Sumit S, Gambhir R, Singh S Radiosurgery in dentistry – a brief review. Ann Dent Res. 2012; 2:8-20
Bashetty K, Nadig G, Kapoor S. Electrosurgery in aesthetic and restorative dentistry: a literature review and case reports. J Conserv Dent. 2009; 12:139-144 https://doi.org/10.4103/0972-0707.58332
Vilos GA, Rajakumar C. Electrosurgical generators and monopolar and bipolar electrosurgery. J Minim Invasive Gynecol. 2013; 20:279-287 https://doi.org/10.1016/j.jmig.2013.02.013
Kalkwarf KL, Krejci RF, Edison AR, Reinhardt PA. Lateral heat production secondary to electrosurgery incisions. Oral Surg Oral Med Oral Path. 1983; 55:344-348 https://doi.org/10.1016/0030-4220(83)90186-x
Rathofer SA, Gardner FM, Vermilyea SG. A comparison of healing and pain following excision of inflammatory papillary hyperplasia with electrosurgery and blade-loop knives in human patients. Oral Surg Oral Med Oral Path. 1985; 59:130-135 https://doi.org/10.1016/0030-4220(85)90003-9
Liboon J, Funkhouser W, Terris DJ. A comparison of mucosal incisions made by scalpel, CO2 laser, electrocautery and constant voltage electrocautery. Otolaryngol Head Neck Surg. 1997; 116:379-385 https://doi.org/10.1016/s0194-5998(97)70277-8
Kalia V, Siddiqui N, Kalra G. Comparative analysis of radio surgery and scalpel blade surgery in impacted third molar incisions: a clinical trial. J Maxillofac Oral Surg. 2018; 17:458-465 https://doi.org/10.1007/s12663-017-1071-2
Sherman JA. Oral surgery simplified with radiosurgery. Dent Today. 2008; 27:123-124
Wilcox CW, Wilwerding TM, Watson P, Morris JT. Use of electrosurgery and lasers in the presence of dental implants. Int J Oral Maxillofac Implant. 2001; 16:578-582
Tom J. Management of patients with cardiovascular implantable electronic devices in dental, oral and maxillofacial surgery. Anesth Prog. 2016; 63:95-104 https://doi.org/10.2344/0003-3006-63.2.95.
Sherman J. Oral Radiosurgery: An Illustrated Guide, 3rd edn. London: Martin Dunitz; 2006
Noble WH, McClatchey KD, Douglass GD. A histologic comparison of effects of electrosurgical resection using different electrodes. J Prosthet Dent. 1976; 35:575-579
Yalamanchili PS, Surapaneni Davanapelly P Electrosurgical applications in dentistry. Sch J App Med Sci. 2013; 1:530-534
Kalkwarf KL, Krejci RF, Shaw DH. Subjacent heat production during tissue excision with electrosurgery. J Oral Maxillofac Surg. 1983; 41:653-657
Buzina DS, Lipozencic J. Electrosurgery – have we forgotten it?. Acta Dermatovenerol Croat. 2007; 15:96-102
Robertson PB, Luscher B, Spangberg LS, Levy BM. Pulpal and periodontal effects of electrosurgery involving cervical metallic restorations. Oral Surg Oral Med Oral Path. 1978; 46:702-710 https://doi.org/10.1016/0030-4220(78)90467-x
Krejci RF, Reinhardt RA, Wentz FM Effects of electrosurgery on dog pulps under cervical metallic restorations. Oral Surg Oral Med Oral Path. 1982; 54:575-582 https://doi.org/10.1016/0030-4220(82)90197-9
British Cochlear Implant Group. Safety for cochlear implant users. 2020. http://www.bcig.org.uk/safety/ (accessed March 2021)
Pisano P, Mazzola JG, Tassiopoulos A, Romanos GE. Electrosurgery and ultrasonics on patients with implantable cardiac devices: evidence of side effects in dental practice. Quintessence Int. 2016; 47:151-160
Roedig JJ, Shah J, Eli CS, Miller CS. Interference of cardiac pacemakers and implantable cardioverter-defibrillator activity during electronic dental device use. J Am Dent Assoc. 2010; 141:521-526
Ochsenbein C, Ross S. A re-evaluation of osseous surgery. Dent Clin North Am. 1969; 13:87-102
Gargiulo A, Wentz F, Orban B. Dimensions and relations of dentogingival junction in humans. J Periodontol. 1961; 32:261-267
Baba N, Goodacre C, Jekki R, Wom J. Gingival displacement for impression making in fixed prosthodontics. Contemporary principles, materials and techniques. Dent Clin N Am. 2014; 58:45-68 https://doi.org/10.1016/j.cden.2013.09.002
Radiosurgery allows precise tissue cutting with simultaneous haemostasis, providing a clearer surgical field. Variation in waveform, power settings and handpiece tip shape allow for a wide variety of clinical applications, making it one of the most versatile pieces of surgical equipment in the dentist's arsenal. However, it is one of the most underused, and probably misunderstood, areas of surgery in dentistry. This may be due to conflicting literature concerning healing, overshadowing of the value of the technique by interest in dental lasers, misuse of terminology and a general lack of knowledge regarding the science underpinning its action.
