva is thicker in nature with changes in its antibacterial properties and ionic concentrations. This results in a shift in the colony counts of micro-organisms with an increase in cariogenic bacteria such as Streptococcus mutans and Lactobacillus species,8,9 a reduced buffering capacity1,10,11 and an average post-irradiation pH of 5.0.9 These act to tip the caries balance in favour of demineralization.
Advice
Referral to Oral Medicine to assess whether stimulation of residual salivary secretion is possible with sialagogues such as pilocarpine, cevimeline and bethanechol;12,13
Use of an appropriate saliva substitute (gel/rinse/spray) depending on whether the patient is dentate or edentulous;
Meticulous oral hygiene practices including use of interdental brushes daily;
Increased fluoride, calcium and phosphate exposure;
Chlorhexidine mouthwash twice daily used at separate time to fluoride use.
Xerostomia
The symptom of a dry mouth may lead to frequent sipping on liquids.
Advice
Maintain hydration by sipping on water only, avoidance of moistening the mucosa frequently with sugary or acidic drinks;
Use of an appropriate saliva substitute (gel/rinse/spray) depending on whether the patient is dentate or edentulous;
Sugar-free chewing gum.
Changes in nutritional needs
Diet changes contribute to risk of dental caries formation in an HNC population. During treatment, if weight loss is an issue, HNC patients are often advised to eat frequent small meals with emphasis on high calorie foods. The frequency of meals may make it difficult to brush between feedings. In addition, patients often use liquid supplements containing refined carbohydrates which favour adhesion to dental surfaces and predispose to caries.14
Advice
Accept a highly cariogenic diet but ideally only in the immediate short term;
Meticulous oral hygiene practices including use of interdental brushes daily;
Increased fluoride, calcium and phosphate exposure;
Stop sugar in tea/coffee and replace all sugar with artificial sweeteners where possible.
Trismus
Limitation of mouth opening following cancer therapy may be caused by surgically- or radiotherapy-induced fibrosis of the masticatory muscles. This can limit access for daily oral hygiene practices, non-surgical periodontal therapy and tooth restoration.
Advice
Take a measurement of the inter-incisal mouth opening as a baseline;
Jaw opening exercises, eg with increased thickness of tongue depressors or a therabite device in a ‘777 regimen’ – 7 stretches for 7 seconds, 7 times a day (Figure 4).
Figure 4. Jaw opening exercise.
Preventive strategies
Regular dental recall
Required to monitor the dentition closely, along with checking for any signs of cancer recurrence.
Patients have a high risk of oral disease and should be seen on a three monthly basis until they show long term signs of stability, at which point a six monthly review may be appropriate. Routine care should include regular dental checks, routine dental treatment and supportive periodontal therapy. Six to twelve monthly bitewing/periapical radiographs are advised long term.
Optimizing oral hygiene
This should be tailored to the individual patient's dexterity and motivation, utilizing other members of the dental team to provide care, motivation and support. There should be twice daily effective toothbrushing and use of interdental brushes daily.
Chlorhexidine
Chlorhexidine has been shown to reduce colonization of cariogenic flora in HNC patients. The number of Mutans streptococci can be reduced to below a pathological level for 12–36 weeks.15 Unfortunately, the effect is not sustained within HNC patients, and a more rapid recovery in cariogenic bacterial counts is seen. Until further research demonstrates an effective regimen of chlorhexidine use in HNC, rinsing with 0.12% chlorhexidine for one minute, twice daily for two weeks followed by twice weekly thereafter (rinsing no less than 30 minutes after fluoride use) may be considered as an adjunct in a patient exhibiting radiation caries.
Fluoride
Data clearly support the use of fluoride to enhance remineralization, thus the use of fluoride has become a mainstay of preventive dental care in the HNC population.16 Both the frequency of exposure and concentration of fluoride is crucial. Brushing with Duraphat 5000 ppm (Colgate) twice daily should be a minimum. In addition, a pea-sized amount can be used in upper and lower soft splints for 30 minutes daily (Figure 5). A supplemental 0.05% sodium fluoride (alcohol free) rinse can be used daily, held in the mouth for one minute at a separate time to brushing, when the trays are not used.
