Howe DF, Denehy GE Anterior fixed partial dentures utilizing the acid-etch technique and a cast metal framework. J Prosthet Dent. 1977; 37:28-31
Pjetursson BE, Tan WC, Tan K, Braägger U, Zwahlen M, Lang NP A systematic review of the survival and complication rates of resin-bonded bridges after an observation period of at least 5 years. Clin Oral Implants Res. 2008; 19:131-141
Patsiatzi E, Grey NJ An investigation of aspects of design of resin-bonded bridges in general dental practice and hospital services. Prim Dent Care. 2004; 11:87-89
King PA, Foster LV, Yates RJ, Newcombe RG, Garrett MJ Survival characteristics of 771 resin-retained bridges provided at a UK dental teaching hospital. Br Dent J. 2015; 218:423-428
Botelho MG, Ma X, Cheung GJ, Law RK, Tai MT, Lam WY Long-term clinical evaluation of 211 two-unit cantilevered resin-bonded fixed partial dentures. J Dent. 2014; 42:778-784
Djemal S, Setchell D, King P, Wickens J Long-term survival characteristics of 832 resin-retained bridges and splints provided in a post-graduate teaching hospital between 1978 and 1993. J Oral Rehabil. 1999; 26:302-320
Pröbster B, Henrich GM 11-year follow-up study of resin-bonded fixed partial dentures. Int J Prosthodont. 1997; 10:259-268
Hussey DL, Linden GJ The clinical performance of cantilevered resin-bonded bridgework. J Dent. 1996; 24:251-256
Berekally TL, Smales RJ A retrospective clinical evaluation of resin-bonded bridges inserted at the Adelaide Dental Hospital. Aus Dent J. 1993; 38:85-96
Edelhoff D, Sorensen JA Tooth structure removal associated with various preparation designs for anterior teeth. J Prosthet Dent. 2002; 87:503-509
Craddock HL, Youngson CC A study of the incidence of overeruption and occlusal interferences in unopposed posterior teeth. Br Dent J. 2004; 196:341-348
Porter RJ, Poyser NE, Briggs PF, Kelleher M Demolition experts: management of the parafunctional patient: 1. Diagnosis and prevention. Dent Update. 2007; 34:198-207
St George G, Hemmings K, Patel K Resin-retained bridges re-visited. Part 1. Prim Dent Care. 2002; 9:87-91
Aboush YE, Jenkins CB The bonding of an adhesive resin cement to single and combined adherends encountered in resin-bonded bridge work: an in vitro study. Br Dent J. 1991; 171:166-169
Walls AW, Nohl FS, Wassell RW Crowns and other extra-coronal restorations: resin bonded metal restorations. Br Dent J. 2002; 193:135-142
Hemmings K, Harrington Z Replacement of missing teeth with fixed prostheses. Dent Update. 2004; 31:137-141
Jafarzadeh Kashi TS, Erfan M, Rakhshan V, Aghabaigi N, Tabatabaei FS An in vitro assessment of the effects of three surface treatments on repair bond strength of aged composites. Oper Dent. 2011; 36:608-617
Freilich MA, Niekrash CE, Katz RV, Simonsen RJ The effects of resin bonded and conventional fixed partial dentures on the periodontium: restoration type evaluated. J Am Dent Assoc. 1990; 121:265-269
Lulic M, Braägger U, Lang NP, Zwahlen M, Salvi GE Ante's (1926) law revisited: a systematic review on survival rates and complications of fixed dental prostheses (FDPs) on severely reduced periodontal tissue support. Clin Oral Implants Res. 2007; 18:63-72
Simon JF, Gartrell RG, Grogono A Improved retention of acid-etched fixed partial dentures: a longitudinal study. J Prosthet Dent. 1992; 68:611-615
Emara RZ, Byrne D, Hussey DL, Claffey N Effect of groove placement on the retention/resistance of resin-bonded retainers for maxillary and mandibular second molars. J Prosthet Dent. 2001; 85:472-478
Verzidjen CW, Creugers NH, Van't Hof MA A meta-analysis of two different trials on posterior resin-bonded bridges. J Dent. 1994; 22:29-32
Bassi GS, Youngson CC An in vitro study of dentin exposure during resin-bonded fixed partial denture preparation. Quintessence Int. 2004; 35:541-548
Ibbetson R Clinical considerations for adhesive bridgework. Dent Update. 2004; 31:254-265
Chana HS, Ibbetson RJ, Pearson GJ, Eder A The influence of cement thickness on the tensile strength of two resin cements. Int J Prosthodont. 1997; 10:340-344
Wong TL, Botelho MG The fatigue bond strength of fixed-fixed versus cantilever resin-bonded partial fixed dental prostheses. J Prosthet Dent. 2014; 3:136-141
Gilmour AS Resin-bonded bridges: a note of caution. Br Dent J. 1989; 167:140-141
Ibrahim AA, Byrne D, Hussey DL, Claffey N Bond strengths of maxillary anterior base metal resin-bonded retainers with different thicknesses. J Prosthet Dent. 1997; 78:281-285
Sato Y, Yuasa Y, Abe Y, Akagawa Y Finite element and Weibull analysis to estimate failure risk in resin-bonded retainers. Int J Prosthodont. 1995; 8:73-78
Dahl BL, Krogstad O, Karlsen K An alternative treatment in cases with advanced localised attrition. J Oral Rehabil. 1975; 2:209-214
Dahl BL, Krogstad O The effect of a partial bite raising splint on the occlusal face height. An x-ray cephalometric study in human adults. Acta Odontol Scand. 1982; 40:17-24
Briggs P, Dunne S, Bishop K The single unit, single retainer, cantilever resin-bonded bridge. Br Dent J. 1996; 181:(10)373-379
Poyser NJ, Porter RW, Briggs PF, Chana HS, Kelleher MG The Dahl Concept: past, present and future. Br Dent J. 2005; 198:669-676
Gahan MJ, Nixon PJ, Robinson S, Chan MFW-Y The ovate pontic for fixed bridgework. Dent Update. 2012; 39:407-415
Resin-bonded bridges – the problem or the solution? part 1: assessment and design Jasneet Singh Gulati Sara Tabiat-Pour Sophie Watkins Avijit Banerjee Dental Update 2024 43:6, 707-709.