CPD/Clinical Relevance: This article aims to outline the mode of action, adjustable parameters and considerations for the safe use of radiosurgery alongside clinical examples of its applications.
Article
Timothy Brown
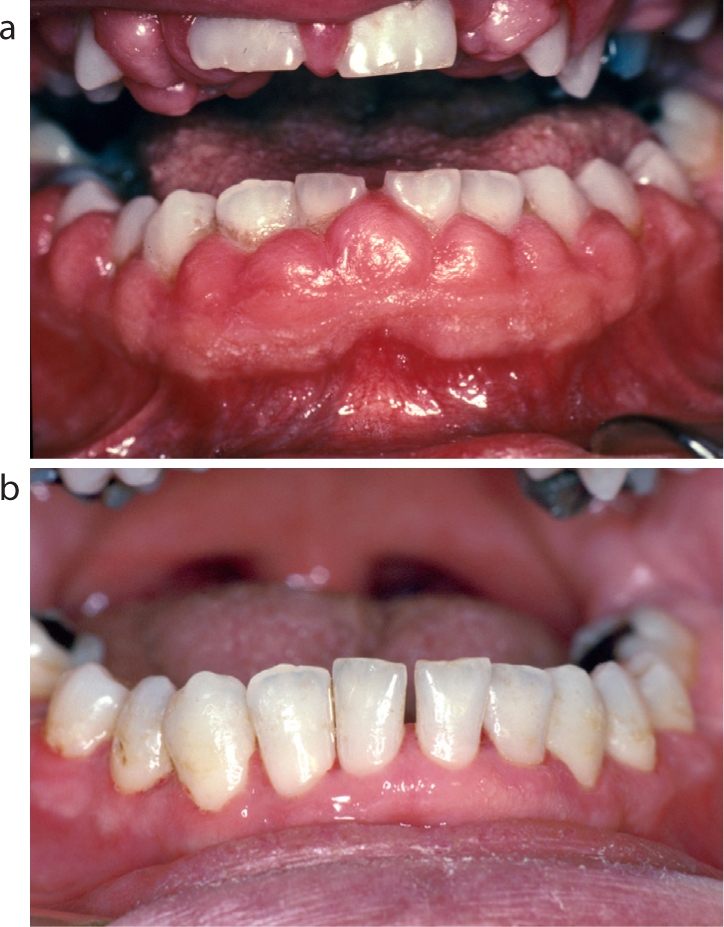
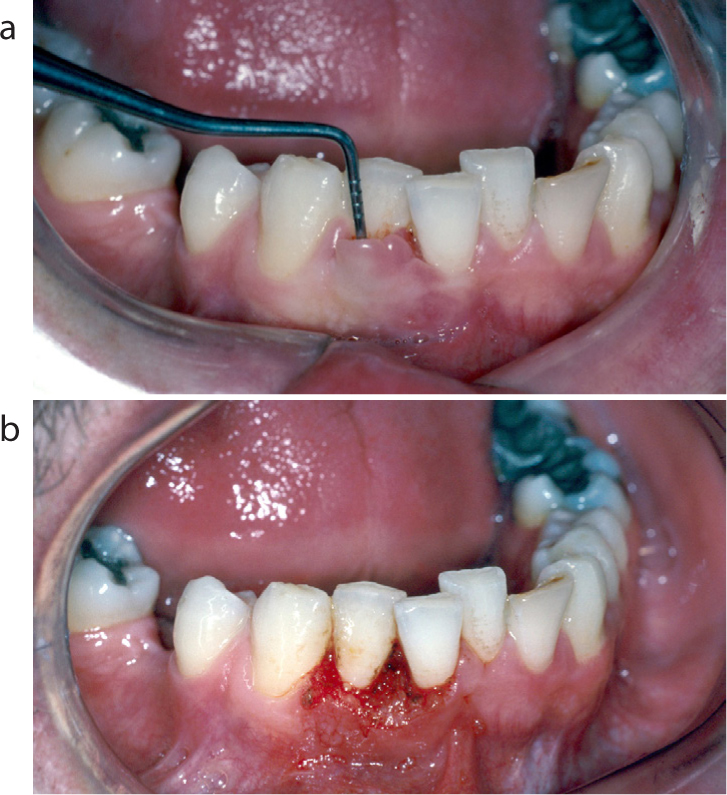
Despite improvements and advances in radiosurgery equipment over the years, the use of this surgical technique has remained relatively static in the dental community.1 Some reasons suggested for this have included the rise of the laser in dentistry, which has overlapping uses, but higher initial costs, along with historically conflicting literature over post-operative wound healing following radiosurgery.2 However, later research has demonstrated that concerns regarding adverse healing results were unwarranted when radiosurgery was used appropriately (Figure 1a, b).3,4
Figure 1. (a, b) Gingivectomy of a patient with drug-induced gingival hyperplasia. Notice the excellent gingival contour and excellent healing with no scarring in the post-operative photograph.
