Bartlett D, Ganss C, Lussi A. Basic Erosive Wear Examination (BEWE): a new scoring system for scientific and clinical needs. Clin Oral Investig. 2008; 12 Suppl 1:S65-68 https://doi.org/10.1007/s00784-007-0181-5
Loomans B, Opdam N, Attin T Severe tooth wear: European consensus statement on management guidelines. J Adhes Dent. 2017; 19:111-119 https://doi.org/10.3290/j.jad.a38102
Gulamali AB, Hemmings KW, Tredwin CJ, Petrie A. Survival analysis of composite Dahl restorations provided to manage localised anterior tooth wear (ten year follow-up). Br Dent J. 2011; 211 https://doi.org/10.1038/sj.bdj.2011.683
Burke FJ. Information for patients undergoing treatment for toothwear with resin composite restorations placed at an increased occlusal vertical dimension. Dent Update. 2014; 41:28-38 https://doi.org/10.12968/denu.2014.41.1.28
Vailati F, Belser UC. Classification and treatment of the anterior maxillary dentition affected by dental erosion: the ACE classification. Int J Periodontics Restorative Dent. 2010; 30:559-571
Hamburger JT, Opdam NJ, Bronkhorst EM Clinical performance of direct composite restorations for treatment of severe tooth wear. J Adhes Dent. 2011; 13:585-593 https://doi.org/10.3290/j.jad.a22094
Chu FC, Siu AS, Newsome PR Restorative management of the worn dentition: 4. Generalized toothwear. Dent Update. 2002; 29:318-324 https://doi.org/10.12968/denu.2002.29.7.318
Minimally invasive management of erosive tooth surface loss using a combined direct and indirect approach: a case report Salman Pirmohamed Dental Update 2024 48:7, 707-709.
Authors
SalmanPirmohamed
BDS (Hons), MJDF RCS (Eng)
Specialty Trainee in Prosthodontics, Eastman Dental Hospital and Institute, Field End Dental Practice, Pinner
This article describes the management of a patient with generalized (primarily erosive) tooth surface loss. It specifically looks at minimally invasive techniques using improvements in material science to achieve this in an efficient and predictable manner within a general dental practice setting.
CPD/Clinical Relevance: The use of minimally invasive techniques within a general dental practice setting are highlighted.
Article
With an increasingly elderly population who are retaining teeth for longer, the prevalence of tooth surface loss is on the increase. The most recent Adult Dental Health Survey (2009) revealed that 77% of dentate adults exhibited wear into dentine.1 Tooth surface loss can be attributed to either erosion, attrition or abrasion. However, it is commonly multifactorial in aetiology.2
Preventive management of tooth surface loss is the cornerstone of care for these patients, and screening tools such as the Basic Erosive Wear Examination (BEWE) should be employed at recall examinations for all patients.3 Tooth surface loss can be classified as being physiological or pathological. However, both groups may need restorative management in cases of:4
Compromised aesthetics;
Increased sensitivity of teeth;
Functional problems.
The traditional restorative management of tooth surface loss involved full mouth reconstructions using indirect restorations, which often resulted in a high treatment burden to teeth, and accelerated their path along the restorative cycle.2 This report presents a case that demonstrates the management of generalized tooth surface loss using a combination of direct and indirect composite restorations, with almost no tooth removal required.
Case report
History and examination
A 37-year-old gentleman presented to the practice in 2018 as a new patient with both aesthetic and functional concerns. He was experiencing generalized sensitivity to cold drinks and was unhappy with the appearance of his ‘chipped’ and ‘worn’ front teeth. The patient had realistic aesthetic expectations of mainly wanting more teeth to show when smiling. Medically, he was fit and well, but reported consumption of more than 1 litre of diet coke every day for the previous 5 years, along with a moderate sugar intake. A diet sheet later confirmed that the patient was consuming five cans of diet coke throughout the day. The patient reported no history of bruxism or other parafunction and had no obvious markers for this.
