Walker A, Cooper I.: Office for National Statistics; 1998
Mensor C. Attachment fixation for overdentures. Part 1. J Prosthet Dent. 1977; 37:366-373
Sherring L, Martin P.London: Quintessence Books; 1994
Ray GE., 2nd edn. Bristol: J Wright; 1969
Jenkins G.London: Quintessence Publishing Co Ltd; 1999
Burns DR, Ward JE. A review of attachments for removable partial denture design. Part 1: Classification and selection. Int J Prosthodont. 1990; 3:98-102
Preiskel HW., 3rd edn. London: Henry Kimpton; 1979
McGivney GP, Carr AB., 10th edn. St Louis: Mosby; 2000
Basker RM, Harrison A, Ralph JP, Watson CJ.London: BDJ Books; 1993
Crum RJ, Rooney GE. Alveolar bone loss in overdentures: a 5 year study. J Prosthet Dent. 1978; 40:610-613
Langer Y, Langer A. Root-retained overdentures: Part II – Managing trauma between edentulous ridges and opposing dentition. J Prosthet Dent. 1992; 67:77-81
Koga DH, Salvajoli JV, Alves FA. Dental extractions and radiotherapy in head and neck oncology: review of the literature. Oral Dis. 2008; 14:40-44
Bureau GP. Tooth-supported stud-retained prostheses: three case reports. Dent Update. 2003; 30:389-396
Shaw MJ. Attachment retained overdentures: a report on their maintenance requirements. J Oral Rehabil. 1984; 11:373-379
Mensor MC. Attachment fixation of the overdenture: Part II. J Prosthet Dent. 1978; 39:16-20
Öwall B. Precision attachment-retained removable partial dentures: Part 1. Technical long-term study. Int J Prosthet. 1991; 4:249-257
Öwall B. Precision attachment-retained removable partial dentures: Part 2. Long-term study of ball attachments. Int J Prosthodont. 1995; 8:21-28
Jackson TR, Healey KW. Rare earth magnetic attachments: the state of the art in removable prosthodontics. Quintessence Int. 1987; 18:41-51
Mensor MC. Removable partial overdentures with mechanical (Precision) Attachments. Dent Clin N Am. 1990; 34:669-681
Walmsley AD. Magnetic retention in prosthetic dentistry. Dent Update. 2002; 29:428-433
Atkin H, Coskun ME, Akin EG, Ozdemir AK. Evaluation of the attractive force of different types of new-generation magnetic attachment systems. J Prosthet Dent. 2011; 105:203-207
Marquardt GL. Dolder bar joint mandibular overdenture: a technique for nonparallel abutment teeth. J Prosthet Dent. 1976; 36:101-111
Precision attachments in partial removable prosthodontics: an update for the practitioner part 1 Gareth Williams Matthew BM Thomas Liam D Addy Dental Update 2024 41:8, 707-709.
Authors
GarethWilliams
BDS, MJDF DipClinHyp, MOrth
Specialist Orthodontist, Total Orthodontics, Brighton
Precision attachments can be used in removable prosthodontics to improve the retention, stability and aesthetics of a prosthesis. Their use is not commonplace. However, when used appropriately, it is possible to construct a more satisfactory prosthesis where conventional partial dentures have previously been unsuccessful. The first of two articles will describe the different types of precision attachments, including intracoronal, extracoronal and radicular. Their relative indications, advantages and disadvantages will also be discussed.
Clinical Relevance: Precision attachments are an option to increase retention in challenging prosthetic cases.
Article
A significant proportion of the United Kingdom is partially edentulous.1 Since the inception of the Adult Dental Health Survey in 1978 the UK has shown a decline in the number of edentulous people. The mean number of teeth observed in the adult population increased from 23 in 1978 to 24.8 in 1998. Between 1988 and 2009, very few adults are reported to have become edentate. In this regard, in 2009, 94% of the combined populations of England, Wales and Northern Ireland were dentate (had at least 1 natural tooth). In 2009, the overall mean number of teeth among dentate adults was 25.7.1 Whilst conventional fixed prostheses and dental implants may be indicated for restoring these edentulous spaces; the removable partial denture is still a commonly prescribed treatment option for patients in the UK. In certain circumstances, optimizing retention, support and stability, with or without compromising aesthetics, is difficult. This can relate to the number of teeth remaining, their distribution and angulations and their restorative status. Precision attachments may improve success if used appropriately.
