Marbach JJ. Phantom bite. Am J Orthod. 1976; 70:190-199
Marbach JJ. Phantom bite syndrome. Am J Psychiatry. 1978; 135:476-479
Marbach JJ, Varoscak JR, Blank RT, Lund P. Phantom bite: classification and treatment. J Prosthet Dent. 1983; 49:556-559
Kelleher M. Regulators and regulations: who will guard the guards? (or ‘Quis custodiet ipsos custodes’ as old Juvenal used to say). Dent Update. 2015; 42:406-410
Hara ES, Matsuka Y, Minakuchi H, Clark GT, Kuboki T. Occlusal dysesthesia: a qualitative systematic review of the epidemiology, aetiology and management. J Oral Rehabil. 2012; 39:630-638
Tsukiyama Y, Yamada A, Kuwatsuru R, Koyano K. Bio-psycho-social assessment of occlusal dysaesthesia patients. J Oral Rehabil. 2012; 39:623-629
, 4th edn. Arlington, VA, USA: American Psychiatric Association; 2000
Arlington, VA, USA: American Psychiatric Association;
Marbach JJ. Orofacial phantom pain: theory and phenomenology. J Am Dent Assoc. 1996; 127:221-229
Cunningham SJ, Feinmann C. Psychological assessment of patients requesting orthognathic surgery and the relevance of body dysmorphic disorder. (PMID: 9884781). Br J Orthod. 1998; 25:293-298
Klineberg I.Oxford: Butterworth Heinemann; 1991
Marbach JJ. Psychosocial factors for failure to adapt to dental prostheses. Dent Clin North Am. 1985; 29:215-233
Kelleher M. Porcelain pornography. Fac Den J. 2011; 2:134-141
Jagger RG, Korszun A. Phantom bite revisited. Br Dent J. 2004; 197:241-243
Reeves JL, Merrill RL. Diagnostic and treatment challenges in occlusal dysesthesia. J Calif Dent Assoc. 2007; 35:198-207
Ligas BB, Galang MT, BeGole EA Phantom bite: a survey of US orthodontists. Orthodontics (Chic). 2011; 12:38-47
Toyofuku A, Kikuta T. Treatment of phantom bite syndrome with milnacipran – a case series. Neuropsychiatr Dis Treat. 2006; 2:387-390
Watanabe M, Umezaki Y, Suzuki S Psychiatric comorbidities and psychopharmacological outcomes of phantom bite syndrome. J Psychosom Res. 2015; 78:255-259
Melis M, Zawawi KH. Occlusal dysesthesia: a topical narrative review. J Oral Rehab. 2015; 42:779-785
The paradoxes of phantom bite syndrome or occlusal dysaesthesia (‘dysesthesia’) Martin G Kelleher Lakshmi Rasaratnam Serpil Djemal Dental Update 2024 44:1, 707-709.
Authors
Martin GKelleher
Consultant and Specialist in Restorative Dentistry and Prosthodontics, King's College London Dental Institute, London SE5 9RW, UK
Phantom bite syndrome was first described by Marbach over 40 years ago as a mono-symptomatic hypochondriacal psychosis. He used the term to describe a prolonged syndrome in which patients report that their ‘bite is wrong’ or that ‘their dental occlusion is abnormal’ with this causing them great difficulties. This strong belief about ‘their bite’ being the source of their problems leads to them demanding, and subsequently getting, various types of dentistry carried out by multiple dentists and ‘specialists’. Sadly, even after exhaustive, painstaking, careful treatment, none of the dental treatments manages to solve their perceived ‘bite problems’. This is because they suffer from a psychiatric illness involving a delusion into which they continue to lack insight, in spite of the failures of often sophisticated dental treatments.1,2,3
In summary, dental practitioners, or other specialists, who suspect that they might be dealing with such a problem should refer these patients early on for specialist management by an appropriate specialist within the secondary care settings, preferably before they get trapped into the time-consuming quagmire of their management. A ‘Phantom Bite Questionnaire’, which is available to download free, might help.
CPD/Clinical Relevance: This article aims to provide professionals in various fields with guidelines on detecting, diagnosing and managing patients with Phantom Bite Syndrome (PBS). This is desirable in order to prevent extensive, or unnecessarily destructive, or unstable dental treatment being undertaken on such patients in a vain attempt to solve their problems with ‘dentistry’ when, in fact, these are really due to underlying mental health issues.
WARNING
Phantom bite patients are often highly resistant to being referred to psychiatrists as they lack insight into their behaviour. They often complain if even a gentle suggestion is made of a possible referral to a psychiatrist. They remain resolutely convinced that if they could only get someone competent enough to get their ‘bite right’ then all their problems would be solved.
Article
Introduction
There are many difficult paradoxes in dentistry generally, but phantom bite syndrome is riddled with them. For instance, if a diagnosis of phantom bite syndrome, or occlusal dysaesthesia (dysesthesia), is suspected then the offer to refer the patient to an ‘occlusion specialist’ can, paradoxically, serve merely to confirm in patients' minds that there is something seriously wrong with them and that their perceived problems really are being caused by ‘their bite’. For other dentists, another paradox is that apparently technically excellent dentistry fails to satisfy these patients' demands about their bite and they then often become serial, time-consuming complainers. They often write very long letters (‘graphitis’) detailing their problems. These letters or emails sometimes include details of the ‘research’ that they have done frequently with the help of Professor Google to support their view that their various, sometimes bizarre, symptoms, often in remoter areas of their bodies, have all been caused by alleged imperfections in their occlusion or bite. They frequently have unusually long appointments, some unscheduled, in various vain attempts to ‘sort out their bite problems’. However, eventually that particular dental clinician's treatment is declared a failure. The phantom bite syndrome patient then moves on to other general dentists, sometimes one with a special interest in occlusion, or to consult with a dental specialist of some sort. Some complain to various ‘regulators’,4 or to administrators, or sometimes to an apparently omniscient lawyer about the previous dentist's, or the dental profession's, alleged incompetence in not getting their bite or their ‘occlusion’ quite right.
Another paradox is that, even if the diagnosis of ‘phantom bite’ is made by a clinician who is familiar with these problems, the patient then often refuses referral to a psychiatrist to confirm that diagnosis, or to attempt to treat it and can complain bitterly if such a suggestion is made even gently to him/her.
Sadly for all concerned, these patients fall into the category of ‘refractory to any dental treatment’, even after hundreds of hours of appointments. Many of these hours are spent on prolonged consultations and involve a variety of interventions of variable destruction, stability, rationality or retrievability. Unfortunately, none of these treatments, however well-intentioned or meticulously carried out, effectively cures the affected patient's prolonged concerns about ‘their bite’ or ‘dental occlusion’, because the problem is mental illness and is not amenable to even very elaborate dental treatment.
Occasionally, their behaviour and persistent demands for treatment can result in hospital security, or the police, having to be called in order to remove them from the premises (see Case PB3 below). Two patients in this case series have attempted suicide – one shortly after travelling over 200 miles for a specialist consultation.
In some other cases, clinicians involved have had to obtain legal injunctions to stop harassment of them and/or their support staff, or their family at their homes or practices.
Regulators, administrators and indemnifying organizations have become involved in various cases and at various stages. As most people working in those organizations are unlikely to be familiar with this relatively rare condition, they do not know what to look out for before assuming that the complaining patient is rational, or mentally healthy, or that their sometimes vindictive complaints are justified.
In 1976, the term ‘Phantom bite’ was introduced by Marbach to describe patients who were preoccupied with their supposedly abnormal dental occlusion. He considered the condition to be a form of mono-symptomatic hypochondriacal psychosis (abbreviated at the time to ‘MHP’) in which a fantasy regarding a single problem about their dental occlusion dominated their whole lives.1,2,3 This is no longer the preferred term used by psychiatrists. More recently, versions of what sounds remarkably like Phantom Bite Syndrome (PBS) have appeared occasionally in the literature, sometimes being referred to as ‘Occlusal Dysaesthesia’ (The American spelling is ‘Occlusal Dysesthesia).5,6
The Diagnostic and Statistical Manual of Mental Disorders (2000) previously used by psychiatrists to classify mental illnesses (DSM–IV–TR version) referred to this sort of condition as being one of a number of ‘Somatoform Disorders’.7
The current American Psychiatric Association's DSM V (2013) preferred term is ‘Somatic Symptom Disorder’.8
Whatever the current preferred psychiatric term being advocated, those patients with ‘Phantom bite syndrome’, or ‘Occlusal dysaesthesia’, can become nightmare patients for themselves, their family and dentists. They usually attend any new dentist, or specialist, as apparently routine patients, but often complain that their ‘bite is wrong’ in a very intense, characteristic way, often using dental terms such as ‘interferences’ or ‘slides’ or ‘cusps’ or ‘guidance’ or other bits of dental jargon and describing how badly this has affected them.
Sometimes their problems with ‘their bite’ is not their first complaint and instead they are adamant that their ‘teeth do not look right’ and/or that their bite or ‘dental occlusion is wrong’ and that this is causing them sometimes quite weird problems elsewhere in their body.
They undergo extensive tests and dental treatment by multiple dental practitioners who, initially flattered by the patient's praise for their ‘knowledge of occlusion’, at the beginning of the relationship, are often keen to try to resolve the patient's reported suffering, which is, allegedly, all due to his/her ‘bite’ or ‘occlusion’.
Patients firmly believe that their reported symptoms, which sometimes sound quite strange, particularly when they are to be present in remoter areas of their body, will also be cured just by getting ‘the right bite’ or ‘the bite right’. Sometimes their partners are convinced of this as well. In psychiatric terms, this is known as a ‘folie a deux’ (a delusion shared by two people). Sometimes an inexperienced, or naïve, but enthusiastic, ‘occlusion focused’ dentist joins in this folly.
These patients often appear to be superficially knowledgeable about how their teeth should ‘bite normally’, but will sometimes also demonstrate how they meet in ‘different excursive movements’. Sometimes, they expound quite elegantly on their views about their bite, cusps, slides or interferences or ‘locking of their occlusion’ and/or offer various ideas on what they need to have done to ‘correct their bite’ (Figures 2–4).