The authors of this article also feel that confusion with terminology, and a general lack of understanding of the mode of action, are other potential factors contributing to the reluctance to use radiosurgery. Limited knowledge of the scientific theory behind radiosurgery is common, and is not limited to dentists, with surgeons of all disciplines also admitting a lack of understanding of this technology despite its widespread use in operating theatres.5 This is not aided by the misuse of terminology, with diathermy, electrocautery, electrosurgery and radiosurgery being used synonymously, despite their having distinct modes of action, clinical properties and applications.
Mode of action
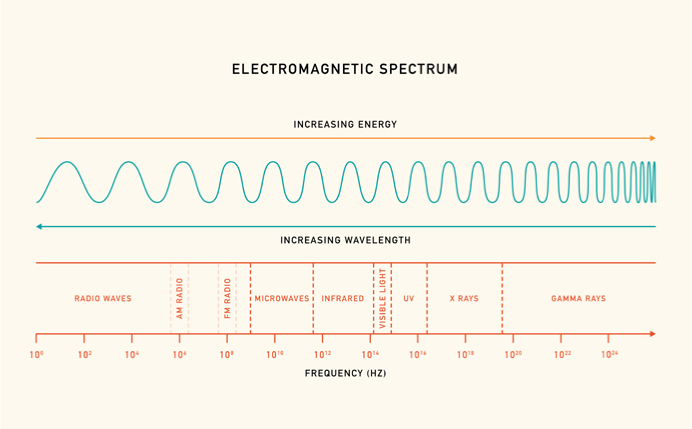
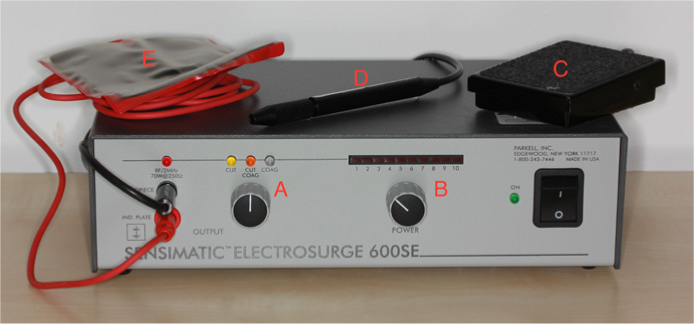
Electrosurgery and radiosurgery are related, but need to be considered on a spectrum; namely the electromagnetic (EM) spectrum (Figure 2). Originally, electrosurgery units were less efficient, emitting lower frequency and higher heat-producing energy, typically operating between 1.0 and 2.9 MHz. Some of the newer radiosurgical units (RSU) can produce outputs of 3–4 MHz, within the AM radiowave portion of the EM spectrum, hence the eponymous term. However, they can be more expensive to purchase, making lower-frequency machines more readily available. Monopolar RSUs produce radiowaves that are focused at the handpiece tip where they are converted into heat energy when impeded by the resistance inherent in tissue, resulting in either sectioning, or desiccation and coagulation of the tissues in immediate proximity. The residual energy is then dissipated through the body to be gathered by a collection pad (usually placed in the region of the patient's shoulders), recycling it back to the RSU (Figure 3).5
Figure 2. Diagrammatic representation of the EM spectrum with the AM radiowave frequency used by radiosurgery units displayed.Figure 3. A typical radiosurgery unit, annotated to show the waveform setting (A), the power setting (B), the foot pedal (C), the handpiece (D) and the collection pad (E).
The authors of this article recommend the use of the term ‘radiosurgery’ (in preference to ‘electrosurgery’ or ‘electrocautery’) because it is much less intimidating to patients when consenting to its use; the result is a calmer and more relaxed patient, devoid of worry from the incorrectly imagined potential for electrocution. For the same reasons, we recommend using the term ‘collection pad’ over ‘grounding plate’.
Heat transfer to tissues
The amount of heat generated in the tissues dictates the functional outcome, and understanding this principle is key to achieving the desired clinical result (be that cutting, haemostasis or both) while ensuring optimal tissue response and uneventful healing. It should be reinforced that it is the resistance inherent in tissue that causes radiowave energy to convert to heat, and not as a result of heat produced and transferred directly from the handpiece tip.
While heat generation is fundamental to radiosurgery functionality, it is important to acknowledge that there is the potential for unintended excess transfer of heat to neighbouring tissues, often referred to as ‘lateral heat’.6 Anecdotal reports about unwanted side effects of the use of radiosurgery such as tissue necrosis or bone sequestration are likely to be the result of an excessive build-up of lateral heat in the tissues.6 The main factors influencing lateral heat development include:
Power setting
Handpiece tip size
Time
Waveform setting
RSU operating frequency
The higher the power setting used (see Figure 3), the larger the handpiece tip and the longer the tip is in contact with the tissues while activated will all lead to higher levels of heat transfer. The waveform setting selected (see Figure 3) also directly affects the amount of heat transferred with the ‘coag’ setting associated with a higher likelihood of lateral heat production, the ‘cut’ setting producing the least and the ‘cut and coag’ setting in between them. Conversely, as highlighted in the previous section, the higher the operating frequency of the RSU, then the more efficient it is, resulting in less unwanted heat production. It should also be noted that heat transfer to the tissues can be actively dissipated by the use of high-volume aspiration and intermittent flushing of the surgical site with sterile saline, or equivalent, when there is concern about undue lateral heat development. These factors and the clinical implications for safe use are discussed in greater detail below.