Precision attachments are not solely used in conventional removable prosthodontics. They are also used in fixed prosthodontics as well as with dental implants. The concept of precision attachments was introduced in Switzerland around 1898 where they were incorporated into retained roots for the retention of overdentures. Approximately 60 years ago, this treatment rationale was popularized by Gilmore.2 Dolder, at the University of Zurich, documented more than 20 years' experience, with over 800 patients who successfully wore bar-fixation dentures.2 Despite their history and development, which includes numerous different types by a variety of manufacturers, their use is often overlooked. This is in part because of cost, but is also due to a lack of understanding of the clinical indications for their use. This article aims to provide an overview of the types of precision attachments available and their indications for use. The second article in this series will consider their clinical application through a collection of illustrated case reports.
Definition, advantages and disadvantages
Definitions for precision attachments include the following:
A precision connector is made up of two or more parts. One part is connected to a tooth, root or implant. The other part is connected to a prosthesis.3
Precision attachments are whole or partly machined accessories used in dentistry for the retention of removable or semi-removable prostheses. In most cases they take the form of articulated joints.4
Precision attachments offer potential advantages in restorative dentistry, particularly in removable prosthodontics. In spite of this, their use in general dental practice tends to be limited.5 In general, the uses of precision attachments in dentistry are for bridgework: intracoronal and extracoronal attachments can be used to overcome the problem of non–parallel abutments; partial dentures, including free-end saddle dentures (unilateral and bilateral); overdentures and implants.
The advantages of precision attachments in removable partial denture design include:
The potential to improve aesthetics by avoiding visible retainers in the aesthetic zone;
Improved retention, support and stability;
Facilitating the management of divergent abutments;
Enabling more direct apical loading compared with occlusal or incisal rests, thus shortening the lever arm of a saddle and minimizing torque forces;
There are several disadvantages associated with precision attachments. These include:
The cost associated with the increased laboratory work and the attachments themselves;
The necessity to prepare abutment teeth;
If space for the attachment is not assessed appropriately then plaque control can be difficult for patients;
A minimum 4 mm of vertical interocclusal space is required for most attachment systems. This can mean the need for a greater level of maintenance with an appropriate hygiene regimen.
The complex nature of an attachment can mean that the path of insertion is difficult for patients. Some attachment systems make repairs or alterations difficult or impossible.6
These disadvantages need to be clearly considered before treatment planning precision attachments. They also emphasize the importance of case selection.
The literature contains several classification systems for attachments. This seems to be due to a potential for category overlap, along with the fact that many of these attachments can be classified in different ways, for example the position of placement, material, accuracy of fit, appearance and flexibility. Below is a classification which is deemed the simplest for the purposes of this article and is adapted from several sources.4,5,7
Classification of precision attachments
Precision attachments can be classified according to:
The sub-categorical classification based on rigidity merits further discussion. Rigid attachments are those that theoretically allow no movement of their component parts during function.6 Clinically, however, micromovement does occur during function, with the amount of movement being a function of the degree of wear of the components.6 The resilient attachment allows a precalculated amount of movement when the attachment is fully seated. The movement is usually of a hinge type and serves to distribute potentially harmful forces towards the saddle and away from abutment teeth.5,6 These are especially indicated in tooth-and mucosa-borne dentures associated with large edentulous spans.