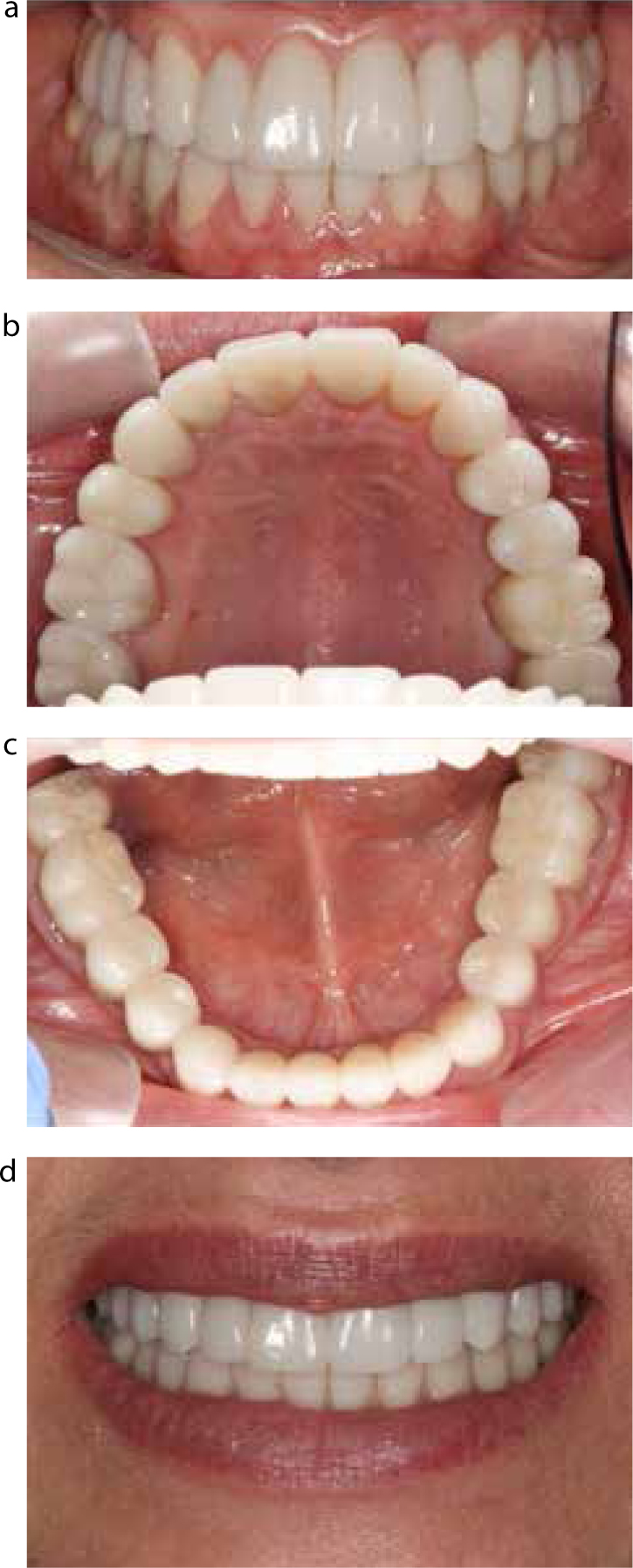
Figure 1.
(a–d) Clinical photographs demonstrating a third full mouth reconstruction with all ceramic crowns provided by a specialist to ‘correct the bite.’ Unfortunately, this extensive treatment did not cure the patient's symptoms either and she presented with suggestions for further adjustments to ‘perfect’ her occlusion.Figure 2.
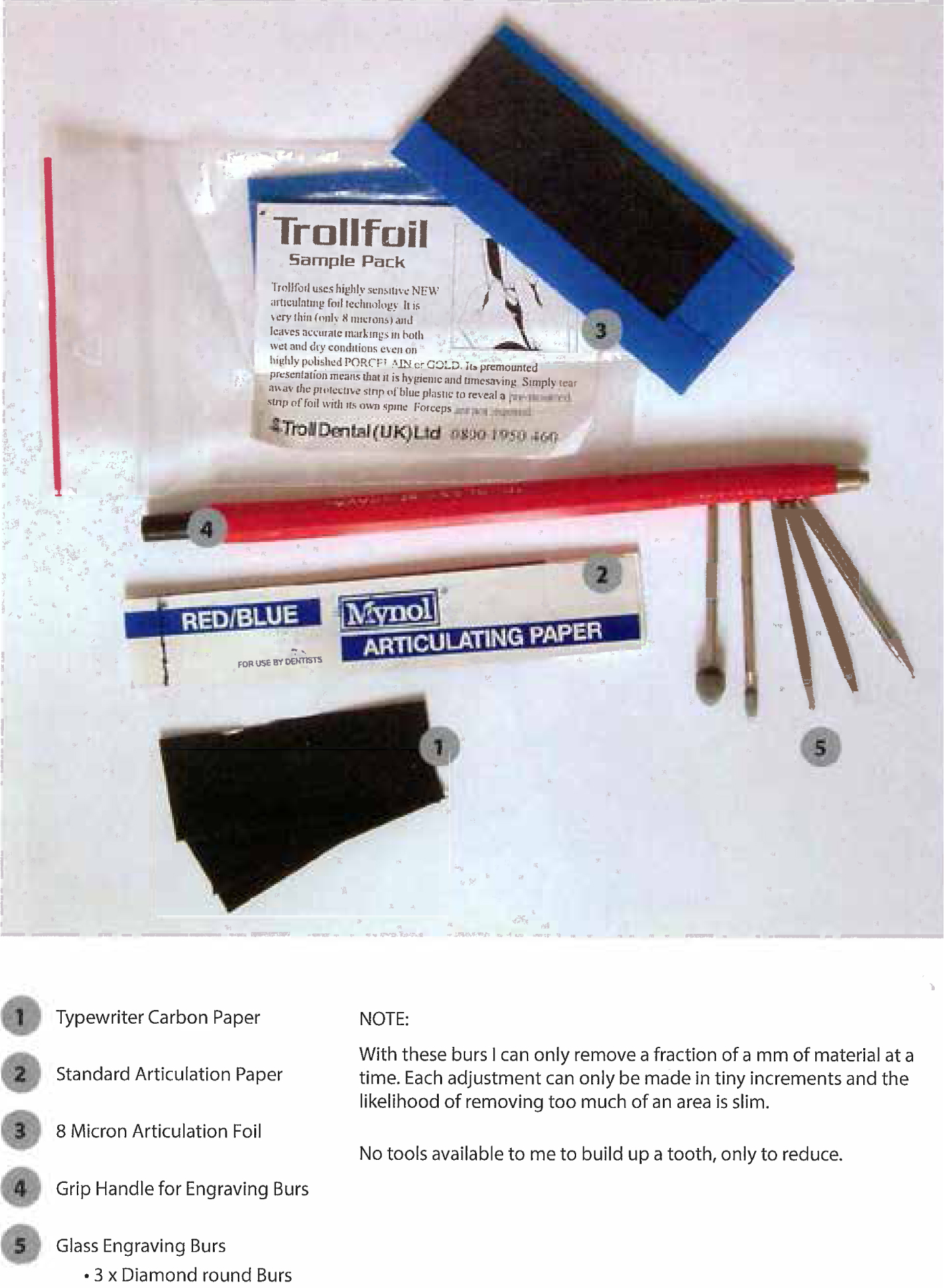
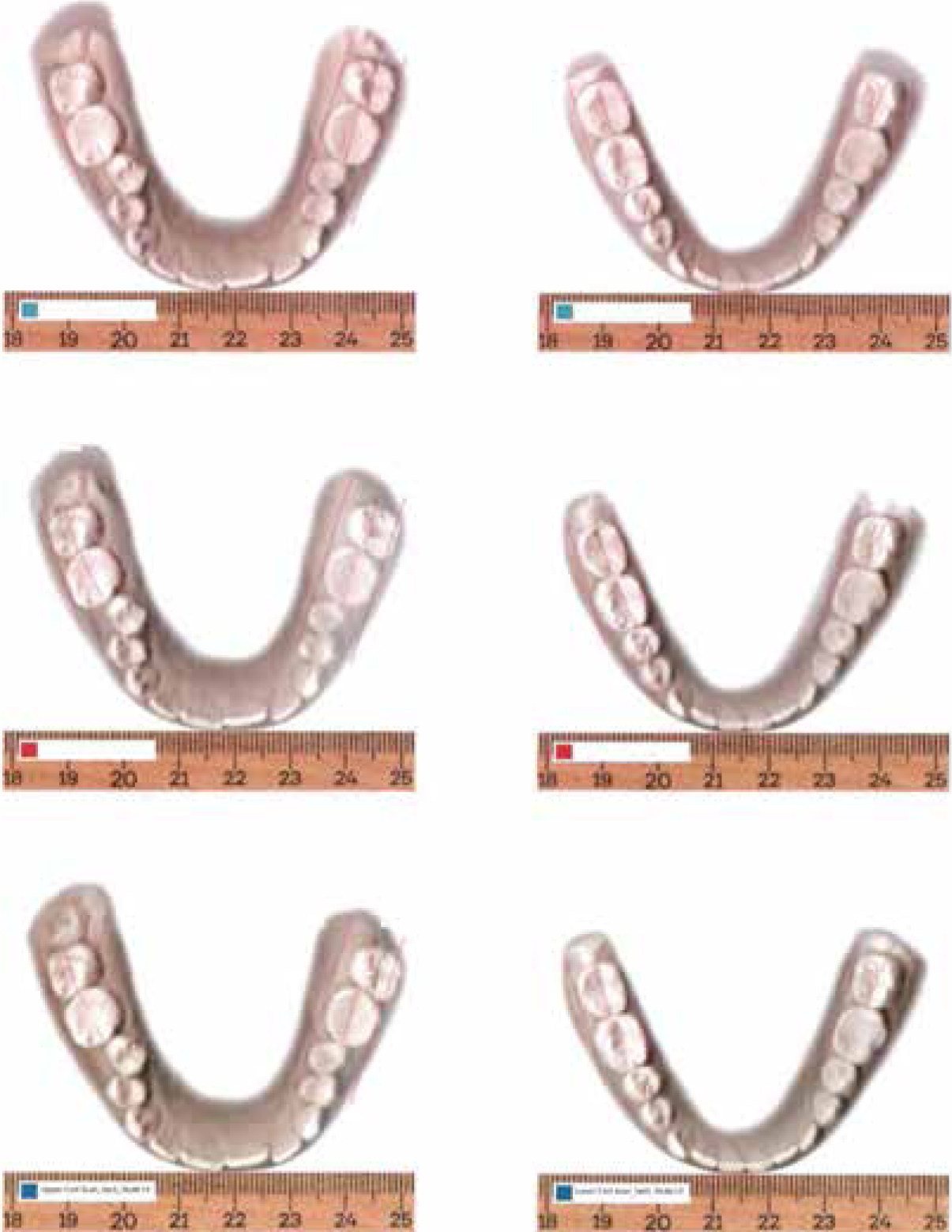
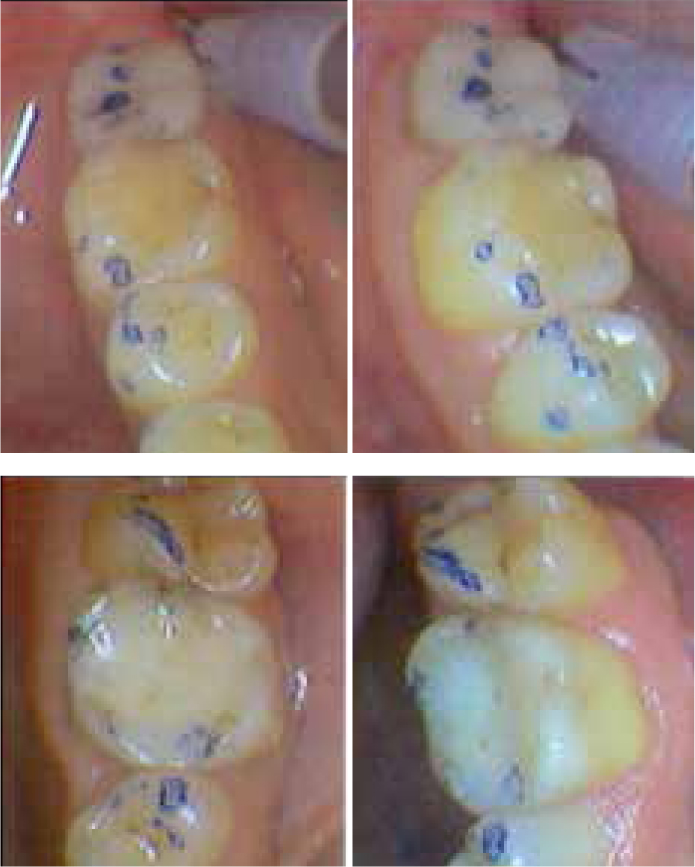
Case 1: Tools used. Hand tools only.Figure 3. Case 1: Computer-generated scans of her study models made by the patient herself with detailed measurements ‘of her bucco-lingual discrepancies of the LR7’.Figure 4. Case 1: Photographs taken by the patient herself, highlighting the occlusal contacts that she had marked herself and that she ‘knew needed to be ground down’. Apparently she did this with a Dremel DIY drill because ‘no dentist could see what needed to be done’.
If a concerned dental clinician suggests that all the reported problems in remoter parts of the body are not being caused by the bite and gently offers to refer the patient for mental health support then, paradoxically, that caring suggestion can trigger a complaint. To avoid a complaint it can be safer for the dentist, paradoxically, not to suggest such a referral and instead attempt some intervention and thereby get trapped.
Prevalence of phantom bite syndrome
There is an unknown prevalence or incidence of this condition. However, many experienced dentists will recall having seen one or more patients presenting with bizarre descriptions, or complaints allegedly being caused by ‘their bite’ or ‘their occlusion’ at some point in their practising career. They usually remember these patients clearly because those now experienced, if not actually embittered, dentists usually wish that, in retrospect, they had not got involved with such patients at all. This is because of the prolonged and time consuming nature of the subsequent multiple complaints and their various costs, worries and other complications that ensued in trying to manage them, often involving complaint managers or the GDC.
It appears, however, based on the limited literature available, that patients with PBS can present at any age, in any gender, with the condition often lasting between 10–20 years.
Clinical history
The pattern of presentation of PBS often involves patients giving a long and detailed history, often without needing to make reference to any notes, after which they tend to finish their story with something like ‘treatment xyz helped for a while, but then the problems returned’.
The history will sometimes involve a specific dental event trigger, in which an initial dentist altered their occlusion, usually with an apparently innocuous restoration, a simple extraction, or with some orthodontic appliance. However, at the end of that intervention they will say something like ‘they needed further bite treatment’, usually by someone else, to ‘fix their bite problem’. Any, or all, subsequent dental treatments do not alleviate their ‘occlusal’ or ‘bite problems’, but instead apparently exacerbate them, with the now disgruntled patients deeming the original problem-causing dentist, or the subsequent dentist(s) to be ‘incompetent’ owing to their inability to resolve their bite problems to their entire satisfaction.
Interestingly, they frequently manage to instil a belief into any new dental clinician that only he/she can correct the occlusal problems that have been erroneously managed by the previous dentist(s), often over several years. They seem to do this by praising the new dentist for their reputation for ‘occlusal knowledge’ and/or their special skills. This flattery of the new dentist's ego then leads the new dentist down the pathway of further, often more destructive, operative intervention, or unstable orthodontic treatment, in a vain attempt to try to ‘perfect their occlusion’.
Given the frequency of occlusal contact variations in the normal population, it is not difficult to find some dentist, perhaps someone with strong, or rather fundamentalist, beliefs about occlusion, or some aspect of a particular occlusal philosophy,9 who agrees with the patient that something should be done to help change things in order to get a better ‘occlusal arrangement’.
However, failure to recognize the possibility of the reported problems actually being caused by ‘phantom bite syndrome’ early on means that significant, often destructive or unstable, treatment is carried out by that new clinician in order to try to achieve the supposed benefits of this putative ‘ideal occlusion’.