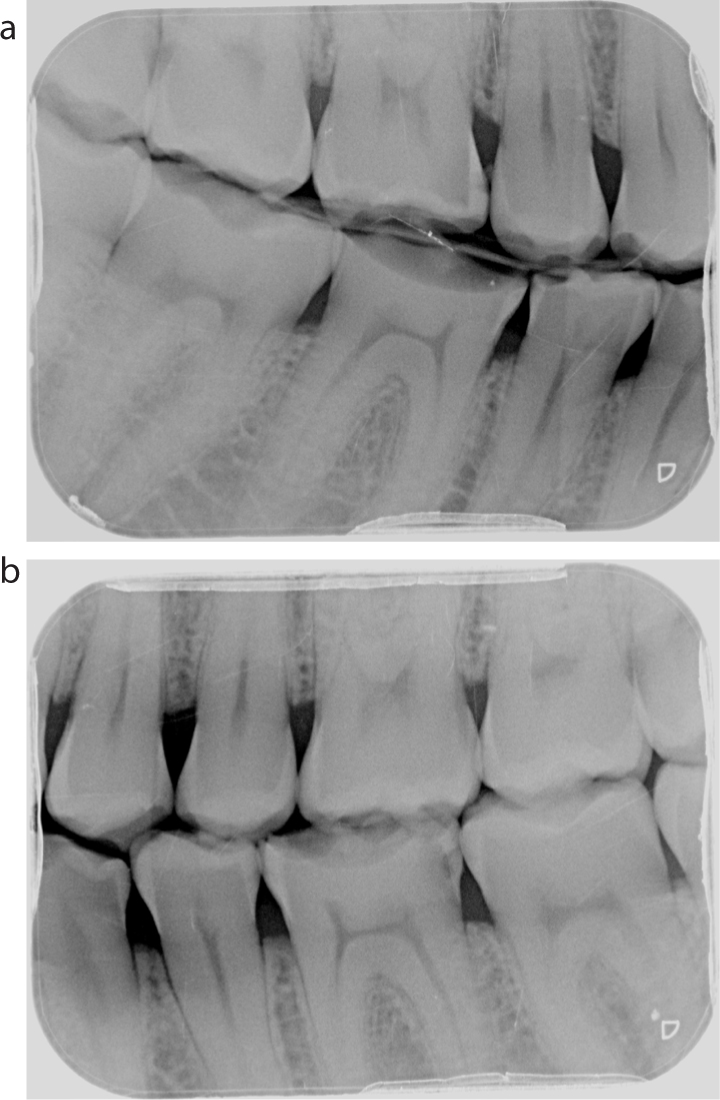
Examination revealed a fair level of oral hygiene, but marked evidence of tooth surface loss with dentine exposure on all teeth except the lower incisors. Several areas of shadowing, indicating caries, were noted, and confirmed by radiographs (Figures 1 and 2). Tables 1 and 2 present the BPE and BEWE scores, respectively.
Pre-operative aesthetic evaluation noted a cant going up to the right-hand side in the upper arch. The incisal edges were chipped, with no incisal show at rest. No obvious dento-alveolar compensation had occurred, but a slight reduction in the lower facial third was noted.
After a thorough history, examination, and special investigations the following diagnoses were reached:
Generalized moderate tooth surface loss with a primarily erosive component.
Prevention
Periodontal management involved tailored oral hygiene instructions and debridement. Dietary advice was given, and resulted in the patient completely cutting out carbonated drinks from his diet. The patient had been unaware of the dental implications of diet cola and had assumed this was better than normal cola for his teeth. This highlights the importance of patient education in managing tooth surface loss. Fluoride supplementation by a high fluoride toothpaste (Duraphat 5000ppm, Colgate, UK) was to be used twice daily, along with a daily fluoride mouth rinse (FluoriGard Daily Rinse 225ppm, Colgate, UK) to reduce the patient's caries and tooth surface loss risk. The patient showed excellent motivation in adhering to the preventive advice given.
Treatment options
After adherence to preventive advice was confirmed, a long discussion was held with the patient on options for further treatment.
A reorganizational approach was chosen because of the generalized tooth surface loss affecting almost all the teeth, and a lack of interocclusal space to restore the teeth. A variety of material options was discussed with the patient, but he had a strong preference for all the restorations to be tooth coloured, including those on the posterior teeth.