Professor of Cariology & Operative Dentistry, Hon Consultant in Restorative Dentistry, King's College London Dental Institute at Guy's Hospital, KCL, King's Health Partners, London, UK
Resin-bonded bridges (RBBs) have an important role to play in the minimally invasive prosthodontic replacement of missing teeth. This treatment modality is perceived to have a high clinical failure rate by some practitioners, which may be associated with poorly planned and executed designs and adhesive techniques. This paper, the first part of a two-part series, discusses the important planning stages in the successful provision of RBBs, including assessment, appropriate abutment selection and design considerations. The second part of this series will focus on the clinical stages of RBB provision.
CPD/Clinical Relevance: This paper aims to provide the general dental practitioner with a guide to appropriate case selection and an overview of the planning stages involved for the provision of RBBs.
Article
How long can RBBs last?
Resin-bonded bridges (RBBs) have been used to replace teeth in short edentulous spans with increasing success since the 1970s.1 A systematic review by Pjetursson et al reported a survival rate of 87.7% at 5 years,2 deeming them an acceptable and minimally invasive (MI) method of restoring modest-sized spaces in the dental arch. It has often been considered that they are an under-utilized restoration modality in general dental practice due to a perceived high rate of clinical failure, which may be associated with incorrect design and execution.3
A recent prospective study of 771 adhesive bridges by King et al found that most failures of RBBs occurred within the first four years, and that very few failed thereafter, with an estimated survival rate of 80.4% at 10 years.4 In this single-centre study, because the point of failure was recorded as the first de-bond, the overall survival in clinical service may have been greater where bridges had been re-bonded successfully. An evidence-informed summary of key papers assessing RBBs has been given in Table 1.4,5,6,7,8,9
Authors (Year of publication)
King et al (2015)4 – University of Bristol Dental Hospital and School, United Kingdom
Botelho et al (2014)5 – Faculty of Dentistry, The University of Hong Kong
Djemal et al (1999)6 – Eastman Dental Institute for Oral Healthcare Sciences, University of London, United Kingdom
Pröbster and Henrich (1997)7 – Johannes Gutenberg University, Mainz, Germany
Hussey and Linden (1996)8 – The Queen’s University of Belfast, Northern Ireland, United Kingdom
Berekally and Smales (1993)9 – Adelaide Dental Hospital, Australia
Design of study
Prospective
Retrospective
Retrospective
Prospective
Retrospective
Prospective
Number of RBBs
771
211
832 (including 38 hybrids/movable connector and 199 splint type bridges)
325
142
262 (including 205 ‘Maryland’ bridges 34 ‘Rochette’ bridges of various designs)
Definition of RBB failure
- First de-bond
- Fractured porcelain or metal
- Diagnosis of caries associated with restorations and sealants (CARS)
- Others including aesthetic failure
- First de-bond
- Extraction of the abutment tooth
- First de-bond
- Fractured porcelain or metal
- Diagnosis of CARS
- Others including aesthetic failure and periodontal loss of abutment
- First de-bond
- Loose retainer
- CARS
- Second de-bond
- First de-bond
- Fractured porcelain or metal
- Diagnosis of CARS
- Others including abutment tooth fracture and periodontal loss of abutment
Survival (excluding re-bond data)
80.8% at 5 years80.4% at 10 years
84.4% with a mean life service of 9.4 years
Median survival of 7.83 years
61% at 5 years
88% at 3 years
Median survival of 2.60 years for ‘Maryland’ bridges 70% at 3 years when pontic failures are excluded from failure definition
Survival (including re-bond data)
No re-bonding data
97% at 5 years91% at 10 years84% at 15 years
No re-bonding data
76% at 5 years, 60% after 10 years
94% at 3 years
No re-bonding data
Anterior vs Posterior RBBs (n)
Anteriors (552) Posteriors (219)Posterior RBBs are more likely to fail by an odds ratio of 1.79
Anteriors (111)Posteriors (100)Posterior RBBS are twice as likely to de-bond compared to anterior RBBs
Anteriors (604)Posterior (228)No significant difference in survival
Anterior (279)Posterior (46)No significant difference in survival
Anterior (131)Posterior (11)No comparison made
Anterior (150)Posterior (78)No difference in survival – results were not statistically significant
Cantilever vs Fixed-fixed RBBs (n)
Cantilever (476) Fixed-fixed (295)Fixed-fixed RBBs are more likely to fail by an odds ratio of 2.23
All RBBs were cantilever
Cantilever (171)Fixed-fixed (424)Fixed-fixed RBBs are more likely to fail by an odds ratio of 1.94
All RBBs were Fixed-fixed.
All RBBs were cantilever.
Most ‘Maryland’ bridges were Fixed-fixed (93%).