Sadly for everyone involved, just before this supposedly ‘perfect bite’ is achieved, usually with different occlusal adjustments, often on already elaborate dentistry done on a sophisticated articulator, or tweaks being done to some careful orthodontic treatment, or by equilibration of the natural teeth, the patient's latest whim to ‘have the occlusion altered just slightly again’ to a newly stated ‘ideal’ is expressed.
Eventually, those ‘nearly, but not quite right’ demands produce understandable frustration in that particular dentist, or specialist, who then, rather belatedly, begins to realize that the patient's real problems lie somewhere ‘north of the maxillary occlusal plane’.
The patient then moves on to a new helpful, if initially naïve, dentist, or to a different dental specialist and adds that former dentist's name to their list about whom they can then complain (Figures 1a–d).
The real problems with these patients
The persistent perception in phantom bite syndrome patients of having ‘an abnormal bite’ almost always coincides with underlying psychiatric issues and this was originally described by Marbach1,2,3 as a mono-symptomatic hypochondriacal psychosis.
The three important hallmarks of PBS that Marbach described in a number of his publications were that it is:
Mono-symptomatic (= only one symptom ie ‘the bite’);
Hypochondriacal (= a self-diagnosed anxiety disorder that the patient has got a serious illness);
A psychosis (= a severe mental disorder in which thought and emotions are so impaired that contact is lost with external reality).
Marbach's seven diagnostic indicators for patients with PBS with the current authors' additional comments are presented in Table 1.10
Perceived dental knowledge
Intensely involved and have some knowledge of dental anatomy, physiology and dentistry. They often know bits of dental jargon, and use abbreviations or terminology regarding occlusion.Will talk endlessly about their ‘bite’ or ‘occlusal’ problems, or their ‘issues around’ the shape, colour and contour of their teeth, or various restorations and suggest how they should be changed, or altered, to correct their problems.
Keep study casts and detailed clinical records
These patients often present at the first, or at subsequent, appointments with numerous diagnostic casts that they have accumulated over the years. They will point at which parts of which cusps need adjustment to fix the problem. Diagrams, some beautifully illustrated, are sometimes presented for inspection (Figures 2 and 3).
Severe symptoms all being due to their occlusion
Complain of, or believe that, they have a serious bite or cosmetic defect. They have an ongoing and unshakeable belief that their ‘bite or occlusion’ is wrong, or that their bite looks wrong.
Sustained delusion
The delusion is sustained for many years in spite of sympathetic explanations and careful reassurance. Apart from the initial placebo effect these particular patients' symptoms are rarely improved by occlusal splint therapy, orthodontics, occlusal adjustments or ‘equilibration’, or prosthodontic interventions of different types by different dentists or various specialists.
Unwilling to accept referral to, or help from, psychiatrists
Resist the suggestion very strongly that their problem is psychiatric in origin and therefore they refuse to accept psychiatric help, or to be referred for psychiatric assessment. Patients are convinced that previous dentists have caused their problems and that further ‘bite’ or orthodontic or prosthodontic treatment, or surgical treatment, if it were just to be done correctly, would rectify all their bite and/or other issues.
Socio-economic status
High socio-economic status patients undergo extensive restoration of the occlusion indefinitely (because they can afford it).Patients of more moderate means are limited by financial constraints but still have uncontrollable impulses to have various people ‘correct their bite’, in the belief that the right occlusal therapy, or the right articulator, will solve their agony. Such dilemmas produce desperate people and they often seek multiple referrals to hospitals where treatment might be free, or they sometimes borrow money in order to have treatment of varying complexity, stability or retrievability.
IQ
These problems often occur in patients with above average intelligence and often very articulate or literate about their problems and what needs to be done.