Clinical applications
Radiosurgery can be used to incise, excise, plane, sculpt or ablate soft tissues while providing a surgical field with reduced bleeding in comparison to conventional surgery.7,8 For clinicians, this means better visibility, potentially making operations safer, less stressful and quicker, with an associated reduction in surgery time.1,9 For patients, less blood pooled or ingested means a more comfortable experience and consequently, reduced apprehension if repeat treatment is necessary in the future.10 Indeed, questionnaires at the time of surgery found a greater number of patients reported less unpleasantness with the radiosurgery technique versus the conventional scalpel for inflammatory papillary hyperplasia removal.7
The reported uses for radiosurgery in dentistry are listed in Table 1. Please note this list is not exhaustive, represents a cross-section of uses reported in the literature and is for illustrative purposes only. Examples of clinical cases using radiosurgery by the authors are seen in Figures 1 and 4–9, with descriptions.
Procedure
Exposure of subgingival cavities to facilitate direct restoration
Exposure of subgingival margins to allow direct or indirect restoration
Gingival troughing prior to impression-taking
Haemostasis
Gingivectomy to increase bonding area for resin bonded bridges
Sculpting gingivae for better emergence profiles for resin bonded bridge pontics
Gingivectomy of hypertrophic tissue
Pocket reduction surgery
Frenectomy
Operculectomy
Incisional or excisional biopsy
Surgical extraction incisions
Pulpotomy
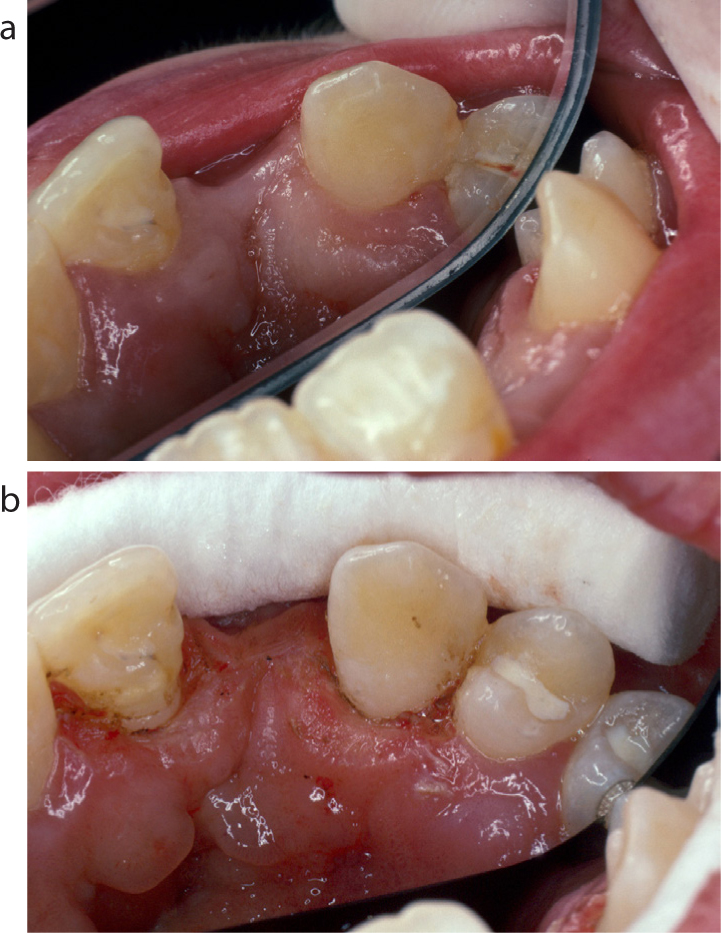
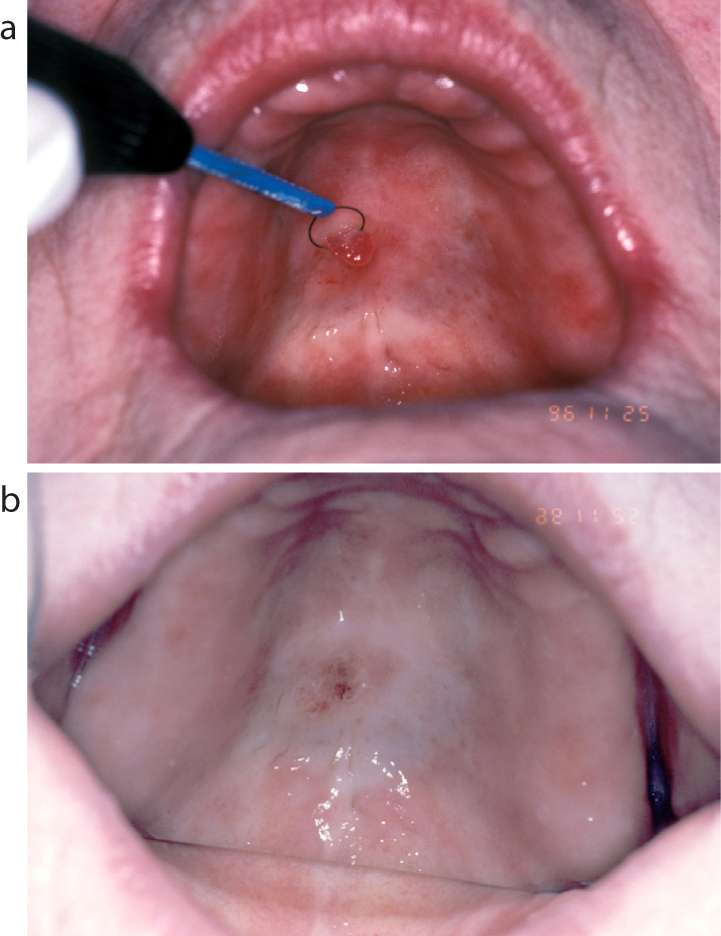
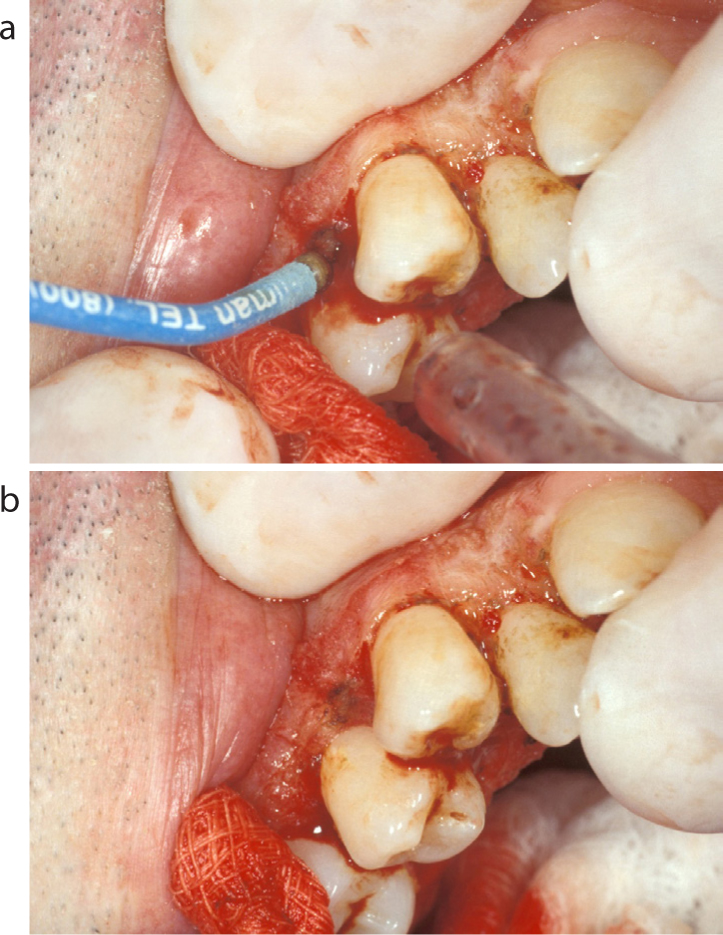
Figure 4. (a) Pre-operative view of failing cervical restorations LR3, LR4. The full extent of the restoration is covered by hypertrophic gingiva making adequate access impossible. (b) Resection of excess gingiva LR3, LR4. Note the use of the diamond-shaped tip at a 45-degree angle to the long axis of the tooth; in one sweep this allows resection