Unrestored vs Restored Abutments
Unrestored or new restoration (706)Old restorations (65)The presence of an old restoration is associated with higher failure by an odds ratio of 3.21
No comparisons possible
No comparisons possible
Unrestored (236)Restored (89)No influence of presence of restoration
No comparisons possible
No comparisons possible
Preparation vs Non-preparation
Minimal preparation (357)Intermediate or maximal preparation (414)Intermediate or maximal preparation RBBs are more likely to fail by an odds ratio of 2.85
No comparisons possible
No comparisons possible
No preparation (65)Slice-cut, grooves and pinholes, or extensive preparation (260)No significant difference in survival
No comparisons possible
Non-retentive preparation (58)Retentive preparation (170)Non-retentive preparation RBBs are more likely to fail by an odds ratio of 1.82 However, this was not significant when pontic failures were excluded from failure definition
Perforated vs Unperforated Retainer
All retainers were unperforated
All retainers were unperforated
Perforated (105)Unperforated (727)Perforated retainers are more likely to fail by an odds ratio of 1.38
All retainers were unperforated
All retainers were unperforated
Perforated (34)Unperforated (228)Perforated retainers are more likely to fail by an odds ratio of 1.88
Critique of bridge construction protocol
The protocol suggested in this paper is in agreement with our suggested protocol:
- Nickel-chromium alloy of at least 0.7 mm thickness
- Unperforated retainers, air abraded with 50 microns alumina
Abutment teeth were prepared, where necessary, to lower the survey line to increase wraparound of the retainer. This was achieved by axial preparation of the interproximal surfaces. Anterior abutment teeth were prepared with opposing interproximal grooves, however the authors (Botelho et al) suggest this is not currently recommended and not a required tooth preparation feature. Occlusal clearance was created when necessary by preparation of abutment tooth, opposing dentition or both to accommodate a 0.8 mm thick retainer. They used nickel chromium alloy retainers, unperforated, and air abraded with 50 microns alumina. All RBBs were bonded with Panavia EX (Kuraray Co. Ltd, Osaka, Japan) or Panavia 21
The period of study (1978 – 1993) covered many developments of resin-retained cast restorations. Therefore there are many variables in their bridge construction protocol including the choice of resin cement, casting alloy and techniques for metal preparation
The period of study (1984 – 1995) covered many developments of resin-retained cast restorations. Therefore there are many variables in their bridge construction protocol including the choice of resin cement, casting alloy and techniques for metal preparation. A 2-mm distance between framework and marginal gingiva was attempted to be maintained ‘to avoid an adverse periodontal reaction’. Therefore the RBBs in this study did not utilize all available enamel
All abutment teeth were minimally prepared within enamel with a wraparound design and cingulum rests. Nickel chromium alloy used, air abraded with 50 microns alumina prior to fitting. Rubber dam isolation was mandatory. All RBBs luted with Panavia 21. Planned for pontic in light contact in centric occlusion, and protected from loading in excursions
This study used two different alloys for casting, of which both contained beryllium. Beryllium containing alloys are no longer used due to concerns about their safety, and the availability of alternative metal surface conditioning techniques that do not rely on etching. All bridge retainer surfaces were air abraded with 50 microns alumina, followed by electrochemical etching, which is why they are referred to as ‘Maryland’ bridges in this study. The term ‘Maryland’ bridge is therefore historic. Various resin cements were used for bonding, and two different types of pontic; porcelain and light-cured hybrid resin
Careful case selection, appropriate design and attention to operative detail are key factors for the clinical longevity of RBBs and will therefore be covered in this paper.
When can RBBs be used?
RBBs have an important role to play in restorative dentistry, with their indications extending beyond the replacement of lateral incisors. They are a MI way of replacing missing teeth compared to conventional bridgework10 or implants, usually not requiring local anaesthetic, making the procedure suitable for patients who are needle phobic or do not wish to go through lengthy surgical treatment. RBBs are an option where there may be a lack of 3-dimensional space or bone for implant placement. The benefits of shorter appointments and associated cost, compared to conventional bridgework and implant-supported restorations, are also favoured by patients.
However, as with any form of treatment, the use of RBBs is not without limitations and success is associated with appropriate case selection and planning. As with the provision of any restoration, the patient must be well motivated with good oral hygiene and primary dental disease well controlled. The indications and contra-indications are summarized in Table 2.
Indications
Contra-indications
Where abutment teeth are minimally or unrestored, with sufficient enamel present for adhesion
Heavily restored abutment teeth with reduced enamel available for adhesion
Patients unwilling or unsuitable for surgical treatment including implants, bone augmentation
Small abutment teeth, eg peg laterals, microdont teeth with a reduced surface area for adhesion
Fixed retention after orthodontic treatment
Mal-aligned abutment teeth which will result in a poor path of insertion and poor aesthetics
Splinting periodontally compromised teeth to improve comfort, although significant differential mobility may be a contra-indication
Significant differential mobility of abutment teeth where more than one abutment is incorporated in the design, as this frequently leads to de-bond
Needle-phobic patients
Allergy to base metal alloys, eg nickel (although nickel-free alloys exist)
The loss of a tooth can have unwanted changes and effects in the mouth that may complicate the provision of a prosthetic replacement, such as tilting of adjacent teeth or over-eruption of the opposing dentition.11 Therefore, the edentulous space should be assessed for adequate space for an aesthetic pontic and sufficient connector height, not only considering the one arch in isolation, but in both static and dynamic occlusion. A lack of vertical space may require an increase in the occlusal vertical dimension (OVD), which will be discussed in this paper. In cases where the mesio-distal dimension of an edentulous space is smaller than ideal, a RBB may be feasible if aesthetics allow, but implant placement may not be practical.
Post-orthodontic fixed retention can also be incorporated into adhesive bridge design with some success.4 Since the use of RBBs lends itself particularly to the restoration of missing teeth in mild or moderate hypodontia, this is frequently useful in the management of cases where pre-restorative orthodontics has been carried out to create appropriate spaces for replacement of the missing teeth. In Figure 1, the central incisor teeth have been used as abutments with the framework linked to prevent orthodontic relapse. Similarly, where canines have been de-rotated, these may be incorporated in a fixed-fixed design to replace lateral incisors, which would control the position of the canines and prevent orthodontic relapse. An alternative would be to use a cantilever design of an adhesive bridge and provide a separate form of orthodontic retention, such as a vacuum-formed Essix retainer, but this is reliant on patient compliance with regards to retainer wear and is therefore arguably less predictable.