In phantom bite cases, there are indeed sometimes detectable ‘occlusal problems’, or at least ‘suboptimal occlusal contacts’ according to some occlusal philosophy.9
However, unlike most normal patients, any dentist's attempts to improve their occlusion, or aesthetics, no matter how skilfully done, will fall short of the patients' expectations, usually at the very last meeting with that particular dentist.
Unfortunately, these patients usually refuse to be referred to a psychiatrist and often resent the suggestion that their problem is mental rather than dental if it is made by a dental clinician. If they do eventually attend a psychiatrist, it is usually reluctantly. Sometimes this is even after the perceived failure of prolonged, serious and often expensive dental interventions of different types, none of which manages to solve their underlying mental problems. Paradoxically, even if they do attend they often do not accept the psychiatrist's diagnosis, nor necessarily comply with taking any prescribed medication, or accept other types of treatment such as Cognitive Behaviour Therapy (CBT).
Instead, they wander nomadically from dentist to dentist, or to dental specialists of different types, in different locations and have different treatments done, often to their personal specification and at their insistence.
The record in this case series about PBS was in a gentleman who attended over 200 appointments with at least 20 different clinicians, many of whom were recognized specialists, in different hospitals and locations around the UK, in order for someone to ‘correct his bite’ to his personal specifications. Sadly, none of them seemed to have recognized the psychiatric condition before being lured into doing even more futile extensive dentistry or recommending it.
Presentation warning signs
Patients with phantom bite usually give a long and detailed clinical history of their problems and relate this to ‘their occlusion,’ often using dental terminology such as ‘canine guidance’, ‘slides’ or ‘occlusal interferences’. They sometimes have multiple dated study models, various images, or different occlusal devices with them. They give a definite sense of knowing exactly what needs to be done to correct their ‘occlusal disharmony’. They articulate these problems in detail verbally, with or without diagrams, and later on in multiple hand written or typed letters, or they send numerous emails to the practice, department or to the GDC.
Clinical examination in relation to the symptoms
Close dental examination will often reveal some common occlusal discrepancies, but these usually are not sufficient to justify the severity of the symptoms reported by these unfortunate patients. For instance, the teeth about which they complain are rarely mobile or tender to percussion and usually respond within normal ranges to extensive pulp testing. There are usually no compelling radiographic changes, such as widened periodontal ligaments or radiolucent periapical areas visible, even on close examination of good quality radiographs.
The teeth are of normal colour with no signs of discharging sinuses or apical tenderness. These patients will, however, insist that they have significant discomfort, general unease with their bite, or pain problems, or that they have a serious disability with their functioning elsewhere, sometimes in areas far from their mouth. Some of the descriptions of these problems can sound bizarre, eg back problems or balance problems, or postural, or eye problems, or a combination of symptoms, but wherever these problems are, they are all, according to the patient, being caused by problems of their ‘bite’ or ‘occlusion’.
One early clue that they might have PBS is that these patients are superficially knowledgeable about dentistry and occlusal terminology, often using dental jargon terms (eg ‘interferences’ or ‘slides’ or ‘group function’) to describe their problems.
The real diagnostic clues lie in taking the history very carefully, preferably in a structured way, (possibly using the questionnaire recommended in this article) with both eyes and ears being wide open and being ‘fully present’ throughout the consultation.
Range of treatments offered for PBS
The interventions by different dentists depend very much on the kind of clinician to whom they present. The treatments attempted can range from occlusal splint therapy and/or occlusal equilibration, to orthodontics of various types, through to extensive crown and bridgework or combinations of any or all of these treatments. Orthognathic surgical approaches have also been involved in some cases.
It is not unusual to find that a bewildering array of occlusal devices, of widely differing designs and used in different arches, have been used as part of diagnosis or treatment, usually by different dentists, sometimes over many years and in different geographical locations. Phantom bite patients will often have had many of these so-called ‘occlusal splints’ (which would be more accurately called ‘occlusal devices’ as they do not actually splint the occlusion) and/or studies casts and diagrams and, if requested to do so, will happily show these at consultation with any new clinician.
The plaster models are sometimes dated and carefully packaged and kept safely stored by the patient. Sometimes the ‘best study casts’ or ‘study models’, allegedly containing the key to solving their occlusal problems, are referred to almost reverently and of them being kept ‘in a safe place’.
Phantom bite patients will readily explain who took these plaster study casts and describe which devices were made for them, when and by whom they were constructed, as well their immediate, sometimes beneficial, results. However, usually, they conclude these prolonged explanations with something like ‘the benefits had only been temporary’.
A larger than usual case series (12) is presented below. These demonstrate most of the key clinical signs on presentation as well as outlining the considerable difficulties faced by many clinicians and their teams when managing these patients' various frustrating and time-consuming problems. Three clinical cases are presented in detail with a brief discussion to demonstrate the key clinical features. For reasons of brevity, other cases are summarized.
Case reports
PBS Case 1
History
Ms PBS1, a 28-year-old female, presented with a three-year history of problems which began after a crown was fitted on her lower right second molar. Over the course of the next four years she saw 11 dentists, an orthodontic specialist, two registered specialist prosthodontists and three restorative consultants in different parts of the UK.
She reported pain initially as being associated with her root-filled lower right second molar immediately after the tooth was crowned. Apparently, this was quickly ruled out as the cause of her pain and instead her partially erupted wisdom tooth was deemed to be the cause of her symptoms. Following the extraction of her lower right wisdom tooth she developed a dry socket, but also had inferior alveolar nerve damage with paraesthesia to the right side of her face.
After six months, she was prescribed Pregabalin which controlled the nerve pain, but she continued to report pain from her lower right second molar. Following a further six months of pain, she was seen on a facial pain clinic, where the diagnosis of trigeminal neuropathic pain was made, but she was ‘still 100% positive that there were issues with her bite’.
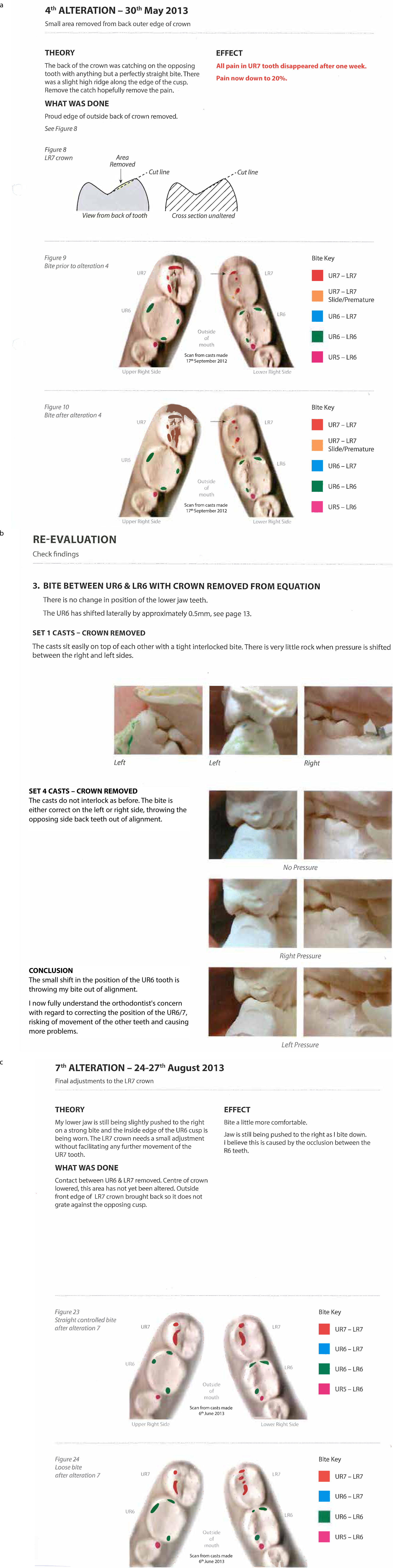
She was referred to a GDC registered specialist orthodontist who identified a premature contact on the upper right second molar and recommended it to be eliminated to correct her occlusal problems. The patient described ‘complete relief to have the diagnosis confirmed and that ‘the bite was the cause’ of her ongoing problems. Although she was advised to see her dentist to have the occlusal adjustments carried out, she decided that she had lost all trust in that dentist. Instead, she decided to carry out the occlusal adjustments at home herself. She used her technical skills in graphic design to colour code serial pictures of her posterior teeth (Figures 2–5).
She presented with a bound, beautifully illustrated, report prepared by herself. This included multiple graphic images, drawings and photographs of the things having been used by her to correct her apparently ‘disturbed bite’. She had shown this collection to the consultant orthodontist and maxillofacial surgeon, as well as four of the more recent dentists, one of whom had acceded to her request to supply her with dental articulating marking materials.
Her symptoms remained, eventually leading her to believe that her incorrect/heavy bite was causing pain that had previously been attributed to a blocked gland in her palate and to sinus infection. She then saw an ENT consultant and had her allegedly blocked gland removed, but she continued to experience pain.
She attributed her malpositioned lower right molars to her sunken appearance under her cheek bones.
After two years of self-treatment, she reported in her beautifully illustrated dental journal ‘there is nothing more that I can do. Professional help needed.’
She was offered Botox injections into her masticatory muscles by one consultant oral and maxillofacial surgeon to help to manage her chronic myofascial pain, which she declined.
She then saw a prosthodontist who recommended reversible treatment only, namely the provision of a Michigan splint. She was then referred to a restorative consultant in a different hospital who described her as ‘acutely dentally aware’ and described her in the letter to her dentist as having ‘atypical odontalgia’.
Presentation to one of the authors
Refusing to accept the diagnosis given by that particular restorative consultant, she was then referred by a different dentist to a different restorative consultant in his practice, where she attended with her bound and beautifully coloured dental journal, multiple study models and radiographs (Figures 5a–c).
Figure 5.
(a–c) Case 1: Multiple patient images with her descriptions, including study casts and her written observations on these.
Management
She was diagnosed with PBS, based on the detailed history, and the nature of the condition was discussed at length with her. She was advised that any further dental treatment could result in secondary symptoms associated with any occlusal treatment. She was told ‘that she had done a great job with her own occlusal adjustments’ and, as she was almost free from symptoms, to leave things as they were and to get on with her life as well as she could. Her father, who attended with her, seemed very relieved with the diagnosis and the proposed plan. The patient was offered onward referral for supportive ‘medical help’ but she declined this.