As the tooth surface loss was primarily erosive in nature and the causative factor had been stopped, composite was chosen to restore the anterior teeth. This was seen as a good balance between an aesthetic and a minimally invasive approach, and there is a strong evidence base supporting its use as a medium-term solution.5,6 Metal backings, for which there is also a strong evidence base that supports their use, may be an option for less aesthetically concerned patients.7 A ‘sandwich’ approach of indirect palatal composite backings and direct labial composite veneers was chosen for the upper anterior teeth. Indirect palatal backings were selected to allow better management of occlusion, and greater strength in this area to preserve planned anterior guidance in a mutually protected occlusal scheme. Furthermore, direct palatal composite build-ups can be challenging to carry out and the indirect backings also allowed for a ‘matrix’ against which the labial composite could be placed. The patient was made aware of the longevity of direct composites in these areas, and the need for repairs and replacement with time. Superior aesthetics could have been achieved with the use of porcelain veneers as shown by Vailati et al by the sandwich technique, but the patient and dentist preferred a non-invasive solution.8
The use of posterior direct composites in managing tooth surface loss is under debate because of the greater occlusal forces in these areas, although there is some promising evidence showing good success with newer hybrid composites.9 The presence of a good enamel rim on the posterior teeth for bonding, as well as supragingival margins for isolation, were deemed positive factors supporting its use in this case. Furthermore, financial constraints made this a more viable option for the patient, especially because of the number of teeth that required treatment. The patient was made aware of the possibility that these would need to be changed to indirect restorations with time (eg ceramic or gold).