as well as simultaneous gingival contouring to develop the correct emergence profile. (c) Immediate post-surgery view. Note the immaculate haemostasis and now excellent visualization of the failing restorations LR3, LR4 to allow replacement.Figure 5. (a, b) Pre- and post-resection of palatal gingiva UL1, UL3 to significantly increase the bonding area of enamel prior to resin bonded bridge placement.Figure 6. (a) View of LL5 after crown removal. The gingiva has overgrown the preparation margin making further preparation and adequate pick up of the margin by an impression difficult. (b) Use of a fine straight tip held at 45 degrees to the long axis of LL5 to trough circumferentially around the preparation margins to enable complete visualization. (c) Buccal view of LL5 immediately after completion of radiosurgery. Note the improved gingival contour, excellent visualization of the preparation margins and large amount of extra coronal tooth structure now visible for preparation refinement.Figure 7. (a) Pre-operative view of LR2 with 6 mm false pocket on the labial aspect, demonstrated with a Williams probe held in situ. (b) Immediate post-operative view of LR2 after pocket reduction surgery using radiosurgery. Note the ease with which it is possible with this technique to extend the surgical site onto the labial aspect of the alveolus, and thin the surrounding attached gingiva to ensure correct gingival profile, optimizing aesthetics once healing is completed.Figure 8. (a, b) Pre- and post-operative use of a loop-shaped tip to excise an area of denture-induced hyperplasia affecting the palate. The use of radiosurgery ensured excision and haemostasis happen concurrently.Figure 9. (a) Use of a ball-ended tip to provide haemostasis of a bleed from the gingiva. The radiosurgical unit is set to ‘coag’ and the tip is lightly held against the bleeding point before activation. (b) This shows the excellent haemostasis achieved with the ball tip along with a small area of associated charring of the tissues that is acceptable.