While she was attentive and polite during this consultation and declined the offer of a review appointment, she may well have continued to carry on her search for someone else to cure her ‘incorrect bite’.
PBS Case 2
History
Ms PBS2 presented with a history of seeing at least 20 dentists over the previous six years. This list included eight very experienced general dental practitioners, from different parts of the country, several restorative consultants, two private practice ‘occlusion’ experts, two orthodontic specialists and one orthodontic consultant.
She complained initially of a fractured lower left first molar that she reported was restored with ‘a Cerec crown’. However, once fitted, she felt that this crown was ‘undersized and had a sharp profile.’ Two months later, the opposing tooth, the upper left first molar, was also crowned, allegedly due to a crack.
Ms PBS2 then saw a second dentist who apparently informed her that the contact between the two crowns was minimal and the left lower 6 crown was then replaced with a porcelain-fused to metal crown to ‘increase the occlusal contacts’.
She then felt that the new crown was ‘too bulky bucco-palatally’ (her words), causing tongue and cheek biting, as well as ‘spacing between the occlusal aspects of these teeth’.
She subsequently saw a series of 17 generalists or dental specialists. Some of these were at the suggestion of a corporate body. Different occlusal devices were prescribed. One of those recommended dentists ‘tried to correct the occlusal problems by replacing the crowns together, in order to establish the correct occlusion’.
Her patient journey continued with another dentist who supplied her with a NTISS device (Nociceptive Trigeminal Inhibition Suppression System) and she was told that her problems were now definitely related to her temporo-mandibular joints. However, after a period of use, she felt that ‘this device only worsened her open bite’ which, considering the design of this, was not surprising.
The patient subsequently developed ‘a unilateral posterior open bite’ (her words) and she described herself as ‘having a slide with a movement to the left after the initial contact’ which she felt significantly affected her speech and overall function.
One of the dentists and one of the consultants who assessed this lady felt that ‘they could not treat her condition because it was not within their area of expertise’. This angered her a lot and enhanced her belief that ‘the whole of the dental profession was incompetent’.
She reported that several hours of her days were spent researching on the internet for various treatment options to correct her bite. Given her research background, which included her having a PhD, she was adamant that there was a treatment ‘out there that she had not found yet’ that could cure her bite problems and ‘she was willing to try everything and anything to get the right bite’.
After several more consultations with various dental professionals, and the use of different occlusal devices, she saw one restorative consultant in his private practice, who offered a non-destructive approach using direct resin composite to build-up her teeth that were not in contact due to trying to stabilize her occlusion. However, the patient felt that ‘the bite was fundamentally incorrect’ and did not want more teeth to be built-up into this wrong position, and therefore that treatment option was rejected, apparently quite angrily, by her.
Further searches on the internet and further consultations ensued with different dental laboratories, using computer scanning modelling. On that basis, she had two crowns replaced and temporarily cemented for her ‘to assess the changes in her bite’, which she did using a microscope that she had bought and used to do this at her home on a very regular basis.
Presentation to one of the authors
She was referred by a dentist, who worked for a corporate body, apparently as a result of the multiple complaints that had been received. She presented with several dated study models, carefully kept in dental model boxes and also with a series of pantographic style tracings that had been carried out in various practices over the years. She also had results of ‘TMJ joint vibration analysis’ that had been done previously, along with multiple periapical and panoramic radiographs.
Her clinical examination revealed no occlusal contacts being present from the upper left second premolar all the way around to the upper right first premolar. However, the pre-treatment study casts showed very clearly that there had been even occlusal contacts on all of the teeth prior to the various bits of dental treatment.
Management
The diagnosis of ‘phantom bite’ was made, explained and discussed at length. Ms PBS2 was informed that the occlusion had indeed changed considerably since the first crown had been placed, as judged from her original study casts. The patient was told that her bite would probably never return to the original asymptomatic one, which was something that the patient found very difficult to acknowledge as being the case or to accept that expressed view.
It was explained, very gently, that the problem was not mainly dental and that the reason for this change in the occlusion was due, in part at least, to the patient's insistence on seeing various dentists and having more and more complex dental treatment at her specific request. As expected, this diagnosis was rejected by the patient and her partner immediately. An offer to refer her on to an appropriate specialist psychiatrist for diagnosis and treatment and help was also rejected immediately. Further time consuming explanations over some hours proved futile.
Subsequent to this consultation some further serious harassment by the patient ensued. This unpleasant harassment of various people and of the clinician who diagnosed phantom bite only stopped following a legal injunction to prevent it continuing. The outcome therefore remains unknown to these authors.
PBS Case 3
History
Mr PBS3, a 29-year-old male patient complained that his bite was causing him severe neck and shoulder problems. He was adamant that this was a direct result of an occlusal filling that had been placed in his upper right first molar two years prior to him being seen at one hospital.
He reported that he had had a ‘change in the enamel after a filling in the upper right six’ and that then his ‘bite felt wrong.’
He believed that his teeth were ‘locked in’ and that his ‘jaw pulled to the right causing postural problems.’ On several occasions, he referred to the impact of his dental problems on his daily life and functions and that ‘this filling had ruined his life’ because his ‘group function was no longer the same.’
He also felt that his ‘shim stock holds’ had changed over the previous two years. During this time period, he had seen eight general dental practitioners and, from the history, which he repeated at length to various clinicians, secretaries, receptionists, or to anyone else who would listen to him, he had had numerous discussions with these dentists over the telephone, as well as going to see them in their practices.
His treatment ranged from replacement of the filling to ‘adjustment of his opposing tooth to correct the bite’. However, the patient felt that his bite was never quite right again.
He subsequently saw five different restorative consultants in three separate London hospitals.
He had an MRI scan as well as a cone-beam CT scan done of his temporo-mandibular joints ‘to assess these for any pathology’. All of the special investigations that were carried out were negative.
Mr PBS3 reported he had been researching his condition on the internet and felt that he ‘probably needed TMJ surgery to fix his problem’.
Clinical presentation to the authors
Examination revealed bilateral masseteric tenderness on palpation and left temporalis tenderness. There were no obvious abnormalities detected in his occlusion, with no evidence of non-working side interferences or of premature contacts.
Diagnosis and management
The diagnoses of PBS and possible TMD (myofascial pain) were made. A hard maxillary Michigan style occlusal splint was constructed for him to wear to manage his TMD symptoms and apparently his pain improved for a short period of time. However, he still remained focused and very concerned ‘about his occlusal problems’. The patient reported that he had very little sleep at night because his occlusion was worsening and he frequently attended or called reception, demanding to be seen urgently to ‘correct the occlusion problems’ and to get his study models.
His pattern was to go to different practices and restorative departments without any appointments and to spend hours telling any clinician, nurse or secretary who would listen to him about ‘his bite’, using dental terminology such as ‘group function’, ‘occlusal interferences’, ‘slides’ and ‘shim stock holds’.
Despite his numerous complaints about his occlusion, further clinical examination by different specialists and generalists revealed no significant abnormalities in his occlusion. He had been advised early on by one consultant that he had ‘phantom bite syndrome’. It was suggested to him at the time of the phantom bite diagnosis that he should cease his search for further expert opinions about his occlusal problems and that he should get his doctor to get him support and medication from the psychiatric department of an appropriate hospital. He objected strongly to this advice and, predictably enough, he sought advice from other dental consultants in different hospitals.
Mr PBS3 frequently became extremely aggressive and confrontational within different hospital restorative departments, often returning to different hospitals without an appointment, demanding to see whichever restorative consultant was available and sometimes demanding that he be given ‘his study models that would fix his occlusal issues’.
He also attended one consultant's home twice, both times unannounced on a Friday night, proffering some study models and repeating his history in detail in the hall to the consultant's wife, as well as demanding that occlusal adjustment should be done there and then. He was ‘strongly advised’ not to visit that consultant's home ever again, with the threat of obtaining a legal injunction.
On different occasions he was escorted by the police from at least one general dental practice after demanding ‘more occlusal treatment’. He was physically carried out from a different hospital's restorative department by their hospital security after showing up demanding ‘treatment for his bite’. His attendance patterns became more disruptive to various different hospital departments and dental practices.
After prolonged discussions with two more restorative consultants in a third hospital, the patient eventually accepted referral for a psychiatric evaluation, but that was something that he was extremely bitter about.
After various psychiatric evaluations, his GMP prescribed Resperidone and Olanzapine. These well-known anti-psychotic drugs are often used separately, or in combination, to treat schizophrenia and bipolar disorder. Predictably enough, he discontinued the medication after 4 days because he felt that he could not tolerate them. He also stopped seeing the psychiatrist after three sessions ‘because he felt it was not worth his time’.
He became increasingly antagonistic towards the restorative consultant who had made the original phantom bite diagnosis at his first appointment with him and who had forecast the likely problems that would happen. In spite of being treated courteously, over very many hours, by various consultants, in different hospitals and by various general dentists in their practices, he then pursued multiple time consuming formal complaints, with the help of an advocate, all the way to the Ombudsman.
Eventually, after multiple unpleasant incidents, restraining orders were taken out against the patient by at least two hospitals.
Prognosis
The prognosis is poor. Patients usually continue to seek different dental treatment from someone new and may eventually progress to surgical options to correct their perceived occlusal disharmonies.
Orthodontics followed by jaw surgery will, if undertaken, only bring more disappointment to both the patient and the orthognathic11 team and the patient will probably prove to be unhappy with that outcome too.
In summary, the amount of time spent by multiple general dental practitioners, restorative consultants and/or others in attempting to manage the unrealistic goals of these patients with dental procedures can be not only extremely time consuming and wasteful of valuable and scarce resources, but also prove to be frustrating and futile, while also being likely to lead to exhausting complaint procedures of various types.