Once posterior composites had been chosen for the tooth surface loss, it was decided to manage the carious lesions concurrently. This had the advantage of the composite being used in a single visit, which meant that old composite was not being bonded to and there was an overall reduced chairtime for the patient.
Planning phase
The preliminary planning involved making upper and lower impressions in alginate for study casts. A retruded axis position (RAP) record was then taken at an occluso-vertical dimension (OVD) that would allow for an adequate thickness of restorative material posteriorly. Ensuring to take the RAP record at the desired OVD is important because it limits the number of inaccuracies created in opening and closing the pin on the articulator.
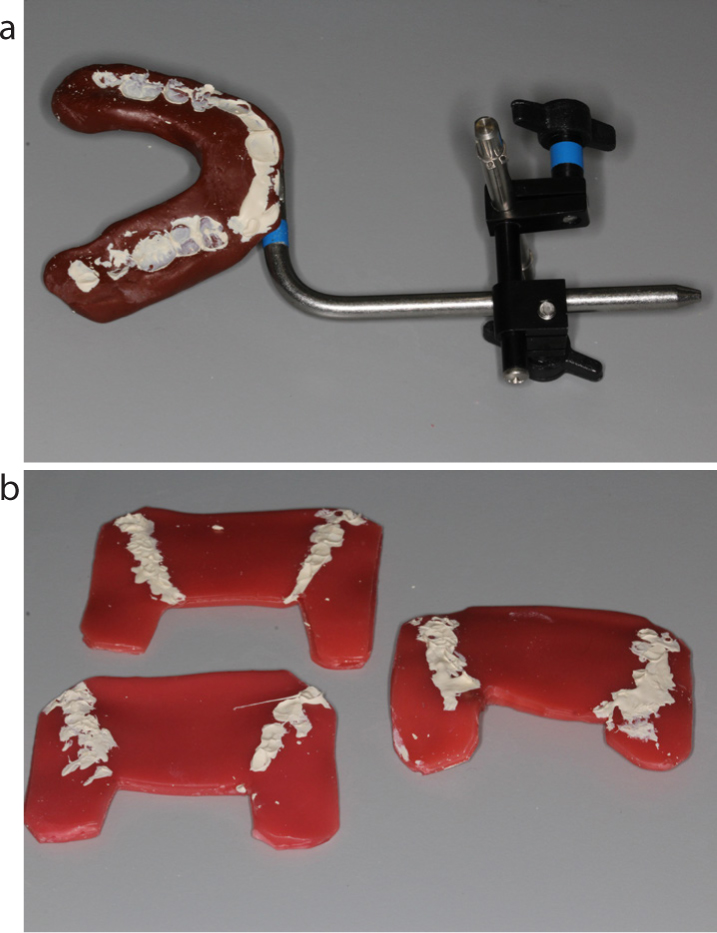
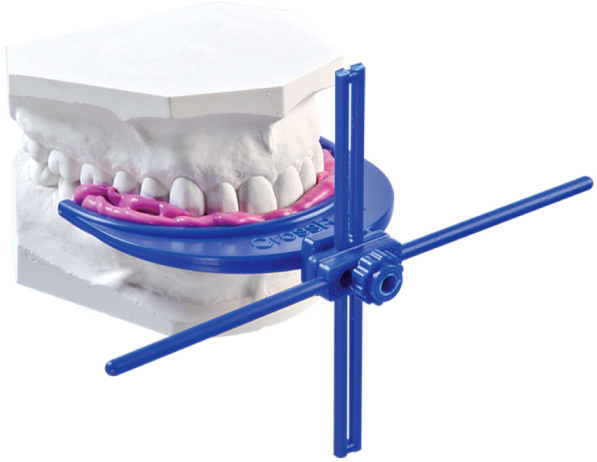
The facebow record taken was helpful in guiding the technician in addressing the canted smile line (Figure 3). However, if there had been facial asymmetry with ear positions, it should be noted other techniques would have had to be used. For example, the Whipmix Esthetic CrossRef allows accurate transfer of midline and horizontal planes to the articulated study casts (Figure 4).
Figure 3. (a, b) Facebow and occlusal records.Figure 4. Whipmix Esthetic CrossRef.
The above records were sent to the laboratory and a wax-up of the upper anteriors at ideal proportions was requested at the desired OVD. The palatal wax-up was planned to allow for vertical stops to ensure that forces would be direct through the long axis of the upper anteriors. An increase in incisal length of 2 mm was also requested to improve the incisal show for the patient, because this was one of his main concerns.10
Once the wax-up was received, a mock-up was completed using bisacryl resin (Protemp, 3M, USA) and a putty matrix (Figure 5). Aesthetics and occlusion were verified at this stage with the patient, and he consented to proceed with the restorative phase of treatment. The working impressions were taken in polyvinylsiloxane for construction of the upper indirect palatal composite backings.
Figure 5. Mock try-in.
Treatment phase
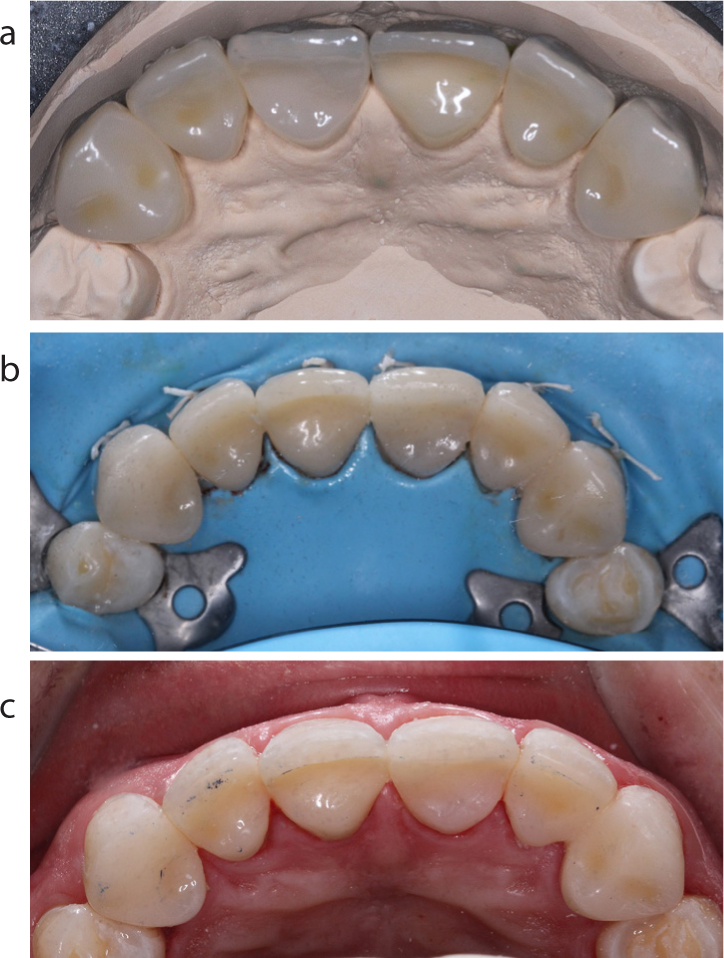