Equipment variables
Radiosurgery can have a wide variety of applications because of the wide range of equipment factors and settings affecting clinical output that can be adjusted by the operator. Although this can lead to confusion for the novice user, once understood, it opens up safe application of radiosurgery to the extensive range of clinical scenarios. These variables are discussed in more detail below.
Monopolar and bipolar
Monopolar is the most common type of RSU and its method of function has been described above.
Bipolar RSUs negate the need for a collection pad by having a second antenna adjacent to the first, most commonly in the form of a tweezer configuration used for achieving pinpoint haemostasis. The radiowaves travel from one tip to the other, affecting only the tissue held in between, and not through the rest of the body.5 This means it may be used with suitable caution in close proximity to metal restorations or implants,1,11 and there is no risk of interference with pacemakers (see ‘Precautions’ below).12 Unfortunately it has poor resection properties, so bipolar devices offering cutting functions are actually a mechanical blade sandwiched between the elements and are inferior to monopolar device incisions.2
Waveform
There are four main waveforms relevant to radiosurgery: fully rectified and filtered, fully rectified, partially rectified and fulguration.1 See Table 2 for a summary of their relevant details.
Waveform
Usage
Tissue sectioning
Coagulation
Lateral heat
Usual RSU setting
Fully rectified, filtered
Pure cutting
Excellent
Minimal
Least
Cut
Fully rectified
Cutting with haemostasis
Very good
Very good
More
Cut + Coag
Partially rectified
Coagulation of soft tissue
Very poor
Excellent
Greater
Coag
Fulguration
Superficial destruction and coagulation
None
Excellent for osseous surgery
Greatest
Not available on modern RSUs. Use not recommended
Fully rectified and filtered
This is a continuous high-frequency energy that will result in a precise incision with minimal lateral heat transfer or coagulation of the adjacent tissues, and can be used with confidence in close proximity to bone. This is the ‘cut’ setting on a RSU, and is best thought of as being most analogous to a scalpel blade when used in conjunction with a fine tip.
Fully rectified
This provides a good but slightly less precise incision with higher lateral heat transfer meaning a greater measure of coagulation is usually achieved simultaneously. As a result, this waveform is best used in cases where significant bleeding is expected on incision, and is normally selected with the ‘cut and coag’ setting on a RSU.
Partially rectified
This is the ‘coag’ setting on devices and, as suggested, induces efficient haemostasis due to higher levels of heat transfer to adjacent tissue. It has very poor tissue cutting qualities and should never be used for this purpose.
Fulguration
From the Latin, meaning ‘lightning’, this is the production of a spark that results in cauterization and carbonization of adjacent tissue. This is no longer seen on modern devices as it produces large amounts of lateral heat with associated tissue damage and provides no tissue sectioning capability.
It is vital to ensure the correct waveform is used, and therefore, the correct RSU setting selected, for the clinical procedure planned, to ensure efficacy of clinical outcome. Using the partially rectified waveform for incision will result in an extremely poor cut with associated heat damage to nearby tissues. Conversely, a fully rectified and filtered waveform may be less likely to achieve an acceptable degree of coagulation in bleeding tissues.
Power setting
The correct power setting will allow a smooth incision or adequate, instant haemostasis. If the power setting is too high, then sparking and charring of the tissues will occur. Conversely, a suboptimal power setting will result in inefficient haemostasis and/or dragging of the radiosurgery tip through the tissues resulting in ragged margins and tissues sticking to the hand-piece tip.1 The former is preferable to the latter to avoid extending the contact time with tissues of an activated tip, but unnecessarily high power settings will result in needless heat production and tissue damage. Unfortunately, due to the variation in resistance of different tissues and between different patients, there are no set rules for power settings and they must be adjusted as required, intra-operatively. When changing between tips, it is important to remember that a tip with a larger surface area will usually require a higher power setting to exhibit similar cutting performance.13
Hand-piece tip
A major advantage of radiosurgery over conventional scalpels is the different shapes of tips available that can be bent as desired to allow more ergonomic access and better visualization of the surgery site for the operator. The high temperatures developed by the tips mean they are in effect self-sterilizing, preventing seeding of bacteria during deep incisions,13 and they negate the small but still significant risk of sharps injury that conventional blades pose.14
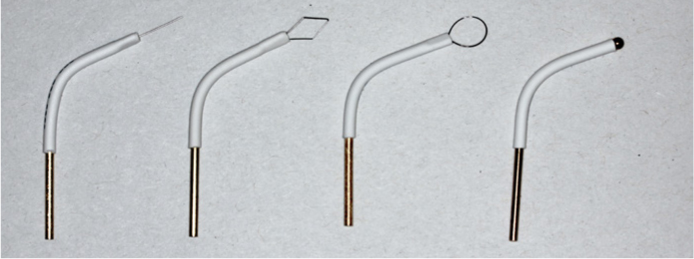
Tips can typically be divided by shape into three categories: straight; loop (including diamond); and ball (see Figure 10). It is vital to ensure the appropriate tip is selected for the desired procedure. Incisions are best performed with the thinnest straight tip available; loop tips are best suited for excisions and sculpting tissues; ball shaped tips are the most efficient for achieving haemostasis.15 It should be noted that it has been demonstrated that the larger the surface area of the tip, the greater the amount of heat imparted into the tissues, which in turn affects the time recommended between incisions (see ‘Incision planning’ below).16
Figure 10. Photograph of the main handpiece tip types that may be used with a radiosurgery unit. The tips may be bent along the length of the insulating collar to allow more ergonomic use.