Summary of other cases
Case 4
Complained of her ‘bite being too heavy at the front’ and this caused her postural problems and vision disturbances. Saw a GDP multiple times, two restorative consultants and an oral maxillofacial surgeon for consultation. Treatment involved splint therapy, full mouth rehabilitation, occlusal equilibration and then further splint therapy followed by rehabilitation as ‘the bite was not quite right’. She had an MRI of the TMJs done. No treatment resolved her bite symptoms. Clinical examinations revealed many different occlusal positions, with her currently preferred posturing one being very strange indeed. She attempted suicide 3 days after being told that she had phantom bite syndrome, which was her third attempt at committing suicide and which resulted in her being sectioned. Apparently she recovered from that acute episode of depression. Overall, it was estimated that she attended over at least 90 appointments with various clinicians.
Case 5
Presented complaining of ‘trigeminal neuralgia’ (patient's own words) which ‘caused his whole body to pull to the right’. He felt sure that ‘correcting his bite would re-align his body and improve his quality of life’. He reported that the symptoms began after a wisdom tooth extraction under local anaesthetic. He was seen by his GDP, a specialist prosthodontist, a number of restorative consultants and an oral and maxillofacial surgery consultant. His treatment included splint therapy, occlusal equilibration, multiple root canal treatments, re-root canal treatment, and extractions under local anaesthetic following ‘failed’ root canal treatment. Special investigations including a cone beam CT scan and MRI of the TMJ, all of which had negative findings. He was seen for over 50 appointments with no resolution of his symptoms. Clinical examination revealed nothing particularly untoward about his occlusion. The patient was eventually informed of the diagnosis being of phantom bite, which he refused to accept or to be referred for psychiatric evaluation.
Case 6
A 67-year-old patient presented with ‘jaw juddering attacks’ lasting 2–3 minutes once a week which caused her bite problems. She reported her tongue getting trapped at night due to her bite disturbance. She had seen her GDP and two other restorative consultants, as well as five junior members of staff over multiple appointments before being diagnosed with phantom bite syndrome. She wrote 25 letters to one of the authors repeating that all her various problems in her back, neck, knees and shoulders were all caused by her ‘bite juddering’. She refused any psychiatric input, or even to try a Michigan splint to see if her symptoms would improve, because her friend had told her that she needed ‘full bite correction’ to cure her. Her oral hygiene was dreadful in spite of multiple demonstrations of oral hygiene techniques. She refused any treatment that was not going to involve full bite rehabilitation because ‘her friend had read on the internet that her problem could only be dealt with properly with full mouth rehabilitation’.
Multiple formal complaints ensued.
Case 7
Patient presented complaining of ‘bite problems which started after 3 crowns were placed in the lower left quadrant’. She reported nasal problems, headaches and sinusitis, along with clicking jaw, neck and shoulder pain, blurred vision and vomiting, all of which, apparently, had been caused by her crowns having been placed incorrectly. Overall, she was seen by 6 general dental practitioners, 1 oral and maxillofacial surgery consultant, 3 consultant rheumatologists, 2 physiotherapists, 2 private dentists, 1 ENT surgeon, 7 general medical practitioners, 1 ophthalmologist, 1 specialist dentist and 1 restorative consultant. During this time, over £10,000 was spent to attempt to ‘correct her bite problems’. She underwent 3 crown replacements, adjustments of the crowns, root canal treatment, occlusal equilibration, 3 MRI scans, 1 facial CT scan and 1 TMJ arthroscopy. All of her dental and head and neck investigations were unsuccessful in managing her symptoms. She said that she was feeling suicidal but refused to accept the diagnosis of phantom bite or to be referred for urgent psychiatric help.
Case 8
Patient had multiple crowns placed in a general dental practice. She then had a full mouth rehabilitation done by a consultant in a teaching hospital which was followed by a Michigan splint. Apparently, she had had about 100 appointments for various crowns to be replaced and for occlusal adjustments to be done over a 5-year period. She then had another full rehabilitation done but using metal and composite on the occlusal aspects for ‘ease of bite adjustment’. Eventually she made a formal complaint because, although she was relatively free of symptoms at that stage, apparently the consultant in charge at that time did not want to change these crowns for ‘new permanent crowns with the correct bite to finish her case’.
Case 9
Patient attended her GDP for 2 crowns and 3 veneers. When she complained after these were fitted she was referred to another dentist for ‘problems with the bite’ and fees were refunded. The crowns and veneers were replaced but things got no better. Fees were refunded. She was referred to a maxillofacial department and subsequently then saw 3 more dentists ‘to replace the replacements’ along with fitting of ‘a brace’ to reposition her bite. The patient attended one of the authors with a box full of models and a big red folder with about 50 pages of letters with dates and the names of different dentists and what they had done, along with copious notes about what ‘needed to be done to correct her bite problems’.
The box of models that she had with her was carefully presented. This box contained the original cast, the original cast with a denture, a diagnostic wax-up, a putty index of the diagnostic wax-up, one master cast of the preparations for one remake, as well as an uncut copy of a second cast with the re-prepared, now minimal remaining cores.
The patient was on Amitriptyline and Zopiclone, which apparently had helped a little.
An explanation was given about phantom bite syndrome and the patient was advised not to have further replacement dentistry. An offer to get her doctor to refer her for specialist psychiatric input was somewhat reluctantly accepted and the patient was then referred back to her doctor, with details of the phantom bite condition, for onward referral.
Case 10
Patient attended with multiple medical problems including cardiac and central nervous system (CNS) problems as well as several autoimmune conditions, including Hashimoto's thyroiditis and systemic lupus erythematosus. She had multiple allergies and was taking various medications. She blamed her CNS and heart problems on the extensive dental rehabilitation work which she had done in 2007.
She had seen multiple GDC registered specialist endodontists for very competent endodontic treatment after this prosthodontic treatment, as well as having had multiple CT scans.
She had had a number of extensive oral rehabilitations done which apparently ‘helped for a while but then the symptoms returned’. She had seen various other experts in various fields, including two pain specialists.
Examination showed extensive high quality restorations, including an implant following some bone grafting and many root-filled teeth without periapical areas. Soft tissues and TMJ examinations revealed no abnormalities and a diagnosis of phantom bite syndrome was made. This was explained to her in detail and the patient was offered onward referral for psychiatric input, but this was declined.
Case 11
The patient had some wisdom teeth removed and then had a maxillary hard occlusal device made which produced a ‘relatively comfortable bite for 17 years’. ‘She had a filling done which precipitated problems’. This included ‘trigeminal neuralgia in her face’, which she referred to as ‘TN’ throughout the consultation as well as ‘pain in her temporomandibular joints’. She then had occlusal adjustments, root fillings, multiple re-root fillings and an extraction of the previously re-root filled lower second molar. She had multiple copies of radiographs with her and various study casts. She had seen quite a number of ‘occlusion experts’, one of whom made her a Tanner device with multiple adjustments being done to this. She felt strongly that ‘if only she could have her bite built back up again then her whole body alignment would improve’. A consultant maxillofacial surgeon and a specialist radiologist concluded after multiple examinations that there was no jaw joint pathology present. A number of other well-known academics had seen her in various UK cities, as well as some pain experts.
She had with her a Lucia jig, a NTISS device, a Tanner device, as well as a couple of Michigan type splints. These had helped for a while but none as much as the first hard upper splint had done.
A diagnosis of phantom bite syndrome was made and gently explained in detail over a couple of hours, with her reiterating her convictions about ‘her problems all being caused by her occlusion’. An offer of referral for expert psychiatric help was refused.
Case 12
The patient presented having had a number of major occlusal rehabilitations carried out. She had had multiple extended veneers and all-ceramic crowns done, followed by remakes of these, many subsequent root fillings and re-root fillings and eventually extractions. She had two implants after two of the re-root filled teeth were extracted.
There were root fillings present in two of the lower incisors, as well as in the lower left second premolar, lower left first molar, upper left second molar, the lower right first premolar, lower right first molar and lower right second molar.
She had got mainly all-ceramic crowns present on her teeth, including two on the implants. She was still unhappy with her bite, in spite of having worn Tanner devices and maxillary hard occlusal splints before, during and after her extensive ceramic-based reconstructions (Figure 6). She was strongly advised against further speculative dental interventions in view of the probability of phantom bite syndrome being the root cause of her ongoing problems.
Figure 6. A DPT of a patient who had extensive dental treatment done on previously intact teeth by different dentists, over long periods, with the apparent aim to ‘correct the bite and to get a perfect smile’.
Discussion
Phantom bite syndrome (also now known sometimes as occlusal dysaesthesia, or as occlusal dysesthesia, which is the American spelling) is usually described as being a rare condition. However, based on various conversations with some older dentists, there will be at least some readers of this article who will remember having seen, or tried to treat, one or more patients who roughly match the description of this problem. The cases described above report the lengths some of these patients will go to in order to get someone to correct their perceived bite issues or ‘problems with their occlusion’ or bite.
One major paradox of this condition is that these sorts of patients are unwilling to accept that they have got phantom bite syndrome (PBS) (or occlusal dysaesthesia/dysesthesia) and usually deny even the possibility of that diagnosis being correct, or of them needing any psychiatric help. However, their previous and their subsequent behaviour, which can include persistent and vindictive complaints, usually confirm the phantom bite diagnosis as being correct.
For instance in PBS2, as described above, in an average patient with a ‘dentistogenically’ induced unilateral posterior open bite, a direct bonding technique using composite could probably be utilized to try to address the functional issues and hopefully ‘stabilize the occlusion’. However, in cases of PBS, unfortunately, this treatment approach would not be at all predictable because these patients are always trying to find their elusive ‘final comfortable bite’. As this preferred ideal position for ‘their bite’ varies enormously, sometimes in very weird ways, with the preferred jaw positions demonstrated being far away from any recognizable or traditional reproducible position, that is probably not going to be realistically achievable by any dental professional in any predictable way.
The root of the problem is mental illness and not dental disease.
The ‘dental’ management of these patients should probably therefore be limited to patient information and sympathetic discussion about the difficulties of the condition, as well as an offer of onward referral for psychiatric input.