When classified by design, this is related to the benefits they provide. Precision attachment is a term used generally for those units that provide benefits in terms of support, retention, reciprocation (bracing) and stability. The term semi-precision attachment is reserved for those intracoronal attachments with tapered sides. These attachments will supply a similar degree of support, but cannot be relied upon for retention and reciprocation.7 This is due to the fact that the fabrication methods for semi-precision attachments yield a less precise tolerance.6 Resilient attachments provide a more defined and predetermined amount of movement in their component parts, permitting functional movement of the denture base towards the ridge during function, theoretically reducing stress on the dependent abutment. It is in this way that the semi-precision attachment acts as a ‘stress director’.6
This article will deal with the former classification, by location, and specifically in relation to removable prosthodontics.
Intracoronal attachments
These consist of two parts, one part joined to the removable prosthesis (flange or patrix) and one part embedded in the restoration (slot or matrix). The two units are linked intra-orally.7 Intracoronal attachments ideally should be completely incorporated within the contour of the crown (Figure 1). This is advantageous because the occlusal forces are then applied close to the long axis of the tooth. If the tooth is underprepared, then an overcontoured crown is produced placing part of the intracoronal attachment outside the natural crown contour, thereby losing this perceived advantage. The size of the tooth, the size of the pulp and the chosen attachment will all influence this. This advantage has to be offset against the degree of preparation required so as not to cause loss of too much tooth structure or vitality. These attachments usually require a box preparation in line with the manufacturer's instructions. It is often useful to have a plastic model or the actual attachment nearby, so that a try-in may be performed and the clinician can be assured of adequate reduction to house the attachment. It will also act as a guide prior to preparation to ensure that its choice is appropriate relative to the tooth and pulp size; minimizing the risk of irreversible pulp damage.5 All intracoronal attachments are rigid. This can make insertion and removal more difficult for patients.
Figure 1. Diagram of intracoronal attachment.
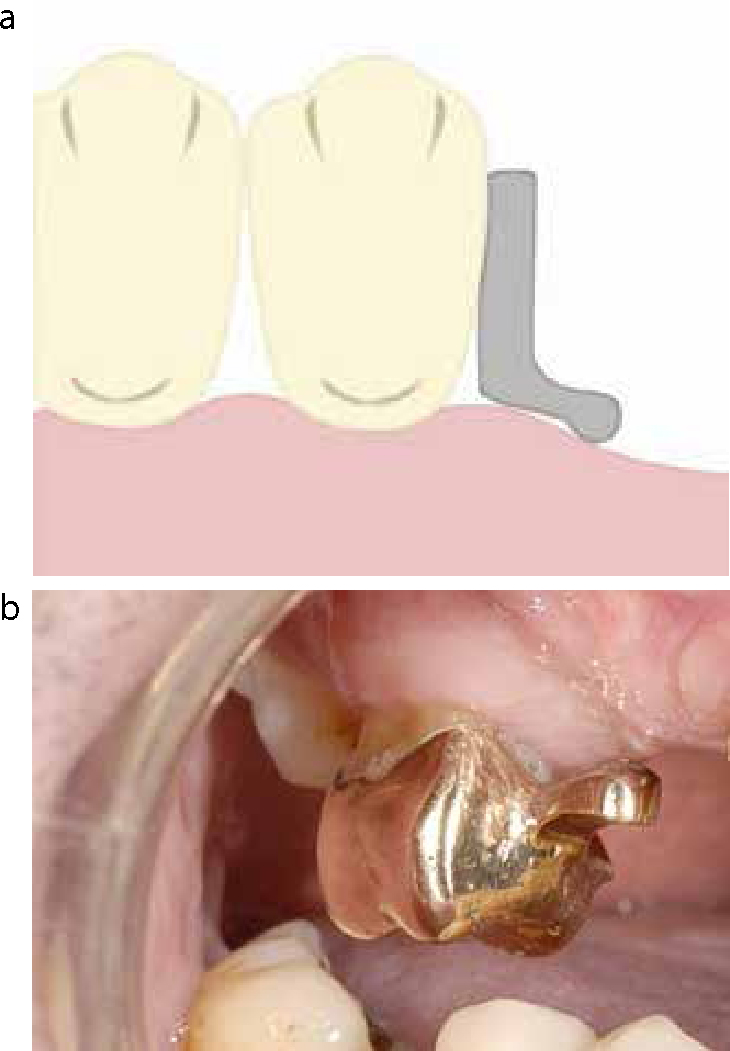
Extracoronal attachments