Precautions
If the principles outlined above are adhered to, radiosurgery is extremely safe to use; however, there are some particular precautions that should be noted.
Speed of incision
When resecting tissue, it has been recommended that incisions should be performed at a minimum of 7 mm/second for no longer than 1–2 seconds to avoid unwanted heat development in the tissues.17,18
Incision planning
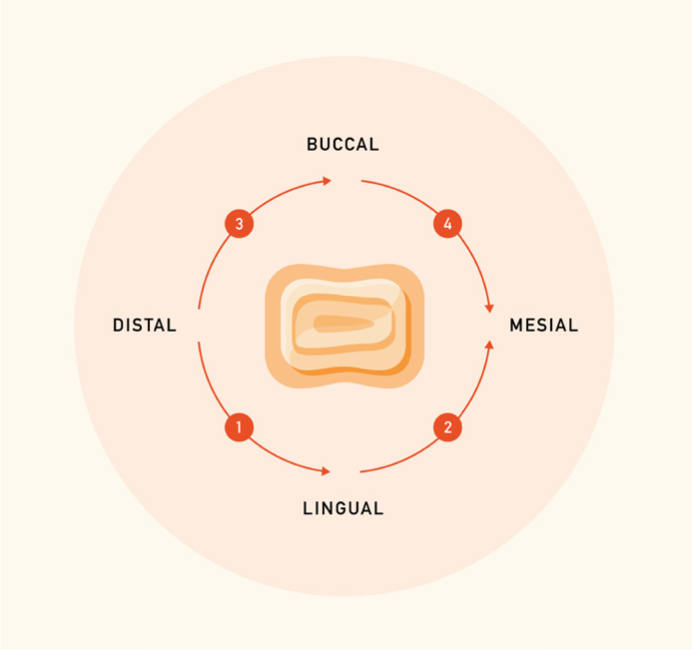
The potential for heat to build up in the tissues affects not only the speed of the incision, but also the order of incisions and the time between incisions at the same site. For effective time management, it is important to plan incisions to reduce the chance of unnecessary lateral heat development by accommodating the recommended delay before re-instrumenting the same site. For thin straight tips this has been advised to be 8 seconds,6 and 15 seconds for loop style tips, owing to the higher levels of heat they pass to the tissues and extra time this requires to dissipate.19 An example of advised incisions for the circumferential resection of a tooth can be seen in Figure 11, with the steps suggested being an efficient way to allow adequate heat dissipation from the tissues in the timeliest manner.
Figure 11. Line drawing depicting step-by-step the most time efficient method to perform a circumferential resection of a tooth, while minimizing the risk of lateral heat development.
Smoke production
Heat application to organic tissues will typically result in the production of smoke and a disagreeable odour. As well as being unpleasant for the patient and operator to inhale, the smoke has been shown to potentially contain bacteria and virus particles.20 Consequently, appropriate surgical masks should be used by the operators, along with constant and accurately positioned high-volume suction never more than 5 cm from the surgical site (see Figure 9a). However, overzealous suction can lead to desiccation of the soft tissues, which is important to avoid as it can lead to the tip dragging and a ragged, suboptimal incision.
Pooled liquids
Application of a ball-ended monopolar electrode to pooled liquids – especially when used in conjunction with the coagulation or partially rectified waveform – can lead to sparking and unwanted lateral heat transfer to the adjacent tissues. Since pooled blood, saliva or saline irrigant can cover a wide surface area adjacent to the operating site, care should be exercised to avoid the delivery of unintended heat to remote tissues, with attendant adverse consequences for the unwary.