The structured phantom bite questionnaire (see below) should be completed by patients in their own time, at their home, and this will provide a suitable record as well as helping to alert the clinician early on about the probable real problems and hopefully enable the clinician to refer appropriately.
The Diagnostic and Statistical Manual (DSM) Classification of Mental Disorders of the American Psychiatric Association (APA)
Phantom bite was originally described by Marbach in 19762as a mono-symptomatic hypochondriacal syndrome, a term which has since been deprecated by subsequent iterations of the American Psychiatric Association (APA) Classification of Mental Disorders.
In terms of APA classification, previous versions of ‘Phantom Bite Syndrome’ (PBS) would probably have been categorized under ‘Medically Unexplained Symptoms’ (MUS), or as a ‘Somatoform Disorder’ in their fourth Diagnostic and Statistical Manual of Mental Disorders (DSM–IV–TR 2000).7
In the 2013 DSM V classification, it would probably now come under ‘Somatic Symptom Disorder’,8 which is abbreviated to SSD. Characteristics of SSD are somatic symptoms that are very distressing to a patient and/or that result in significant disruption of functioning, as well as excessive and disproportionate thoughts, feelings and behaviours regarding those symptoms. To be diagnosed with SSD, the individual must be persistently symptomatic, which typically means for at least 6 months.
Once the diagnosis is confirmed by a specialist psychiatrist, preferably one who is familiar with these sorts of problems, then selective serotonin re-uptake inhibitors (SSRIs) or other appropriate antidepressant or other drugs and/or cognitive behavioural therapy, or some combination of these treatments can be prescribed as appropriate. If the treatment suggested is accepted by patients, this probably represents their best chance of a possible solution to their longstanding problems, as opposed to someone continuing to provide speculative, unpredictable, irreversible, biologically expensive dental treatment to ‘improve or correct the bite’, which often seems, based on this selection of 12 cases but also on others, to have been futile and to have been undertaken, at least partly, at the repetitive insistence of the patient.
Some patients with ‘Phantom Bite Syndrome’ or a ‘Somatoform Symptom Disorder’ may have overlapping features similar to those with body dysmorphic disorder (BDD), a term applied to those individuals with a normal appearance who present requesting treatment because they believe that they have a ‘defect’.11
Costs of treatment for phantom bite syndrome
Patients with this condition seem to be of above average intelligence and often highly articulate and literate. Some can afford to have extensive private treatment and detailed investigations in an effort to satisfy their perceived needs for their bite or ‘occlusion’ to be treated.
Patients from different social groups can become a repetitive burden on different NHS hospital departments and regularly move to different ones if they can, particularly if they are frustrated in their quest for their ‘bite’ or ‘occlusal’ desired treatment being denied to them by one clinician, department or hospital.
Phantom bite patients often intersperse their hospital visits with an unknown number of contacts with general dental practitioners (GDPs). Unless that GDP contacts the appropriate clinician or hospital(s), there may well be no real knowledge of the overall number of these patient visits. An estimate of the three most ‘frequent flyers’ in this series is that they each had well over a 100 visits to various clinicians in different locations. This conservative estimate does not include the costs of the time involved with dealing with their time consuming telephone calls and/or letters to secretaries and reception desks, often followed by complaints to different people and organizations.
As a result of the different and often extensive dental treatments, these patients become educated in dental terminology and various ‘dental occlusion philosophies’.9 They then often use this new found knowledge to persuade any new, and usually initially sympathetic, clinician to undertake the next course of speculative treatment based on one or other of these mutually contradictory occlusal treatment philosophies.9 Given the benefits of the detailed history and enough experience of the condition, coupled with the 20:20 vision of hindsight, at least some of this might be considered to be inappropriate treatment.
Different explanations for phantom bite have been proposed. Klineberg suggested that occlusal hyper-awareness could be the cause of the condition.12 He suggested that a lack of adaptability to occlusal changes resulted in the condition.
In 1985, Marbach13 considered the psycho-social factors involved in why these patients fail to adapt to dental treatment. He found that many of the complaints were incurable. Interestingly, he found that they were also not terminal with regards to the dentition. These patients are chronic sufferers, with their ongoing dentistry becoming an illness maintenance system. He warned that ‘prolonged dental intervention and palliation can result in the emergence of symptoms secondary to treatment’. These secondary symptoms, or side-effects, are sometimes more destructive than the disease the treatment was intended to palliate.
Root fillings following elective extensive ceramic crown preparations, which are sometimes done to achieve the desired occlusal contacts, are not uncommon. This is often because the pulps in the previously intact teeth get no warning of the unprovoked air rotor attack opening millions of their previously healthy dentinal tubules. This physical assault is often followed by a period of microleakage due to poor temporization of the cut teeth, thereby allowing easy bacterial ingress down the freshly opened tubules directly to the pulp, especially near the pulp horns or gingival margins.14 The resultant pulpitic symptoms can then lead to pain of variable severity and difficulty of interpretation, and eventually to root fillings through the extensive restorations with unpredictable outcomes. If there are further ongoing complaints, then eventually extractions of the previously intact teeth are done, sometimes followed by implant-retained restorations.
Dental treatment in cases of phantom bite syndrome almost always promotes the illness, as opposed to curing it. In a delusional condition such as this, patients' seemingly unshakeable belief about the cause of their dental problems will not be overcome by replacing a filling, a crown or bridge with fastidious detail to occlusal contacts, nor by altering the occlusal contour of the restorations, nor by even more extensive occlusal treatments. However, that does not stop some dentists sharing in the delusion that it will do so, particularly if adequate fees are available, and/or when the patient initially flatters the dentist with compliments about the dentist's reputation for greater occlusal knowledge and occlusal expertise. In some ways, this could be described as a version of the ‘folie a deux’, with both the patient and the dentist being deluded, at the beginning of their relationship at least. Sadly, this ‘mutual adoration’ relationship only lasts until the patient declares the dentist's treatment a failure and then goes to someone else to try to solve their ongoing problems, or complains to some supposed higher ‘authority’ or to some allegedly unbiased regulator – neither of whom know anything much about these difficult problems – often leaving a clinician to puzzle about how, or why, things went so badly wrong.
Describing these patients as having ‘obsessive compulsive tendencies’ is understandable, but possibly inaccurate in purely psychiatric terms, as patients with true obsessive-compulsive-disorders are usually defined as having ‘an unwanted intrusive thought, doubt, image or urge that repeatedly enters the mind. The person usually regards the intrusion as unreasonable or excessive and tries to resist them’. In other words, they have some insight into their problems. In phantom bite syndrome cases, patients are usually oblivious about their delusion and they lack insight into their condition. Indeed, as Marbach observed originally, if they developed insight into it, it would cease to be a psychotic delusion and therefore would not be included in that category of mental disorders.
Jagger and Korszun, in an article reviewing three cases, noted that phantom bite was a rare and difficult to treat disabling condition, which could not be cured by occlusal treatments and irreversible occlusal treatments and therefore that these should be avoided.15 Instead, they recommended that, if possible, patients be referred for psychiatric diagnosis and help. They deemed the prognosis to be poor for symptom elimination, but not necessarily for patients' overall functioning and well-being. In their view, further research into the condition was required but, in the meantime, it was suggested that emphasis should be placed on patients building their adaptive coping skills.
In 2007, Reeves and Merrill16 described an apparently similar condition to ‘Phantom Bite Syndrome’ as being one they termed ‘Occlusal Dysesthesia’ and stated that it was a somatoform disorder that should be described under the psychiatrists’ Diagnostic and Statistical Manual IV (DSM IV, 2000). They suggested cognitive behavioural therapy should be undertaken by the appropriate specialists. They described occlusal dysesthesia as having the following characteristics:
The patient's complaints are often of long standing and reported to have occurred as a consequence of procedures ranging from simple fillings through to extensive restorations, orthodontics or oral surgery.
Reassurance by the dentist does not reduce patient's concerns or distress.
Being referred to a ‘TMJ expert’ or ‘Occlusion’ expert increases patients' somatic preoccupation and reinforces their erroneous conviction that they have a serious illness as a result of their occlusion.
An occlusal dysesthesia patient often misinterprets the reason for the referral. They believe that the dentist believes that the problem is very serious and is merely asking the ‘expert’ to confirm this.
Patients misinterpret their physical sensations regarding their occlusion as well as other health-related communications.
The patient's perception of occlusal abnormalities persists in spite of multiple attempts to adjust the patient's occlusion.
No dental or pharmaceutical treatment has been effective in eliminating the unhappiness about the ‘bite’ or ‘occlusion’. Occlusal splints, occlusal adjustments, orthodontics, oral surgery or orthognathic surgery of various other types do not solve patients' perceptions of their problem.
Repeated failures merely reinforce patients' convictions that there is a serious illness and that this is all due to their occlusion.
They persist in seeking multiple opinions and make unreasonable demands for their occlusal ‘problems’ to be sorted out, often presenting with monologues detailing their current problems and past treatment failure(s).
They are usually dissatisfied and often angry with all their various dentists' previous failures which did not resolve the occlusal problems as they perceive them.
They become litigious against the dentist(s) who they perceive as having caused them harm.
This description sounds a lot like the much earlier named ‘Phantom Bite Syndrome’.
Psychiatric issues of phantom bite/occusal dysesthesia. Somatic symptom disorders (which were previously classified as somatoform disorders)
These are characterized by symptoms affecting different parts of the body, usually beginning at age 30 and extending over many years.8 The incidence of patients presenting in general medical practice with somatization has been put at just under 9%, with three-quarters of those reported to be women.7
‘Somatization’ involves the patient presenting with symptoms whose cause cannot be identified and it is often associated with stress, anxiety or other psychological factors.
Typical complaints include double vision, fainting, abdominal pain, bowel problems or extremely painful menstruation. These complaints are often presented in a dramatic and exaggerated manner. The patient may visit many healthcare providers, sometimes several simultaneously, and undergo numerous diagnostic procedures, unnecessary treatments and even surgery.