Figure 1. The use of RBBs for post-orthodontic permanent retention. (a) Post-orthodontic labial view of a patient with missing upper lateral incisors. (b) Pre-operative occlusal view, showing electrosurgery preparation of the pontic sites to accommodate a larger pontic and improve aesthetics. (c) Postoperative occlusal view. The metal framework across the upper central incisors is linked to provide permanent post-orthodontic retention. Note the extension of the framework on to the incisal edges of the central incisors. (d) Post-operative labial view.
Consideration of parafunctional habits is important, as fixed prosthodontic work may be more likely to fail where heavy loads are placed on the teeth. The provision of RBBs in bruxists, therefore, requires careful occlusal assessment and planning, as described later in this paper, and consideration may be given to protecting restorative work through the use of an occlusal splint.12,13
Selecting suitable abutment teeth
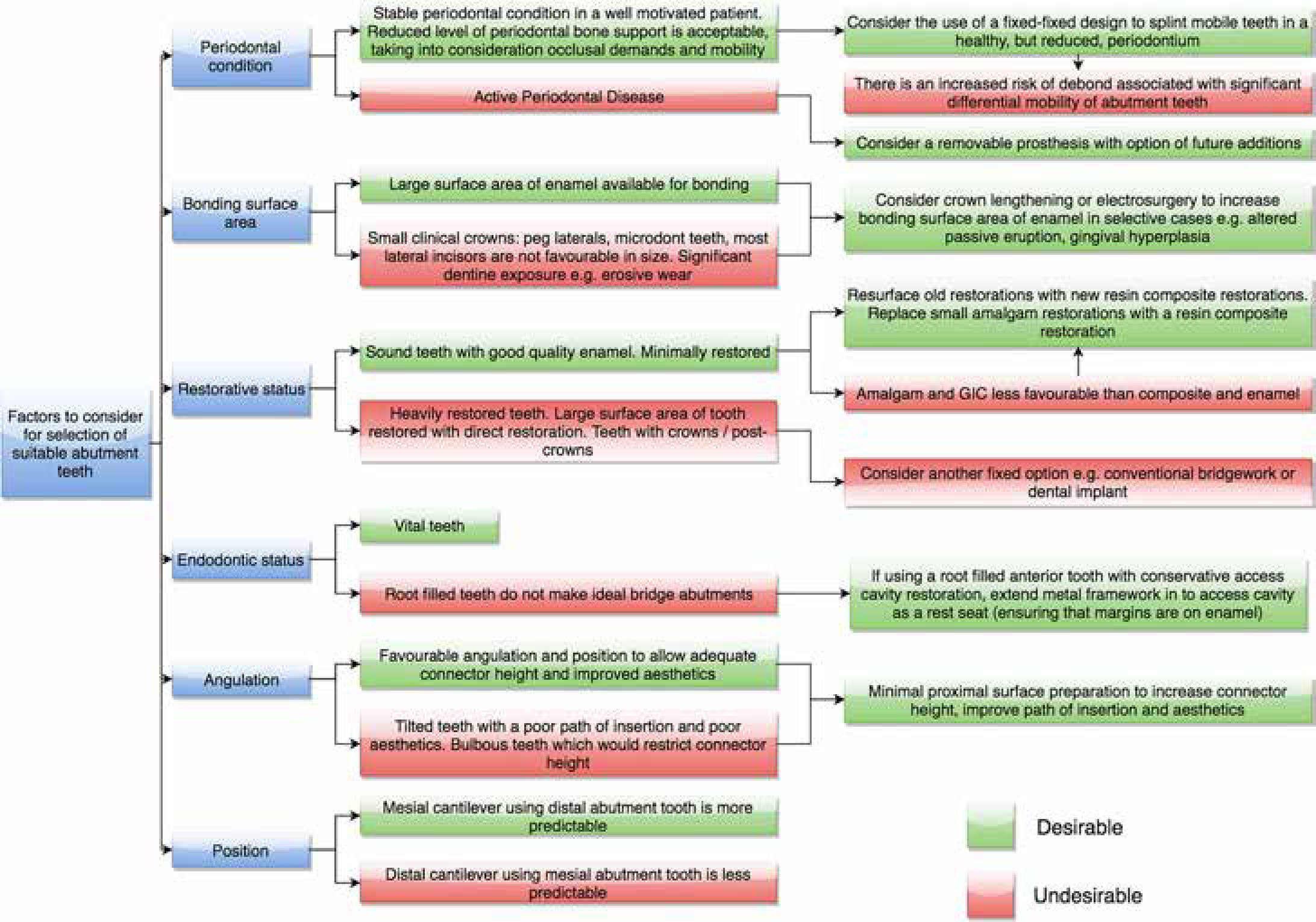
There are multiple factors to consider in the selection of appropriate abutment teeth for RBBs. These are outlined below and also summarized in a flowchart (Figure 2).
Figure 2. A flowchart of various factors to consider in the selection of suitable abutment teeth.
Size
RBBs are ideally suited to the replacement of single units where the adjacent abutment tooth is minimally or unrestored, with sufficient enamel available for adhesion. A large area of enamel allows for a predictable bond to the abutment and is a crucial indicator of success.6 It is therefore desirable that the abutment tooth has sufficient height and width to ensure that a sufficient surface area of enamel is available for bonding and that the retainer design is such that it incorporates the maximum available enamel.