Figure 5. Fluoride trays.
Calcium and phosphate
Unfortunately, the efficacy of fluoride may be limited in the HNC population due to the lack of calcium and phosphate secondary to hyposalivation.17 Remineralization cannot occur if the degree of saturation of calcium and phosphate in saliva related to tooth mineral is low. Although data are sparse, they appear to support the potential and promising results of calcium and phosphate in addition to fluoride, on the remineralization of early dental caries in HNC patients. The recommended regimen is to apply a product such as Tooth Mousse (GC, UK, Newport Pagnell) with a finger around the teeth, leave for 5 minutes then spit out any excess, prior to the use of fluoride within soft splints for 30 minutes daily as above.
Saliva substitutes
This may include patients trying several different brands and forms of delivery (sprays, gels, rinses). Care must be taken to advise sugar-free, pH neutral or alkaline products to dentate patients (Table 1), and animal-derived products when appropriate.
When caries is detected, consider the following points:
Whether a cleansable lesion be created to aid remineralization;
The caries should be addressed without delay to avoid the need for extraction;
Maximum preservation of underlying tooth structure;
A hygienic design of any restoration.
Treatment options
The treatment options are more limited in HNC patients. They must be selected, fulfilling the aims of caries management (Table 2). These treatment options encompass the following:
Intensive prevention alone: ensure cavities are cleansable;
Direct restorations;
Indirect restorations are best avoided unless compliance with preventive advice is optimal;
Removable partial dentures are not advised unless essential for aesthetics or function. Hygienic, tooth-supported designs where possible;
Root canal treatment +/- overdenture to avoid extraction;
Where root canal treatment is not possible, extraction, accepting the risk of osteoradionecrosis (ORN) (Figure 6).
To maximize quality of life following treatment
Encourage lifelong commitment to preventive strategies
Prompt stabilization of any carious lesions
Reduce the risk of ORN by avoiding extraction
Root canal treatment +/- overdenture to avoid extractions
Well-fitting, hygienic removable prostheses when appropriate
Figure 6. Osteoradionecrosis following extraction of LR7 following radiotherapy.
Discussion
GDPs have a vital role to play in promoting the lifelong oral health of their patients. The burden is even higher when their patients' disease risk status is increased, such as that seen in patients who have received radiotherapy for head and neck cancer, with resulting hyposalivation. GDPs are in the ideal position to continue reinforcing the importance of preventive dentistry in this complex cohort who have lost a major protective factor against caries. Regular recall will ensure regular soft tissue checks for recurrence, and any caries can be detected early. In this group of patients, the dentistry is simple and based on preventing or arresting caries as and when necessary, and producing hygienic, well-sealed restorations to prevent pulpal complications.
It is unlikely that the GDPs will see their patients during radiotherapy when they may be suffering the short-term side-effects of treatment, such as mucositis and infection. However, short-term relief of mucositis has been obtained through Chinese medicines, hydrolytic enzymes, ice chips, benzydamine, calcium phosphate, etoposide bolus, manuka honey, iseganan and zinc sulphate.18 All have been shown to demonstrate some level of benefit, although the response seems to be patient specific. Interestingly, nystatin does not appear to be effective for oral candida infections caused by cancer treatment. However, CHX may be of benefit due to its antifungal, antibacterial and antiplaque effects, but its value is still unconfirmed.
The role of preventive dentistry cannot be emphasized enough. If limited access makes operative dentistry impossible then the jaw opening advice as above should be given with an urgent referral to a local Restorative Dentist and all preventive strategies employed to minimize the rate of deterioration. When an extraction is unavoidable, if the root(s) cannot be root-filled and retained, then extraction should be carried out by an Oral Surgeon or Oral and Maxillofacial Surgeon in a secondary care setting so that extra precautions can be taken. This may include the use of hyperbaric oxygen therapy, before and after extraction to try and prevent ORN.
Treatment should be based around preventing the need for future dental extractions to avoid complications in balance with maintaining the dentition long term with regards to satisfactory speech, function and quality of life. If surgical resection for head and neck cancer has compromised satisfactory speech and function, osseointegrated implants can be considered to allow effective oral rehabilitation through support of oral or facial prostheses.19,20