This term is best defined as those units having part or all of their mechanism outside the contour of a tooth (Figure 2). Commonly, these attachments have their main application with distal extension prostheses, but may be used in bounded saddles.7 The advantage of this type of attachment is that tooth reduction is less than an intra-coronal attachment, minimizing tooth reduction. One disadvantage is that maintaining hygiene below the attachment can be more difficult (Figure 3). This depends on the height of the tooth, the dimension and shape of the attachment used and the contour of the soft tissue adjacent to the edentulous span. It is important to provide the patient with specific oral hygiene instruction to overcome this problem. This should include the use of superfloss or interdental brushes, so enabling adequate plaque removal. In free-end saddle situations, for example, it may be advantageous to use a cantilever pontic unit with the attachment on the pontic to allow for soft tissue clearance (Figure 4). For patients with limited dexterity, insertion and removal is often easier with extracoronal attachments compared with intracoronal attachments. Since teeth retaining extracoronal precision attachments can be subject to considerable torque (especially if opposing teeth are natural), it is suggested that distal facing attachments in free-end saddle situations be retained by two or more crowns (double abutted) to resist these adverse forces.5 The disadvantages of this approach is the additional tooth preparation, difficulties in interproximal cleaning and therefore risk of caries or periodontal disease. Individual circumstances need to be considered, such as root size and shape, as well the size of the crown and the opposing occlusion before committing to a double abutment construction. Extracoronal attachments can be either rigid or resilient.5
Figure 2.
(a) Diagram of extracoronal attachment. (b) Ceka (CEKA Alphadent NV, Belgium) extracoronal attachment.Figure 3. Extracoronal attachment showing very little space between attachment and tissues. This can be difficult for patients to keep clean.Figure 4. Extracoronal precision attachment cantilevered distally from double abutted crowns. The receding ridge creates more room for the precision attachment and does not encroach on the cervical papilla on the posterior abutment.
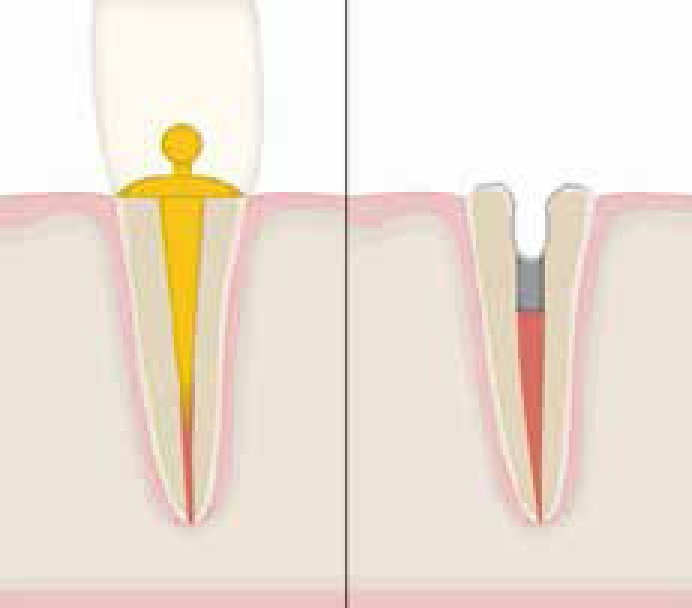
Radicular attachments
By definition, radicular precision attachments are connected to a root preparation (Figure 5). These have been shown to improve the retention of removable partial dentures significantly.8 Their use can minimize the need for retention and stability components in aesthetic areas.9 The majority are soldered or cast to a coping, although there are pre-formed ones available. The use of pre-formed ones could be limited as there is no scope to change their angulations. It is critical that an assessment of the vertical height of both the attachment and coping is made so that there is sufficient space for the denture tooth. Case selection is important not only with respect to attachment choice, but also in relationship to root length, root morphology and quality of endodontic treatment. An appropriate length post is required to resist decementation on removal of the prosthesis. This has become less of a problem more recently with the availability of adhesive cements.