Restorative status
Where potential abutment teeth have existing restorations, it must be borne in mind that the bond strength will be limited by the weakest adherent, with the hierarchy being enamel > resin composite > glass ionomer cement (GIC) > dentine = amalgam.14 It is therefore not ideal to select heavily restored abutments (as these might be better crowned), or teeth where significant amounts of dentine may be exposed, such as in erosive wear cases. However, it may be acceptable to consider a less than ideal abutment tooth where MI conservative treatment and cost-effectiveness are paramount. King et al found that the presence of one or more old restorations on the abutment tooth was associated with a three-fold increase in risk of failure, whereas a new restoration was not significantly more likely to fail than an unrestored abutment.4 Traditional opinion has suggested that old restorations should be replaced with a new resin composite restoration prior to the impression stage.15,16 A more contemporary MI solution is to resurface old resin composite restorations, rather than completely replace them, to ensure conservation of tooth structure. A protocol is outlined in Table 3.
Ensure adequate moisture control. Rubber dam isolation is advised
Use rotary instrumentation to remove uniformly at least 1.0 mm depth of old restoration from the abutment surface
Ensure that a fresh cavity margin of enamel is exposed; ensure removal of residual resin composite, and expose a favourable substrate for better micromechanical/chemical adhesion
Roughen the surface of the resin composite substrate with intra-oral air-abrasion (Microetcher, Danville Engineering Company, IA, USA), or lightly with a fine grit diamond bur if this is not available
Acid-etch the newly prepared enamel margins with 37% orthophosphoric acid (K Etchant Gel, Kuraray Co Ltd, Osaka, Japan) - 20 seconds for enamel (10 seconds for dentine if unavoidably exposed)
Apply primer (Clearfil SE Bond Primer, Kuraray Co Ltd, Osaka, Japan) to the margins where there is freshly cut tooth tissue, wait 20 seconds and gently air dry
Mix primer and silane (Clearfil SE Porcelain Bond Activator, Kuraray Co Ltd, Osaka, Japan) in 1:1 ratio, and apply over old resin composite substrate, wait 5 seconds and gently air dry*
Apply adhesive agent (Clearfil SE Bond Adhesive, Kuraray Co Ltd, Osaka, Japan) onto all cavity surfaces, then dry gently and light cure for 20 seconds
Add resin composite incrementally, light cure and finish
*Clinically, it is difficult to separate the silanation procedure with the adhesive protocol, and it is often omitted for this reason.
Clinical Tip
Replace any small GIC or amalgam restorations with resin composite. Re-surface old resin composite restorations that are otherwise sound. Remember that healthy enamel is the best bonding surface and is critical for the successful provision of RBBs. If there is limited enamel, reconsider the choice of abutment or avoid restoring with a RBB altogether.
Angulation and position
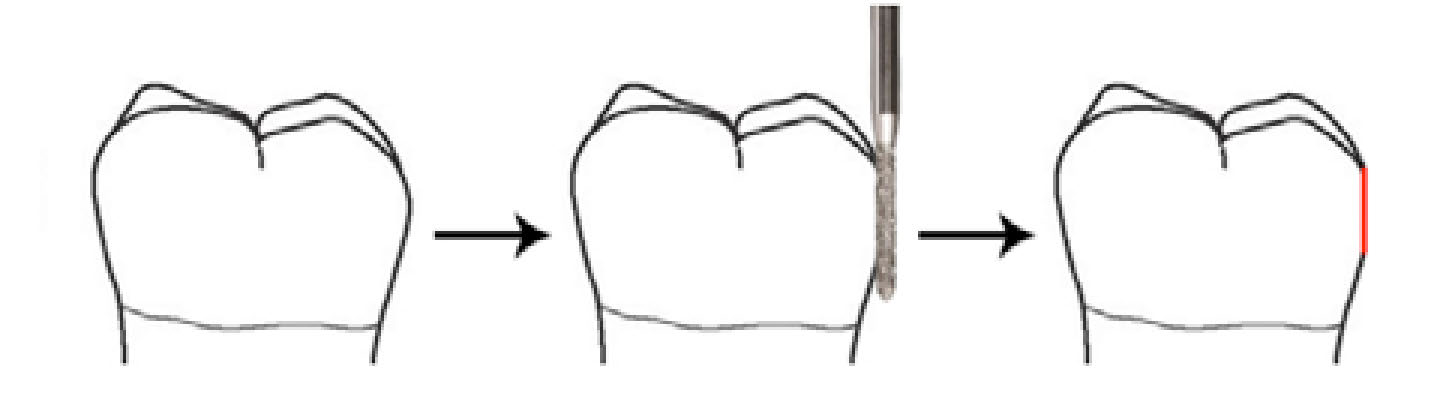
An unfavourably tilted or bulbous abutment tooth crown anatomy may reduce the height of the connector between the pontic and retainer wing, causing an increase in flexibility of the framework. In such cases, consideration should be given to a minimal proximal surface preparation of the abutment to reduce the bulbosity, thereby maximizing connector height to increase rigidity, and allowing the maximum surface area to be incorporated into the design (Figure 3). This also limits the path of insertion, which assists in retention by reducing forces on the cement lute. As well as all these advantages, proximal surface preparation can also reduce the size of embrasure spaces to eliminate black triangles in anterior regions. As with all forms of cantilever bridges, mesial cantilever designs are preferred over distal cantilever bridges. This is due to the increased biomechanical levering forces around the abutment, which acts as a fulcrum.
Figure 3. A diagrammatic illustration of proximal surface preparation to reduce bulbosity, thereby increasing the connector height and rigidity and allowing a suitable path of insertion.