Most of these patients are anxious and/or depressed and many have difficulty in their personal relationships. They are rarely completely free of symptoms, in spite of frequent medical attention. The repeated, unnecessary diagnostic procedures or surgery can add to their real suffering. Depression has been found to be highly correlated with somatoform disorders. Versions of these conditions are well recognized in different medical circles, with one version, described by Briquet as long ago as 1859, being termed ‘Briquet's syndrome’.
In summary, ‘phantom bite syndrome’/occlusal dysaesthesia (‘dysesthesia’) probably meets most of the criteria for a somatic symptom disorder, or of a somatoform disorder. In this instance, it usually presents with excessive preoccupation with recurring complaints which, in patients' persistent view, is being caused by their bite or occlusion being incorrect.
Reeves and Merrill noted that such patients indulge in ‘dentist shopping’ for occlusal treatment and this search for a bite solution is of such long duration and intensity that this impairs their normal social and occupational life.16 Such searches for a dental solution incur expenses estimated at more than six times the average. That figure excludes the amount of income that they lose due to lost work when seeking or having treatment.
However, as this is a mental health issue rather than a dental health issue, until the somatoform disorder is addressed with some combination of medical, behavioural or pharmaceutical treatments, virtually all types of dental treatments, even sophisticated occlusal ones, are very likely to fail.
Specialist orthodontists' familiarity with phantom bite syndrome
In 2011, Ligas et al17 carried out a survey of 4,000 orthodontists in America. Only 337 completed the survey and only 50% of this group were familiar with the term ‘phantom bite’. However, many reported seeing patients with ‘phantom bite’ types of complaints. It would appear that the awareness amongst this group of this phantom bite phenomenon, or of its various versions, such as occlusal dysesthesia, needs to be raised in order to detect these patients early on, thereby preventing unnecessary treatment of a condition that will not resolve with orthodontic or elaborate, often irreversible, subsequent dental treatment.
Warning signs of phantom bite or occlusal dysaesthesia being the possible diagnosis
Patients reporting severe problems ‘caused by their bite’ or using the term ‘occlusal problems’ that do not make much dental sense but yet seem to be overly disabling to the patient.
Patient showing hugely increased focus on some aspect of ‘their bite’ which is way in excess of what would normally be expected.
Patient giving a very detailed history of many previous ‘occlusal’ or ‘bite’ problems and treatments including the failures of traditional conservative occlusal treatments, eg Michigan splints or Tanner devices.
Patients expressing anger about previous dentists' failures ‘to get their bite right’ or of having had dental treatment, which looks reasonably satisfactory, but is nonetheless getting blamed by the patient for all their problems, often in remoter parts of their body.
Patients who are overly praising about your reputation for knowledge about occlusion, or overly ingratiating or manipulative, about your great clinical skills, in the hope of them getting treatment from you for their ‘bite’ problems.
In this context, there are many dentists with strong views about occlusion. The dental literature is replete with descriptions of various occlusal philosophies purporting to be the correct one.9 Many orthodontists worship Edward Angle's classification as being vitally important and many strive to produce Angle Class 1 occlusions where possible. Some prosthodontists are fans of mutually protected occlusion, while others prefer canine guided occlusion, or unilateral group function. Makers of complete dentures aspire to provide ‘bilaterally balanced occlusion’.
However, a more rational approach involves recognizing that dental occlusion changes as a result of the time of day, conscious jaw posturing and muscle tension.
Premature contacts are common in most patients and these are generally tolerated. Some problems, eg temporomandibular dysfunction, which have often been attributed to occlusal discrepancies, are now viewed as being multi-factorial with stress, anxiety, depression and gender being important risk factors, but these usually resolve themselves without aggressive dental adjustment in the majority of cases.
Can the paradoxes be resolved?
Not predictably, sadly. Phantom bite syndrome or occlusal dysaesthesia has a protracted and poor prognosis. Dentistry in its various guises is very unlikely to cure patients' perceived occlusal problems in a predictable way, but it can do irreversible damage, and it is therefore important to try to detect the condition early on, in order to prevent inappropriate and/or dentally destructive, or unstable, over-treatment of these very difficult, trying and challenging patients.
A structured history should be taken and a detailed summary should be made, preferably using the patient's own sentences, phrases and terms to report their main complaints. Sadly, the national health remuneration system does not encourage clinicians to do this nor does it allow adequate time for these time consuming tasks to be undertaken thoroughly.
A questionnaire has been developed for patients to complete in their own time and in private which should help to alert clinicians to the possibility of the patient having this condition and save them surgery time trying to work out what is probably going on. A copy of this is available to be downloaded FREE from info@martinkelleher.co.uk
Early referral, preferably to a psychiatrist, if they will attend, or at least to a dental hospital for sympathetic explanations is probably a sensible first step. However, many of these patients do not generally accept psychiatric support or medication and, paradoxically, some complain very strongly if this is suggested, even gently, to them.
Drugs used for phantom bite
The use of the drug Pimozide was suggested in the original Marbach report (1978) but it is lacking scientific support.2
A very small study in Japan18 described a case series of treating phantom bite with the serotonin re-uptake inhibitor Milnacipran for four weeks. The paper showed 5 out of the 6 patients taking the medication reported a significant improvement, with a visual analogue scale improvement in their occlusal discomfort in half of them. It was reported that the improvement was independent of the anti-depressant effect. It was suggested that Milnacipran might be helpful in managing this condition, but the authors stressed that further long-term studies should be carried out.12
A 2015 a Japanese study of 130 patients reported on the incidence of psychiatric co-morbidities, as well as the psychopharmacological outcomes of treatment of PBS. There were four times more women than men in the study, with a mean age of 53 +/- 13 years They stated that only about one fifth of these patients had had severe psychiatric co-morbidities, such as schizophrenia, bipolar disorder or major depressive disorder. Forty patients (31%) showed good improvement with Mirtazapine, Amitryptilene or Aripiprazole.19
A 2015 review of the literature about occlusal dysesthesia by Melis and Zawawi found 18 articles which they considered to be relevant to the condition, including aetiology, diagnosis, classification and treatment. Their main conclusion was that irreversible dental treatment should be avoided because it usually worsened the condition.20
Medico-legal implications
When phantom bite syndrome patients complain, or make a claim, the fair placement of appropriate blame, or responsibility, is often extremely difficult. In those cases where irreversible treatment has been done, which turns out not to have solved the patient's complaint, dentists should not be judged too harshly after the event by some probably previously poorly informed ‘authority’.
The truth is that there are often many complex factors involved, including the insistent patient demanding treatment and a dentist or specialist failing to recognize this rare condition early on. Many pious people have great wisdom, especially with the 20:20 benefit of hindsight. Patients and dentists are involved in varying proportions for these unhappy outcomes, including their biologic and financial consequences. In truth, many patients are at least as culpable as dentists in causing their own ongoing problems and costs.
Allegedly omniscient lawyers or regulators, most of whom have never met, or bothered to meet, any such difficult patients, because the condition is rare, can claim that the condition should have been recognized and dealt with better, but only with the benefits of seeing things after the event through their well-polished retrospectoscopes.
The harsh blame culture increasingly prevalent in modern society can mean that allegations can be made that the dentists who carried out extensive invasive treatment in these patients should carry all the blame for the ongoing problems or progression of the ‘Phantom Bite Syndrome’. That is spurious because most of these patients have demanded further extensive treatment. However, these claims can be difficult to defend, particularly if any obvious warning signs were repeatedly ignored, and it is alleged that some or all of the treatment done was inappropriate and/or undertaken largely for financial gain. That said, the high degree of intelligence of some of these patients, coupled with their ability to articulate their problems in a manipulative way in order to get clinicians, of different types or specialties, to treat them, means that they often become the real driving force in what attempts are made to try to correct their perceived ‘bite’ problems. Treating their perceived occlusal issues with mechanical dentistry means that the underlying psychiatric issues remain. However, because these patients lack insight, even after the failure of often elaborate dentistry, they often refuse psychiatric referral, because their firm belief remains that their problems really are purely dental and not mental.
Another paradox is that there does not seem to be much awareness of this specific phantom bite syndrome condition in the psychiatric or dental literature. Furthermore, even if patients do attend for psychiatric help, there is paradoxically little compelling scientific evidence of there being a swift or predictable cure by psychiatric intervention, pharmaceutical therapy, cognitive behavioural therapy (CBT) or any combination of these.
It appears that psychiatric treatment goals should be focused on re-directing beliefs away from ‘correcting the bite’ and towards coping with their current occlusion and how to focus on other aspects of their daily life. This approach can help reduce their fixation about ‘fixing’ their bite or their ‘occlusion’ or their other issues which they attribute to the problems caused by their allegedly problematic bite.
If, however, such patients do not get what they want done, they often become serial complainers to various patient advice and liaison offices, practice managers, practice owners, corporate bodies, or to regulatory authorities of various sorts.4 They can often easily manipulate the people handling the complaints early on that their previous dentists were incompetent, uncaring, ‘rude’ or negligent. Such complaints can result in even more time consuming quasi-judicial or disciplinary procedures, until eventually even those apparently omniscient complaint managers or regulators grow weary. They sometimes then accept what the clinician eventually making the diagnosis of ‘Phantom Bite Syndrome’ had told them early on about this unfortunate condition in these often extremely challenging patients.
Conclusions
Possible phantom bite syndrome patients should be identified early on if possible and managed very carefully as they do not respond at all well to dental treatment, no matter how skilfully this is performed.
Phantom bite patients are highly resistant to being referred to psychiatrists as they lack insight into their condition or behaviours and they usually remain resolutely convinced that if they could only get someone competent enough to get their ‘bite right’ then all their symptoms and problems would be solved.
Dental practitioners, or other specialists, who suspect that they might be dealing with such a problem should get such patients to complete a phantom bite questionnaire. One questionnaire that can be helpful can be downloaded free from info@martinkelleher.co.uk and once this is completed it can provide an appropriate record as well as helping to identify patients who might suffer from phantom bite syndrome.
Once identified, these patients should be referred early on for specialist management, within the secondary care settings, preferably before embarking on extensive dental treatment that will probably not resolve the patient's underlying mental illness condition.