Figure 5. Root face attachments: extra-radicular and intra-radicular.
Retained roots provide many advantages, even when not restored with precision attachments.10 Their maintenance continues to provide proprioceptive feedback, support psychological benefits of tooth retention and tactile sensitivity discrimination to the patient. Crum and Rooney, in 1978, used lateral skull radiographs to assess quantitatively vertical alveolar bone loss in lateral skull radiographs to compare edentulous and overdenture patients with retained canine teeth. A mean loss of 5.2 mm mandibular alveolar height was reported for the edentulous group, whereas the comparable mean for the overdenture group was 0.6 mm.11 The problem of combination syndrome can be avoided if roots are maintained.12 The maintenance of roots has also been advocated in patients who have had radiotherapy to reduce the risk of osteoradionecrosis following tooth extractions.13
The use of radicular precision attachments in retained roots offer additional advantages.8 Those that are soldered onto gold copings cover the root face and provide protection of the root face from caries. If ferrule production is possible, they can resist stresses which may propagate vertical root fracture.8 Some systems enable the level of retention to be modified. This can allow retention to be increased or decreased depending on the patient's needs.
There are, however, disadvantages when using teeth for overdentures, and these include problems of plaque retention, secondary caries, endodontic problems and the need for continuing care and maintenance. Once again, case selection is critically important as the dexterity of the patient should influence the choice of radicular attachment.14,15,16,17 Like all the aforementioned classified precision attachments, their disadvantages include cost and technical demands. In addition to these, the bulk of the attachments need to be considered, not only in height, but also mesiodistally. Not considering these can leave insufficient space to house the component that is encased in the denture. This can cause a potential weakness of the prosthesis, which may be more susceptible to fracture. It is always sensible, therefore, to do a tooth try-in to assess space in all dimensions before choosing an attachment. Table 2 highlights the heights of a number of commonly used attachments.
Attachment Name
Height of Attachment (mm)
Extracoronal
Dalbo – S
5
Mini Dalbo
3
Hinge
4.5
Ceka Revax
5
Anchors/Bars (Dimensions do not include root face coping or space for prosthetic tooth)
Rothermann Eccentric
1.1 (rigid); 1.7 (resilient)
Dalbo Anchor
4
Rigid Dolder Bar
3.5
Ceka Axial
2.7
Öwall found that the long-term results for intra-radicular stud retained removable partial dentures were favourable.18 At 10 years, the success rate was reported to be 70% and at 15 years 60%.18
Various types of radicular attachment exist, these include:
Anchor (stud) types: these are among the simplest of all attachments.7 The matrix or patrix is soldered to a root surface coping. Intra-radicular attachments have their matrix prepared into the root surface with the patrix slotting into the root form contour, whereas extra-radicular attachments have the patrix attached to the root preparation. Examples of intra-radicular attachments are the Zest, and extra-radicular are the Ceka Axial or Rothermann eccentric (Preat, Grover Beach, CA USA). Both Rothermann eccentric and Ceka axial attachments have rigid and resilient variants (Figure 6).
Magnetic attachments: these adopt a similar principle but, instead of a mechanical matrix and patrix, the root diaphragm and prosthesis contain magnets of opposite polarity. Case reports have shown this to transfer less lateral root force to the abutment root.19 Advocates of magnets would argue that they provide a constant retention factor, and are independent of wear, in contrast to mechanical precision attachments.20 Magnetic retention is simple to use, although these attachments exhibit the problem of potential intra-oral corrosion.21,22 New magnets show promise in circumventing this problem.22 They also tend to require less vertical space. Modern magnets, such as the Neodymium/Boron/Iron alloy magnets, provide good attachment force in combination with small dimensions (Figure 7).