Metallic restorations and implants
When a monopolar tip comes into contact with metal, it can result in sparking and the potential for heat transfer and damage to the surrounding tissues.21 This is significant when operating in close proximity to cervical amalgam restorations, metal-containing crowns, metallic oral piercings or dental implants. However, research has shown no damage to the pulp occurs as long as contact with a metal cervical restoration is for less than 0.4 seconds.22 Although there is a dearth of research confirming the potential for loss of osseo-integration of implants when radiosurgery energy is actively applied to them, it has been recommended that the judicious use of bipolar radiosurgery can be undertaken with confidence, but monopolar radiosurgery in close proximity to implants should be avoided.11
Implantable electronic devices
Cochlear implants have been shown to be potentially sensitive to electromagnetic interference and as such, the use of radiosurgery is contraindicated for these patients by the majority of implant device manufacturers.23
Despite modern cardiovascular implantable electronic devices (CIED), such as pacemakers, being very well insulated, there is still significant conflict in the literature around the potential of monopolar RSUs to interfere with their function.12,24,25 Owing to a lack of scientific consensus and the significant potential consequences of interference, it is recommended that contact is made with the patient's cardiologist prior to use. If radiosurgery is performed for such patients, then it is advised to place the collection pad as close to the surgery site and as far away from the CIED as possible, along with the minimum usage to achieve an acceptable clinical outcome.11,12 Alternatively a bipolar RSU may be used with reportedly no concern regarding interference.12
Flammable liquids and gases
Sparking may occur occasionally with radiosurgery, especially if metal is touched or power settings are excessive. Thus, it is recommended that all flammable products, such as ethyl chloride, should not be used in close proximity to a RSU while in use.1
Gingival biotype and biological width
As with any procedure involving the gingiva, the usual precautions concerning gingival biotype and respect for the biological width should be assessed and accounted for pre-operatively, particularly in aesthetic zones. Two main biotypes are described: thick and thin.26 The former is noted as having thicker and more fibrotic gingiva and usually heals predictably. The thin biotype needs to be treated with more caution, with its thin friable nature and commonly associated underlying bony fenestrations and dehiscences predisposing it to recession after any form of surgery.27
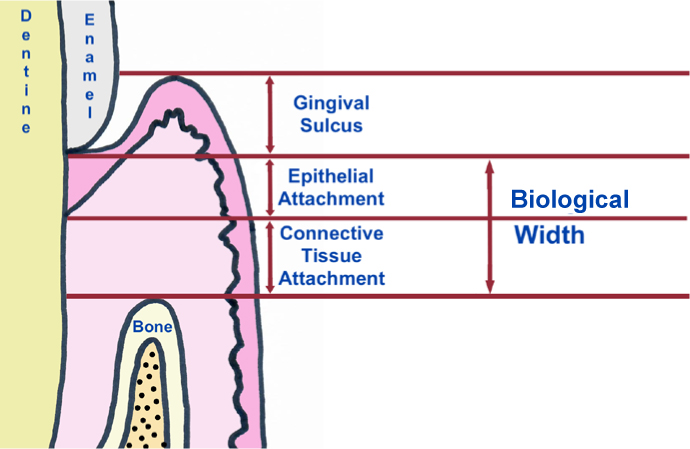
The biological width can be defined as the tissue separating the gingival sulcus and the alveolar bone crest, usually estimated as being 2 mm in depth and comprising the junctional epithelium and underlying connective tissue (Figure 12).28 Any surgery that violates the epithelial or connective tissue attachment at the base of the sulcus may result in inflammation and recession, so caution must be exercised when working in proximity to this apparatus.29
Figure 12. Cross-sectional diagram of the periodontal apparatus with the biological width highlighted.
Conclusion
While radiosurgery will never make the scalpel redundant, the authors hope this article has highlighted the many benefits it offers, along with clinical situations where its use may be advantageous over the traditional surgical blade. We hope the factors for efficient and safe use discussed (and summarized in Table 3) will provide the knowledge base to encourage more practitioners to look to incorporate it into their day-to-day practice and discover the benefits first hand.
Summary of recommendations for safe and efficient radiosurgery use
Use the term ‘radiosurgery’ when discussing its use with patients
Use the most appropriate waveform and handpiece tip for the intended surgical purpose:
Pure incision is best achieved with the fully rectified and filtered (‘cut’) waveform with the thinnest tip
Incision or resection of tissue that is expected to bleed significantly is best performed with the fully rectified (‘cut + coag’) waveform
Haemostasis is best achieved with the partially rectified (‘coag’) waveform with a ball tip or pencil-shaped tip held lightly on the tissue
Actively monitor and adjust the power setting as required between different tissues, different patients and different tips intra-operatively
Aim for a smooth, pressure-less incision with no sparking and minimal charring
Beware electrode contact with metallic restorations and avoid contact for more than 0.4 seconds
Do not activate the tip while in contact with tissue for longer than 1–2 seconds, if kept stationary
Ensure incisions are made at a minimum speed of 7 mm/second
Plan incisions to allow 8–15 seconds between treatment of the same site, depending on the tip used
Ensure tissues at the site of surgery are adequately moist, and neither overly desiccated nor bathed in pooling liquid
Avoid use near flammable liquids or gases
Discuss with a patient's cardiologist the use of radiosurgery in patients with cardiovascular implantable electronic devices prior to use
When radiosurgery is performed on patients with cardiovascular implantable electronic devices, keep the amount of surgery to a minimum, and position the collection pad as far from the device and as close to the surgery site as possible
Use normal saline to clean any areas of charred tissues post resection, especially before impressions or the patient leaving the surgery