Periodontal status
The presence of an adhesive bridge in itself does not have an adverse effect on the periodontium when compared to other types of restoration.18 It is difficult to define an absolute threshold of periodontal support below which bridgework is contra-indicated, as there is no clinical evidence relating to this. A reduced level of bone support is not necessarily a contra-indication for adhesive bridgework, providing there is no evidence of active periodontal disease and lost periodontal support does not result in excessive mobility. Results of a systematic review by Lulic et al indicated that the long-term prognosis of bridgework using abutments that have severely reduced periodontal support depends on the maintenance of a healthy periodontium.19 The careful control of occlusal force distribution in this cohort of patients is advised.
In well-motivated patients, with plaque control compatible with good periodontal health, RBBs can be used successfully.19 As a practical guide, careful consideration should be given if there is greater than 50% bone loss around the roots. Where bone loss is more than 50% and, especially if there are mobile teeth, the use of a fixed-fixed design to splint the mobile teeth may be considered to improve patient comfort, and ensure that occlusal forces are shared across multiple abutment teeth. To minimize the risk of partial de-bond due to differential mobility of abutment teeth, the RBB must be designed carefully to include abutment teeth that have a similar mobility, both in direction and magnitude. This is especially true for teeth that exhibit more mobility due to a loss of periodontal bone support. It is also worth noting that the use of this technique is particularly technique sensitive, especially at the impression stage, where mobile abutment teeth may be displaced by the impression material, resulting in a poor fit of the framework.
Preparing abutment teeth
Over the years, some literature has suggested that a degree of coronal preparation (such as vertical grooves and preparation of rest seats) of abutment teeth can increase resistance form and thereby longevity of RBBs.9,20,21 However, there is conflicting evidence in relation to this as some studies suggest no benefit of abutment preparation on the overall success of RBBs, and that significant preparation is associated with an increased risk of failure.4,5,6,22 The biological cost of tooth preparation, however minimal, is significant enough to negate the requirement for preparation as there are undeniable advantages of the MI approach, whilst the preservation of enamel for adhesion is important for RBB success. The non-operative approach avoids the risk of exposing dentine,23 which is less ideal as an adhesive substrate and more prone to Caries Associated with Restorations/Sealants (CARS, previously known as secondary or recurrent caries) if the bond fails. There are also complications associated with tooth preparation, such as the need for the preparation to be sufficiently accurate with parallel retention slots/grooves in order for them to be usable or confer any advantage with respect to limiting the path of insertion. The preparation must then be recorded accurately and transferred to the dental laboratory via the master impression and working cast, and for the laboratory to conform the retainer manufacture exactly to the preparation. The loss of detail at each stage may adversely affect the final fit of the RBB and negate any perceived advantage.
One suggested advantage of tooth preparation is that it can create space for the retainer, removing the need for occlusal adjustment of the opposing dentition. However, preparation for this purpose is not advised at the impression stage as it is difficult to provisionalize predictably, risking loss of the created space in the interim between impression and fit appointments due to dento-alveolar compensation and over-eruption.
However, minimal preparation of the abutment teeth to create a guide plane within enamel by removing the natural bulbosity of the clinical crown can assist positive seating of the RBB and increase resistance form by limiting the path of insertion as well as providing the room for an increased connector height (Figures 3 and 4). This is particularly suited for fixed-fixed RBB designs, where the terminal guide planes must be parallel.
Figure 4. Factoring in the connector height of RBBs. The UR2 has been restored with a RBB using the UR1 as a cantilever abutment. Note the difference between the prosthetic UR2 and the natural UL2. The connector height on UR2 is necessary for the framework to maintain rigidity. Note also how this improves aesthetics, however, by eliminating the embrasure space, which might otherwise result in a ‘black triangle’. Note also how the use of opaque cement has eliminated incisal greying of UR1, but that it no longer exhibits the natural incisal translucency that UL1 does.
Clinical Tip
Use a long parallel-sided microfine diamond bur to prepare guide planes where necessary to increase connector height and reduce ‘black triangle’ formation. Be careful not to sink the tip of the bur into the tooth, as this would create a margin, which is not necessary and requires precise adaptation of the metal retainer wing in this area, which is more technically demanding. (Figure 3)
Designing the RBB framework
Degree of coverage
The literature suggests that the best outcome for adhesive bridges can be achieved where maximum enamel coverage is incorporated in the retainer design, and a 180-degree wraparound of the abutment teeth is often recommended.6,24 Incorporating the palatal/lingual cusps and occlusal surfaces of posterior teeth within the retainer wing coverage increases the surface area of enamel for bonding. This also offers some protection against shear forces that would be applied to the cement lute in the axial portions of the retainer wings during function and increases rigidity of the framework, protecting it from dislodging forces.
In anterior cases, extending the retainer onto the incisal edge is advocated as this can assist with location of the retainer, provides a degree of resistance against axial shear forces, and increases the area of bonding further (Figure 5).6 The effect on aesthetics is minimal as when the patient smiles with his/her teeth apart, the retainer extension becomes less visible against the dark background of the oral cavity (Figure 5a). The aesthetic requirements of the patient should also be assessed and good communication maintained throughout the planning and consent stages to ensure that the patient has understood the potential impact that a visible metal wing retainer may have on his/her smile against the perceived advantages associated with this approach. The rationale for maximum palatal coverage and wrapping on to the incisal edge should be made clear to the patient, but in the authors' experience this is often not a problem for the patient. Potential aesthetic failure of RBBs is sometimes described, due to the grey shine through of the metal retainer at the translucent incisal edge, but this can be eliminated predictably by using opaque luting cement.
Figure 5. A case where the RBB retainer has been extended on to the incisal edge. (a) Labial view with the teeth apart, showing the acceptable aesthetic implications of wrapping the retainer on to the incisal surface of maxillary right and left canines. (b) Occlusal view showing the extent of coverage of the retainers. In this case, the patient was unconcerned about the small amount of metal showing and therefore maximum extension was maintained.