The first restorative appointment involved cementation of the indirect composite (TWiNY, Yamakin, Japan) palatal backings under rubber dam isolation for the six upper anterior teeth (Figure 6). TWINY is a light- and heat-cured indirect composite resin material chosen for the reasons outlined previously. The palatal backings extended over the incisal edge of the upper anteriors and up to the labial surface. This meant they could then be used as a palatal matrix for the freehand labial composite (Figure 7). The indirect composite backings were pre-treated by sandblasting with 50-micron aluminium oxide and application of a silane-containing dentine bonding agent (Scotchbond Universal Adhesive, 3M, UK). Cementation was carried out with a high-strength flowable composite (G-ænial, Universal Flo, GC Europe, Belgium). Labial direct composite was applied to restore the erosive wear that had occurred, as well as to disguise the join line between the tooth and indirect composite (GC Gradia Direct, GC Europe, Belgium). After minor adjustments, equal static contacts were confirmed on all six upper anterior teeth, with even protrusive guidance and canine guidance in lateral excursion. Good posterior disclusion was created after the first appointment. To reduce the effect of relative axial movement (Dahl effect), the patient was called back for restoration of the posterior teeth within the same week. Another option could have been to place posterior occlusal stops with direct restorations to preserve this space. The patient was extremely happy with the aesthetic outcome after this appointment and tolerated the increased OVD well.
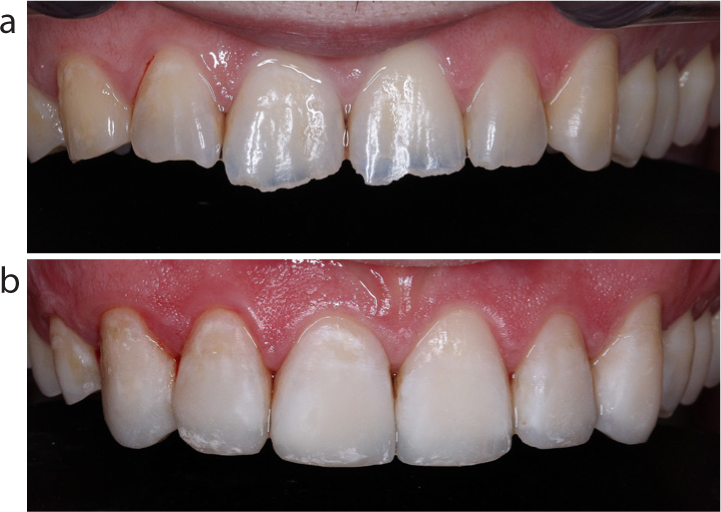
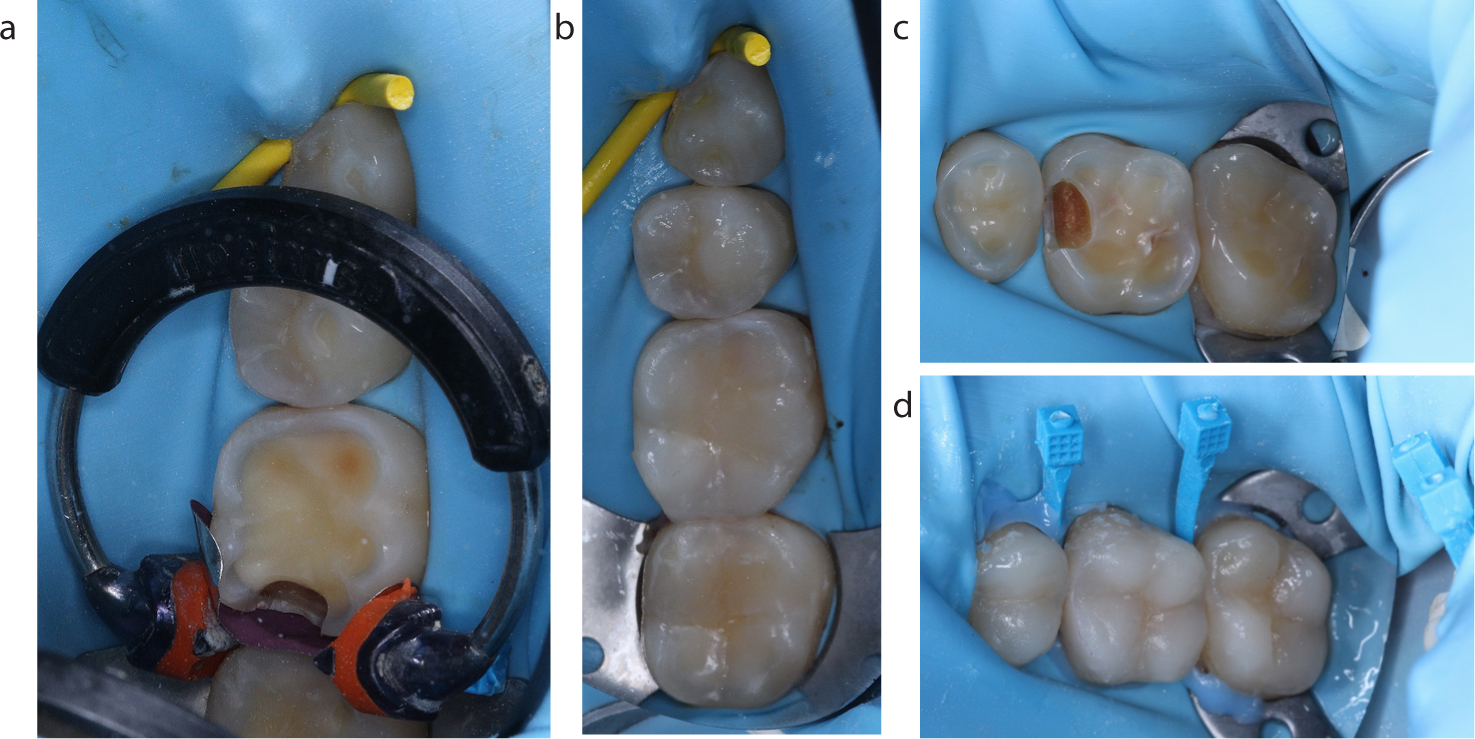
Figure 6. (a–c) Cementation of indirect palatal veneers.Figure 7. (a, b) Pre-operative and immediate post-operative view of anterior labial segment after placement of freehand direct labial composite.Figure 8. (a–d) Restoration of posterior teeth with direct composite build-ups and concurrent management of caries.