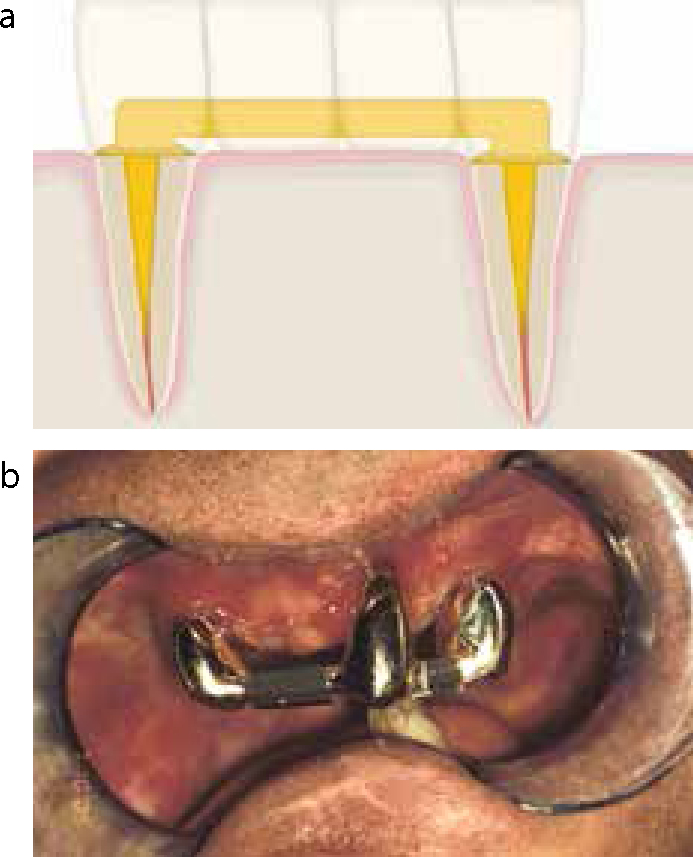
Bar attachments: the Ackerman bar is one of the most popular prefabricated models.5 These attachments span an edentulous space and connect removable prostheses, roots, abutment teeth or implants (Figure 8). Bar attachments, to a limited degree, can be used with divergent root canals to overcome angulation problems.23
Figure 6.
(a) Rothermann attachment; (b) Ceka attachment.Figure 7. Root face magnets.Figure 8.
(a, b) Bar type attachment.
This category contains a large collection of miscellaneous items. For this reason, only those most commonly used will be detailed here:
Screw and tube;
Key and Keyway;
Presso-Matic (Metalor Dental Products Ltd, London) or Ipsoclip (Cendres + Métaux UK Ltd, Cheshire);
Sectional dentures.
Screw and tube attachments consist of a screw with a tapered head and threaded tube. A collar for the screw may be incorporated into the design. These attachments are for connecting prostheses and allowing contingency planning of long span bridgework. Removal of these screws would allow removal of a bridge suprastructure and examination or treatment of supporting abutments. Their brief discussion warrant mention as they facilitate removal rather than retention of prostheses. The other auxiliary attachments fall outside the scope of this article.
Conclusion
The success of partial dentures is primarily dependent upon sound prosthetic principles; the selection and design of precision attachments should be based around these, not vice versa. With so many different systems on the market, it is better to be fully aware of a small number and to be clinically competent at using them, rather than have knowledge of many systems. It is also equally important to work with a technician who is knowledgeable in their use. Knowing when to use the appropriate one is fundamental to their long term success. In the second article, these clinical considerations will be illustrated with appropriate cases.
All precision attachments require a varying amount of vertical height (Table 2). It is critical in the planning that there will be enough space for the vertical height of the attachment, along with 1–2 mm clearance from the occlusal level, so the attachment is completely housed within the denture and therefore not subject to undue stress, which might lead to early failure. Adequate tooth preparation can be ensured by having a tooth try-in stage prior to committing to a particular attachment.