The use of an incisal locating tag has been described in cases where retainer location may be difficult, but this can result in inaccurate seating of the retainer, resulting in an increased thickness of luting cement.25 In addition to this, the locating tag must be removed at the fit appointment, which theoretically may compromise the cement lute owing to vibration and heating of the immature material immediately after polymerization. The authors' preference lies with extension of the retainer on to the incisal edge, for the advantages already described.
In addition to the aforementioned advantages of maximum coverage of the framework in RBB designs, there is an additional benefit of full coverage in fixed-fixed RBBs. Stopping short of the incisal edge is contra-indicated in fixed-fixed cases where protrusive and excursive forces beyond the retainer may result in differential movement of the abutment tooth, in effect pushing the tooth away from the framework when two retainers are used. Therefore, the retainer should be full coverage to prevent such a mode of failure in fixed-fixed cases where the excursive guidance may otherwise drive the teeth away from the framework.
Clinical Tip
Incorporate the maximum available enamel for bonding within the framework design. For anterior teeth, this should include the entire palatal/lingual surface, as well as extending on to the incisal edge. For posterior abutments, extend the framework on to the occlusal surface. This also increases the rigidity of the framework.
Number of abutments
The design of choice when replacing a single unit is to cantilever the pontic from a single abutment tooth.15 Fixed-fixed adhesive bridgework has a lower survival rate and there is evidence that they are twice as likely to fail compared to cantilever designs.4,6
Although RBBs are ideally suited for shorter spans, they have also been used successfully for larger spans using a fixed-fixed design.6 Using adhesive bridgework to replace multiple units requires the consideration of additional factors and will therefore require more careful planning. The development of dental implants and their increasing use in routine dental practice means that this treatment option may be selected in preference to adhesive bridgework where multiple teeth are absent. However, MI adhesive bridgework can offer a more cost-effective solution that does not rely on bone availability, and does not involve surgery.
It is acceptable to use a fixed-fixed design to replace teeth in cases where it would be inappropriate to use a cantilever design due to factors such as increased span, occlusal demands and where stability of abutment tooth position is unpredictable. In post-orthodontic treatment cases described above, and in periodontal splinting, it is also more acceptable to use a fixed-fixed design to replace a single unit. However, the differential mobility of a lower canine and lower incisor tooth is such that, as a general rule, the authors avoid incorporating these two teeth in combination as abutments in a fixed-fixed design as, in our experience, this frequently results in de-bond, often at the incisor retainer, and is felt to be too unpredictable. In contrast, in cases where two lower central incisors are absent, a fixed-fixed design retained on the lateral incisor teeth has frequently been used. This makes bonding more straightforward, and the similar mobility of these two abutment teeth both in direction and in magnitude reduces the risk of de-bond compared to the previous scenario.
Due to the differential mobility of abutment teeth in fixed-fixed designs, there is an increased risk of partial de-bond with the bridge remaining in situ, rather than the complete detached failure seen with cantilever adhesive bridges.26 Classically, the fixed-fixed design may fail silently, going unnoticed by the patient. Plaque biofilm stagnation and the ensuing development of caries can occur under the de-bonded wing, especially in cases where dentine is exposed.27 Therefore, in all cases where a fixed-fixed design is used for adhesive bridgework, the patient should be given appropriate advice to be alert to partial de-bond of the framework and caries progression. Patients should be advised to be aware of mobility of the framework, feeling a sharp surface at the margin, food trapping around the framework and a bad taste coming from the bridge as potential signs of a partial bridge de-bond, and should be encouraged to seek prompt dental care.
Similarly, it is important that fixed-fixed adhesive bridges are checked carefully at review as a de-bond is not always obvious on examination.
Framework rigidity
The thickness of the nickel-chromium retainer should be at least 0.7 mm to achieve adequate rigidity within the framework in anterior RBBs.28,29 The longer the span of bridge, the greater the need for rigidity in the framework, as its flexure may lead to bond failure. Rigidity of the framework is therefore paramount for posterior RBBs where the sustained loads are likely to be higher. It is important that this is communicated to the dental technician, as anecdotal evidence suggests that adhesive metal framework is often cast or milled to a thickness of less than 0.5 mm where the thickness has not been specified in the laboratory prescription. Increased rigidity is also achieved by increasing the connector height(s) via proximal preparation and by extending the frameworks over both palatal/lingual and occlusal surfaces.
Using RBBs to replace missing posterior teeth
Due to an ageing population and a change in the pattern of tooth loss, there is likely to be an increase in the number of partially dentate patients in the population. Although accepting a gap is sometimes appropriate, this may lead to unwanted complications such as tilting of adjacent teeth and over-eruption of unopposed teeth, which has been reported to occur in up to 83.9% of cases.11 This may complicate the future restoration of the edentulous space, and may introduce occlusal interferences. Therefore there may be an increasingly significant role that adhesive bridges can play in the replacement of posterior teeth in a MI way in order to maintain tooth position.
There is sometimes cause for concern with using RBBs in the first molar region with regards to design and success associated with the large mesio-distal dimensions of the edentulous space. One option is to replace a first molar with two premolar-sized pontics on cantilevered bridges, using the second molar and the second premolar as abutment teeth. By using two smaller adhesive cantilever bridges to replace one large unit, there is more favourable stress distribution through the framework and a greater surface area of the combined two abutment teeth can be utilized. The alternative option is to cantilever mesially from the second molar tooth, with generous occlusal and lingual/palatal coverage (Figure 6). In most cases the authors prefer a cantilever design in this situation, however, a fixed-fixed design may be accepted to match the increased occlusal demands posteriorly or where there is concern regarding the risk of tilting of the molar abutment (Figure 7).