The reconstruction of the posterior teeth was completed over two appointments and involved direct composite build-ups to rebuild lost tooth tissue and cover over any areas of dentine exposure (GC Gradia Direct). Concurrent management of the carious lesions was also completed, and this was the only part of the patient's entire treatment that involved some removal of tooth structure. Another option with the direct build-ups could have been to use a transparent matrix to transfer a posterior wax-up over to the mouth. The decision to do the build-ups freehand was because of the good anatomical contour of the remaining teeth, and the need to rebuild several proximal walls, so incremental layering was required. Furthermore, the indirect backings had already set up good canine guidance, so final occlusion for the posteriors was relatively straightforward to achieve with static occlusal contacts and no further contact in lateral excursions.
Final outcome
The patient was initially placed on a 3-monthly high-risk recall pathway owing to his susceptibility to tooth surface loss and caries. However, after regular attendance for 2 years, the most recent review showed good adaptation of the composite with very little wear occurring and no chipping (Figure 9). During this time, he continued to adhere to the preventive regimen initially prescribed. The patient was aware that the direct composite restorations might need to be replaced by indirect restorations in the future, but that these should be possible to provide via a straightforward conformative approach.
This case showed how advances in bonding chemistry have allowed for traditionally destructive care plans to be provided in a minimally invasive way. Furthermore, preserving tooth tissue slows the passage of teeth through the restorative cycle, and allows for fallback options in the future to be provided. Good consent and discussion of the various options is key before beginning the treatment journey, so patients know the expected longevity of the restorations provided. With regards to tooth surface loss, managing the aetiological factor and a continued emphasis on prevention allows provision of predictable dentistry for patients.