Figure 6. A posterior cantilever RBB to replace UL5. (a) Post-operative occlusal view showing maximal coverage of the UL6 abutment tooth. (b) Post-operative buccal view of the posterior RBB. Note the extension of the framework over the entire occlusal surface of UL6. No preparation was carried out. The bridge was cemented high in occlusion and occlusal contacts are expected to re-establish in 6–12 months using the principles of the Dahl effect.Figure 7. A fixed-fixed posterior RBB demonstrating the principles of full coverage design. (a) Pre-operative labial view. The upper lateral incisors, upper second premolars and lower second premolars are developmentally absent. The maxillary canines occupy the space of the lateral incisors. Note the inter-occlusal space which can accommodate the framework thickness of the RBB. (b) Post-operative labial view after restorative camouflage of the upper canines using resin composite, and the replacement of all second premolar teeth using fixed-fixed RBBs. (c) Postoperative upper occlusal view. The framework has been designed to be full coverage, including the palatal and occlusal surfaces, which increases surface area of bonding and rigidity of the framework whilst increasing posterior inter occlusal contact for improved masticatory efficiency.
The use of RBBs to replace posterior teeth is less predictable than anterior teeth due to increased occlusal demands.4,5 There is little published evidence assessing the factors associated with success for the replacement of molar teeth with RBBs. However, applying the general principles described previously, the rigidity of the framework, degree of coverage and the occlusion are likely to be important factors for consideration. The extension of the retainer onto the occlusal surface of posterior teeth (Figures 6 and 7) is advised because this incorporates more enamel for bonding and increases the rigidity of the framework. Furthermore, the cement lute is protected from shear forces that could dislodge a bridge that is retained by a retainer wing limited to the axial walls only because the occlusal load is directed onto the occlusal extension, and therefore the cement is loaded in compression.
Occlusion and RBBs
Pre-operative assessment should include examination of the patient's occlusion in the inter-cuspal position (ICP) and in dynamic excursions to ensure that there is enough room for a functional and aesthetic replacement. Ideally, the occlusion should be organized so that the pontic is in light contact in ICP to control the axial position of the opposing tooth, but not involved in guidance, where possible. If guidance on the pontic cannot be avoided, guidance should be shared with the natural teeth, especially where a cantilever design is used. The ICP contact should be kept away from the margin of the retainer. This may be achieved by minimal adjustment of the opposing dentition. It is prudent to warn the patient about this prior to bonding, to reassure the patient that the adjustment is planned rather than a necessity to compensate for a poorly fitting bridge. The use of a facebow transfer to allow casts to be mounted on an articulator, although not always essential for RBB provision, may aid in planning a predictable occlusal scheme in larger span or multiple bridges (Figure 8).
Figure 8. Large span RBB replacing four incisor teeth with careful planning of the occlusal scheme. (a) Labial view showing the incisal wrapover of the canine abutment teeth to increase enamel surface area for adhesion and to assist correct seating of the bridge. The upper central and lateral incisors have been replaced. (b) Occlusal view to show the framework has been contoured to provide occlusal contacts directed axially in ICP.
If pre-operative assessment reveals limited space available for the metal framework, an increase in the OVD can be planned. The bridge can be bonded at an increased vertical dimension, to achieve what is commonly referred to as the ‘Dahl effect’. This should result in relative axial movement as a result of alveolar compensation of the teeth brought out of contact in this way, such that the occlusal contacts re-establish in the weeks or months following bridge placement.30 The technique was initially described using an anterior bite plane to create space anteriorly after a number of months. The mechanism described for the creation of space in an anterior ‘Dahl appliance’ was found to be through a combination of intrusion of anterior teeth (40%), and eruption of unopposed posterior teeth (60%).31 The use of this technique specifically for RBBs has also been described by Briggs et al and is part of the standard protocol for achieving interocclusal space for RBB restorations in our secondary care unit.32
The patient should be pre-warned about occlusal changes and the possibility of transient lisping, and how chewing may feel awkward at first. A review of the literature suggests that the Dahl technique has a high predictability of success (94–100%) and is generally well tolerated by patients.
The average amount of time for contacts to re-establish is 6 months, therefore a longer period of follow-up is advised where this technique is used.33
Clinical Tip
RBBs are frequently bonded high in occlusion. Avoid high static and dynamic contacts that are on the pontic only. The contact should instead be on the retainer wing or shared between the natural teeth and pontic, as should guidance in excursions. Minimal adjustment of the pontic and opposing teeth can achieve this. Warn the patient that this is a planned adjustment and of the potential effects of any short-term disclusion.
RBB pontic design
The pontic should achieve a passive contact with the tissues and allow adequate hygiene by the patient. The two most common pontic designs for bridgework are the modified ridge-lap and the ovate pontic. The potential benefit of ovate over the modified ridge lap is its potentially improved emergence profile and aesthetics. However, the use of an ovate pontic is more technically demanding as it requires planning and possibly the creation of room for the convex portion of the pontic. Where the soft tissue in the pontic bearing area is thick, convex and not compressible, this may be achieved with the use of electrosurgery or, where this is not available, the use of an oval-shaped, diamond bur in a high-speed air turbine handpiece has been described.34 Electrosurgery has distinct advantages for this as it also arrests haemorrhage and allows the master impression to be taken immediately after soft tissue re-contouring and is therefore preferred by the authors.
Clinical Tip
Consider soft tissue modification using electrosurgery to improve the aesthetics and emergence profile of the pontic.
Summary
As with all aspects of restorative dentistry, careful case selection and attention to detail are critical for the successful provision of RBBs. This paper has covered common challenges that practitioners face during planning and designing of RBBs, and hopes to have emphasized the key, evidence-based principles of design that are important for their longevity. The operative techniques involved in RBB provision, including effective laboratory communication, will be covered in Part 2.